
Abstract
Introduction:
Elderly patients intrinsically have higher bleeding risks, deterring clinicians from prescribing them oral anticoagulants. Setting a narrow international normalized ratio (INR) target range might potentially mitigate some of these risks. This study sought to compare the outcomes of elderly patients who were assigned to either a narrow INR target range or the conventional INR target range in a real-world environment.
Methods:
This was a retrospective cohort study with the primary and secondary outcomes being the mean percentage time above INR 3.0 and the mean percentage time below INR 2.0 and the incidents of bleeding and thromboembolism associated with oral anticoagulant therapy, respectively. Patients and health care workers managing them had no prior knowledge of this study.
Results:
Data of 150 patients with a narrow INR target range (2.0-2.5) and 164 patients with a conventional INR target range (2.0-3.0) were collected and analyzed. The narrow INR group had significantly higher underlying risks of bleeding than the conventional INR group. Patients in the narrow INR group had a significantly lower percentage time above INR 3.0 but no significant difference in the percentage time below INR 2.0. Adjusted incidence rate ratio (IRR) for bleeding events was significantly lower for the narrow INR group, while the adjusted IRR for thromboembolic events between both groups was similar.
Conclusion:
Patients assigned to a narrow INR target range in real-world practice spent a significantly lower amount of time below an INR of 3.0 compared to conventional INR target range with lower incidents of bleeding complications and no increase in subtherapeutic INRs.
Introduction
Oral anticoagulant therapy with warfarin is widely used for the primary and secondary prevention of venous and arterial thromboembolic events. Its effectiveness has been consistently demonstrated in various settings, 1 but a narrow therapeutic index and wide-ranging interactions with food and drugs make managing patients on warfarin a challenge. Overanticoagulation with warfarin can result in serious hemorrhage, while underanticoagulation can lead to recurrent thromboembolic events. 2 As such, regular monitoring and warfarin dose adjustments are necessary to maintain patients within their specified therapeutic target.
The intensity of anticoagulation, represented by the international normalized ratio (INR) target range, depends on the indication for warfarin therapy. International guidelines recommend specific INR target ranges for different indications, 3 –5 the most common being an INR target range of 2.0 to 3.0. This conventional INR target range was found to have the lowest rate of a composite outcome of major hemorrhage and thromboembolism. 2 Studies have also identified other factors that might affect the safety and efficacy of warfarin therapy. Among them, advanced age was consistently shown to be an independent risk factor for both bleeding and thromboembolism. 6 –10 These concerns might deter clinicians from prescribing warfarin to elderly patients, adversely affecting their survival outcomes and quality of life. 11,12
To minimize the risk of bleeding, it has been suggested that older adult patients should have a “low INR target zone”, coupled with close INR monitoring. 7 However, INR target ranges below 2.0 were associated with poorer efficacy, with no significant improvements in safety in clinical studies. 13,14 Alternatively, a narrow INR target range that falls within the lower spectrum of the conventional INR target range might improve the safety profile of anticoagulation, without compromising efficacy.
At our institution, a conventional target range of 2.0 to 3.0 was assigned to older adult patients as a standard of practice. However, over the past 5 years, a select number of hematologists preferred assigning their patients aged 65 years and older to a narrower preset target range of 2.0 to 2.5. Their aim was to actively keep older patients at the lower spectrum of the conventional INR target range, thus minimizing the percentage of time spent at higher INR values. This target range was reported to have the lowest incidence of stroke and intracranial hemorrhage while providing adequate anticoagulation. 14
The dichotomous practice of setting different INR target ranges for older adult patients by individual physicians in our hospital has resulted in 2 distinct sets of patients managed at narrow and conventional INR targets. We therefore sought to find out whether this practice of setting a narrow INR target was indeed beneficial for patients in terms of reducing the incidence of bleeding complications, without reducing efficacy.
Methods
Study Design and Population
This was a retrospective cohort study conducted at the Singapore General Hospital, a 1500-bed academic medical center. A list of patients on warfarin, followed up at the outpatient pharmacist-assisted anticoagulation clinic (ACC), was retrieved from an electronic anticoagulation database (Dawn AC, 4S Information Systems Ltd, Milnthorpe, United Kingdom). Patients with an INR target range of either 2.0 to 2.5 or 2.0 to 3.0 between September 1, 2007, and August 31, 2012, were identified. Assignment to either group was done on therapy initiation or modification, in a nonrandomized manner, depending on clinical judgment and physician preference.
Patients were eligible for this study if they were aged 65 years or older at the start of the study period and had a labeled indication for warfarin. This included patients who were initiated on warfarin in the wards, stable upon discharge, and subsequently referred to the outpatient ACC as well as those who had been on warfarin for some time. Patients were excluded if they were receiving warfarin for mitral valve replacement or for an unlabeled indication, were prescribed more than 1 INR target range, had less than 2 INR readings during the study period, or were lost to follow-up.
All patients in our ACC were first reviewed by a hematologist who verified their indications and set the INR target ranges. These patients were then subsequently seen by pharmacists with a review by a hematologist annually and whenever predefined triggers or complications occurred. The ACC had practice protocols for its pharmacists on warfarin dose adjustments and recommended intervals between visits. The usual monitoring of these 2 groups of patients was, however, not differentiated in our protocol, since the study was not preplanned. This study was approved by our institution’s Centralized Institutional Review Board.
Data Acquisition
A data acquisition form was created to collect demographic information (age, gender, smoking status, and alcohol consumption), past medical history, current medical conditions, and existing comorbidities from patients’ case notes and the electronic admission database. Indications for oral anticoagulant therapy, prescribed INR target range, and treatment duration were retrieved from patients’ case notes and computerized patient databases. The INR readings were retrieved from electronic results issued by our clinical laboratory. Hospitalization events during the study period were collected from patients’ case notes and electronic admission database. All data were extracted and verified by pharmacists.
Definitions
Labeled indications of warfarin include the prophylaxis or treatment of deep vein thrombosis, pulmonary embolism, chronic atrial fibrillation (AF), and rheumatic heart disease. Indications that did not fit the above-mentioned criteria were considered as unlabeled indications. 15
Only INR readings taken at the outpatient ACC within the study period were considered for this study. The duration between the first INR reading and the last INR reading within the study period was defined as the duration of follow-up. Patients with a treatment duration of 90 days or lesser were defined as new patients because published data suggested a higher risk of bleeding in the first 3 months of anticoagulant therapy. 7 Patients who were prescribed the INR target range of 2.0 to 3.0 were classified as the conventional INR group while those with a target range of 2.0 to 2.5 were classified as the narrow INR group. In each group, the number of ACC visits was also recorded. The HAS-BLED bleeding risk score, 16 originally intended for patients with AF, was adapted to assess the risk of bleeding in all patients. The CHADS-VASc score was used to assess the risk of stroke in patients with nonrheumatic AF. The presence of established thromboembolic risk factors was captured for every patient. 17
Safety of warfarin therapy may be assessed from the incidence of bleeding complications, while efficacy of therapy can be determined from the incidence of thromboembolic complications. However, due to the expected low incidence of events in this setting, percentage time above INR 3.0 and below INR 2.0 were used as surrogate markers for bleeding and thrombosis, respectively. 18 These were computed based on the Rosendaal linear interpolation method. 19
Bleeding and thromboembolic events that resulted in the hospitalization of the patients were classified into 3 categories (major bleeding, minor bleeding, and thromboembolism). Major bleeding was defined as fatal or clinically overt bleeding associated with either transfusion of 2 or more units of blood or a ≥2 g/dL decrease in hemoglobin or bleeding involving a critical anatomic site (intracranial, intraspinal, intraocular, retroperitoneal, intra-articular, pericardial, or intramuscular with compartment syndrome). Clinically overt bleeding not satisfying the criteria for major bleeding was classified as minor bleeding. 20
Thromboembolism referred to incidents of ischemic stroke, recurrent deep vein thrombosis (DVT), pulmonary embolism, and other thromboembolic events. Events that did not result in a visit to the emergency department or hospitalization were not captured.
Outcomes
The primary outcome for this study was the mean percentage time above INR 3.0. The secondary outcomes of this study were the mean percentage time below INR 2.0 and the incidents of bleeding and thromboembolism associated with oral anticoagulant therapy.
Statistical Analysis
The Cohen’s standardized effect size was used to estimate the sample size required. This method has been shown to be robust in estimating the sample size required when the effect size cannot be determined from previous studies. 21 In order to detect a low to moderate effect size in the primary end point (ie, Cohen standardized effect size of 0.35) with 80% statistical power, a sample size of 130 per group was required.
Nominal variables were expressed in numbers (%), and comparisons were done using chi-square test. Ordinal variables were expressed in median (interquartile range), and comparisons were done using Mann-Whitney U test. The primary outcome (ie, percentage time above INR 3.0) and other continuous variables were expressed in mean (standard deviation [SD]) and compared using 2-sample t test. Multiple linear regression of the primary outcome was subsequently employed to adjust for potential confounders. Negative binomial regression was used to compare the incidents of bleeding and thromboembolic complications between both groups and presented as incidence rate ratios (IRRs). The IRRs were adjusted for potential confounders. All analyses were performed using SPSS (version 18.0.1, released 2009; SPSS Inc, Chicago, Illinois), with the level of statistical significance set at 5%.
Results
Patient Characteristics
A total of 150 patients were identified in the narrow INR group and 164 patients in the conventional INR group. Majority (53.3%) of the patients in the narrow INR group were 75 years and older, while the majority (76.2%) of patients in the conventional INR group were aged between 65 and 74. This resulted in a significantly higher mean age in the narrow INR group of 75.71 (6.23) years compared to the conventional INR group of 71.74 (5.21) years (P < .05). Hypertension, hyperlipidemia, diabetes mellitus, and previous history of stroke were the most common comorbidities in both the groups. Patients placed in the narrow INR group had more comorbidities and past medical history such as renal impairment, liver impairment, hypertension, previous stroke, previous transient ischemic attack, and anemia than patients in the conventional INR group. Antiplatelet agents were the most common concurrent medication in both the groups. Proportion of new patients between both groups was similar (Table 1).
Patient Demographics.
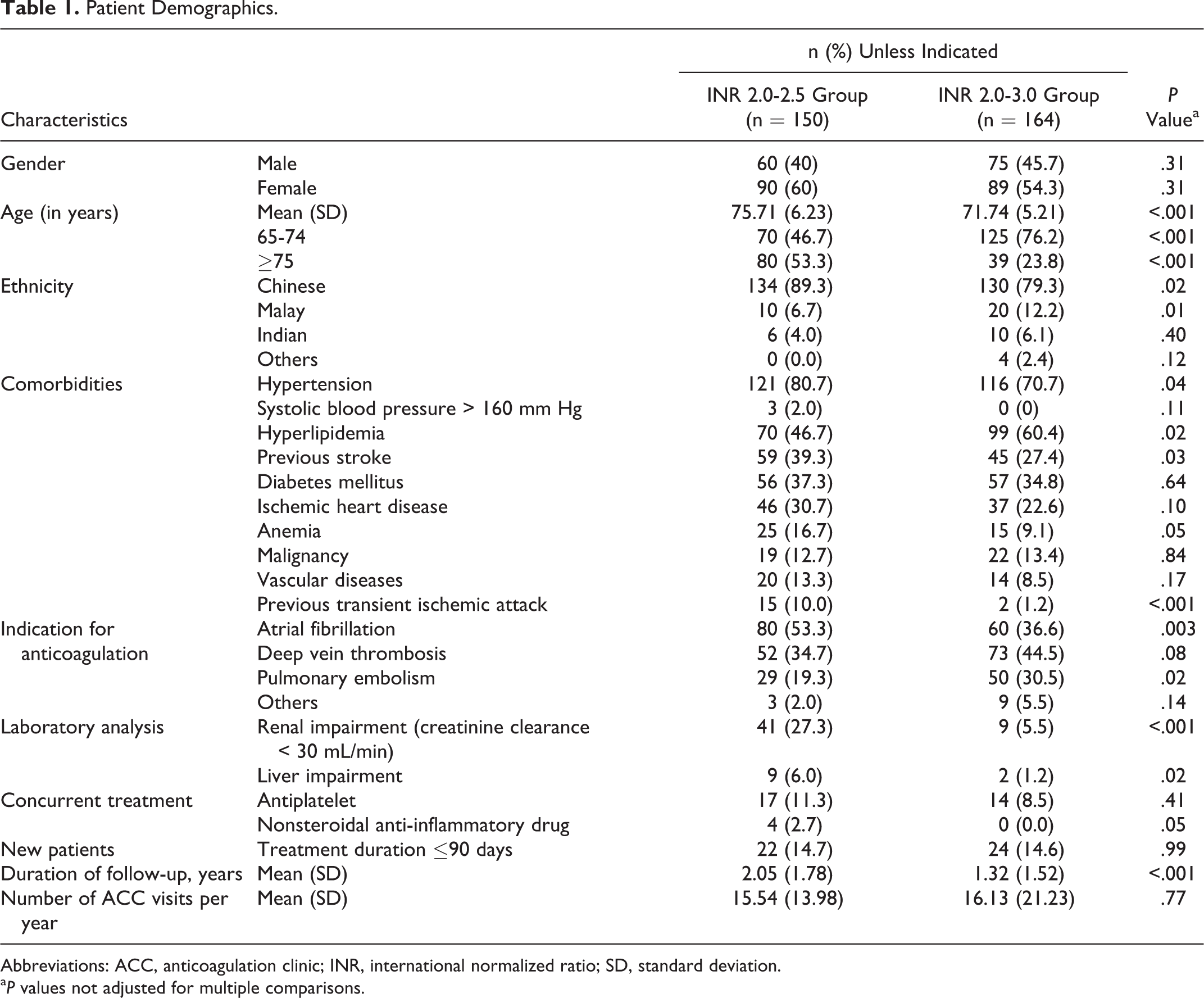
Abbreviations: ACC, anticoagulation clinic; INR, international normalized ratio; SD, standard deviation.
a P values not adjusted for multiple comparisons.
The distribution of indications for anticoagulant therapy in each group was different, and some patients presented with more than 1 indication. In the narrow INR group, 53.3% of patients were receiving anticoagulant therapy for the management of AF, while 34.7% of the patients were receiving it for the management of DVT. This was in contrast to the conventional INR group, where the majority (44.5%) of the patients were on warfarin for the management of DVT while only 36.6% of the patients were on it for AF. Pulmonary embolism was more prevalent in the conventional INR group (30.5%) than in the narrow INR group (19.3%).
The HAS-BLED score classified 100 (66.7%) patients in the narrow INR group and 41 (25.0%) patients in the conventional INR group as having a high risk of bleeding (score ≥ 3). The remaining patients were classified to have a low risk of bleeding. The median HAS-BLED score was significantly higher in the narrow INR group (3.0 [2.0-4.0]) than the conventional INR group (2.0 [1.5-2.8]; P < .05; Table 2).
HAS-BLED Scores.
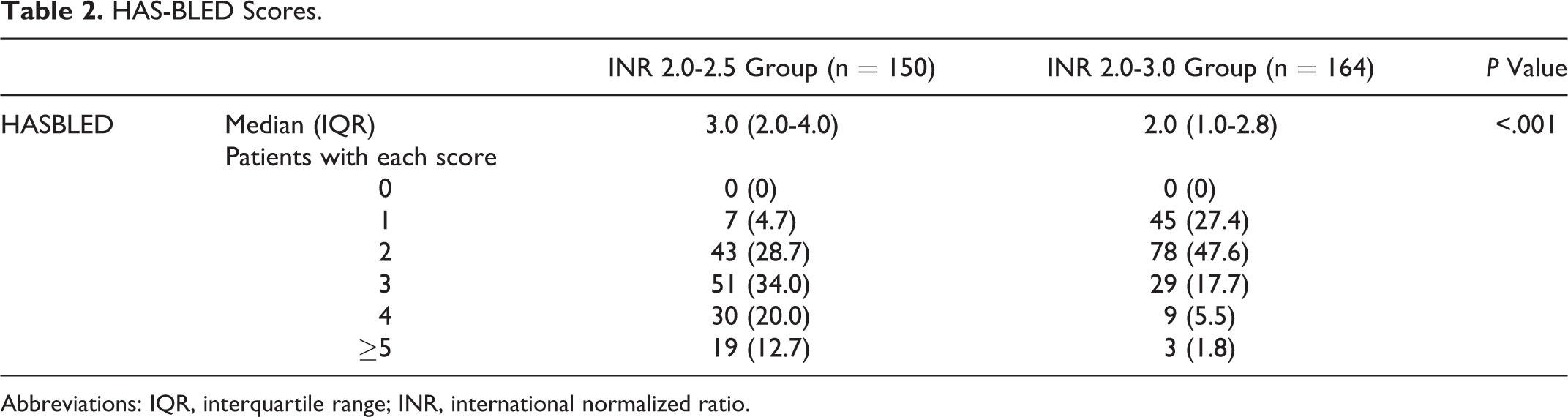
Abbreviations: IQR, interquartile range; INR, international normalized ratio.
The median CHADS-VASc score was significantly higher in the narrow INR group (5.0 [4.0-6.0]) than the conventional INR group (5.0 [3.0-6.0]; P = .005; Table 3). The narrow INR group had a larger proportion of patients who had a history of trauma (9.3% vs 1.8%) but a smaller proportion of patients who had a history of venous thromboembolism (45.3% vs 65.9%) and immobility (0.7% vs 7.3%) compared to the conventional INR group (Table 4).
CHADS-VASc Scores for Patients With Atrial Fibrillation.
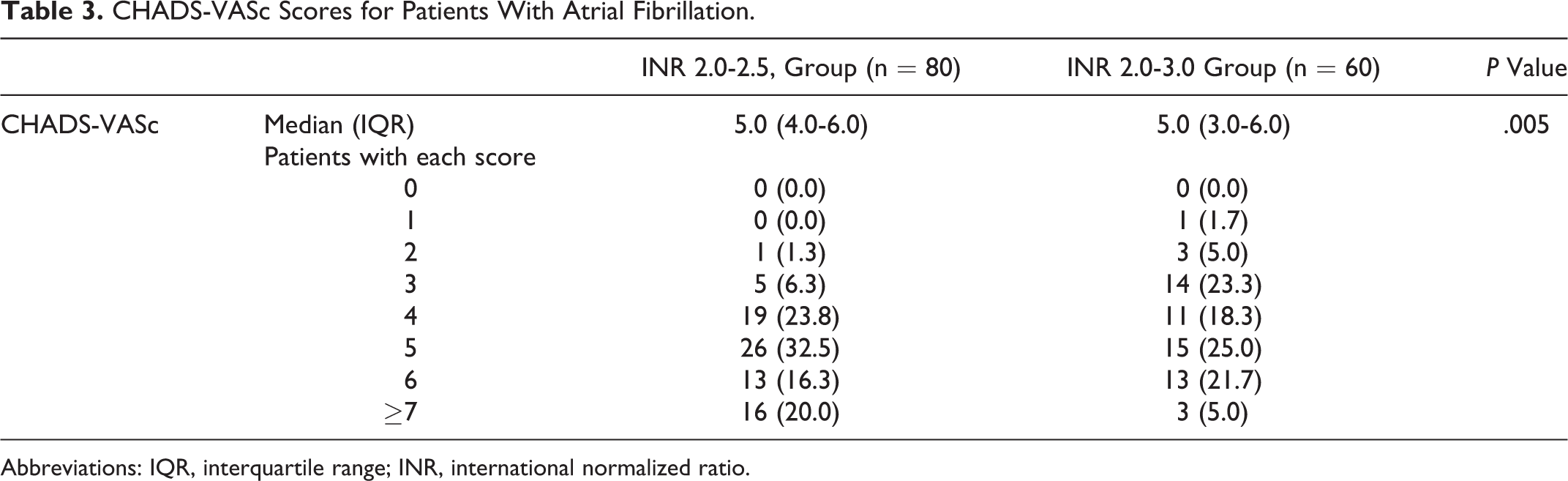
Abbreviations: IQR, interquartile range; INR, international normalized ratio.
Risk Factors for Venous Thromboembolism.
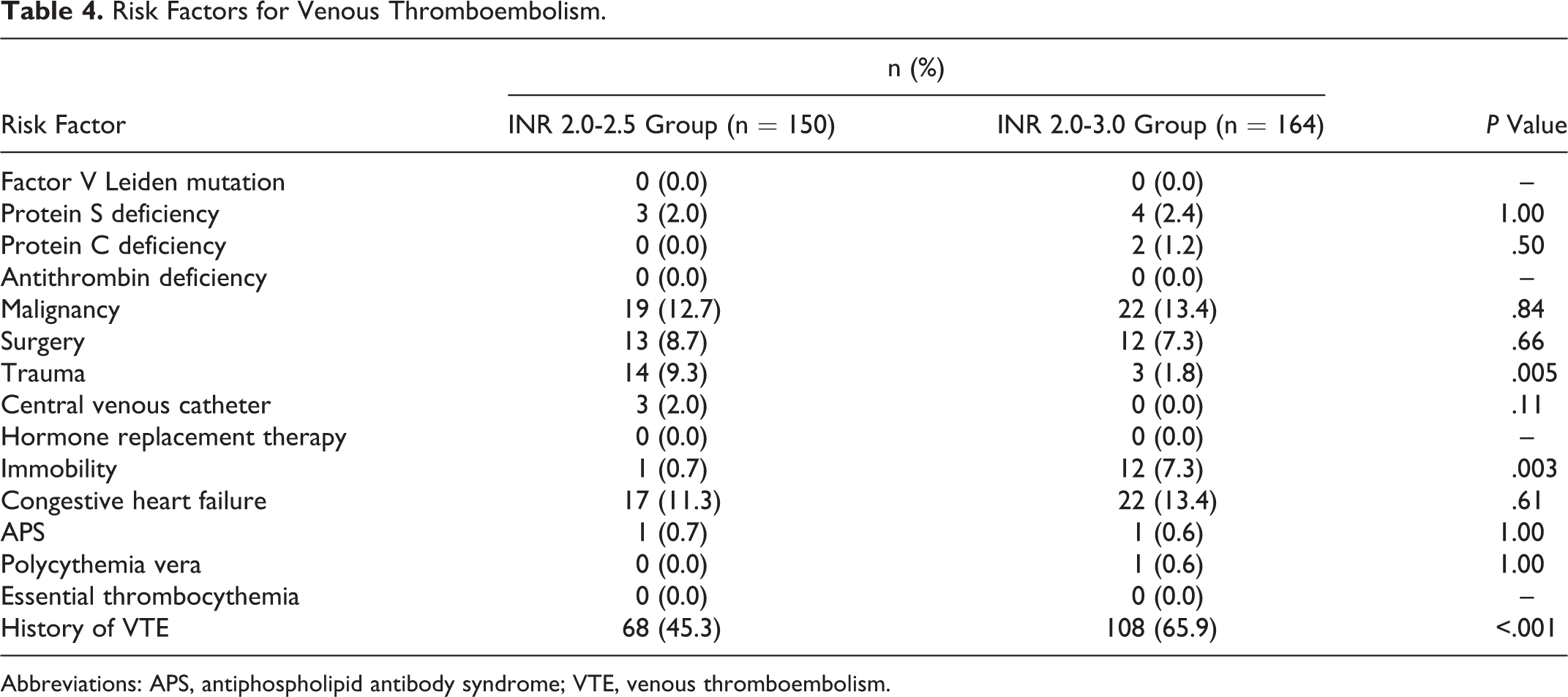
Abbreviations: APS, antiphospholipid antibody syndrome; VTE, venous thromboembolism.
Primary Outcome
The mean (SD) percentage time above INR 3.0 was significantly higher in the conventional INR group compared to the narrow INR group (6.85 [10.54] vs 4.53 [8.40], P = .03; Table 5). The difference remained statistically significant after adjusting for gender, age, ethnicity, indications for warfarin, duration of follow-up, and HAS-BLED scores (b = −0.028, 95% confidence interval [CI]: −0.054 to −0.003, P = .028).
Percentage Time Below INR 2.0, Above INR 2.5, and 3.0.

Abbreviations: INR, international normalized ratio; SD, standard deviation.
Secondary Outcomes
The mean (SD) percentage time below INR target range was comparable between both groups (narrow INR group: 36.82 [25.38] vs conventional INR group: 35.73 [28.17], P = .72; Table 5). Thirty bleeding (11 major and 19 minor bleeding events) and 14 thromboembolic events occurred in this study cohort. The number of hospitalizations per 100 patient-years for all bleeding events, major bleeding events, minor bleeding events, and thromboembolic events are presented in Table 6. Compared to the conventional INR group, patients in the narrow INR group had a lower risk for all bleeding events (adjusted IRR: 0.34; 95% CI: 0.12-0.95) and comparable risk for thromboembolic events (adjusted IRR: 0.51; 95% CI: 0.13-1.97).
Number of Hospitalization Events per 100 Patient-Years.
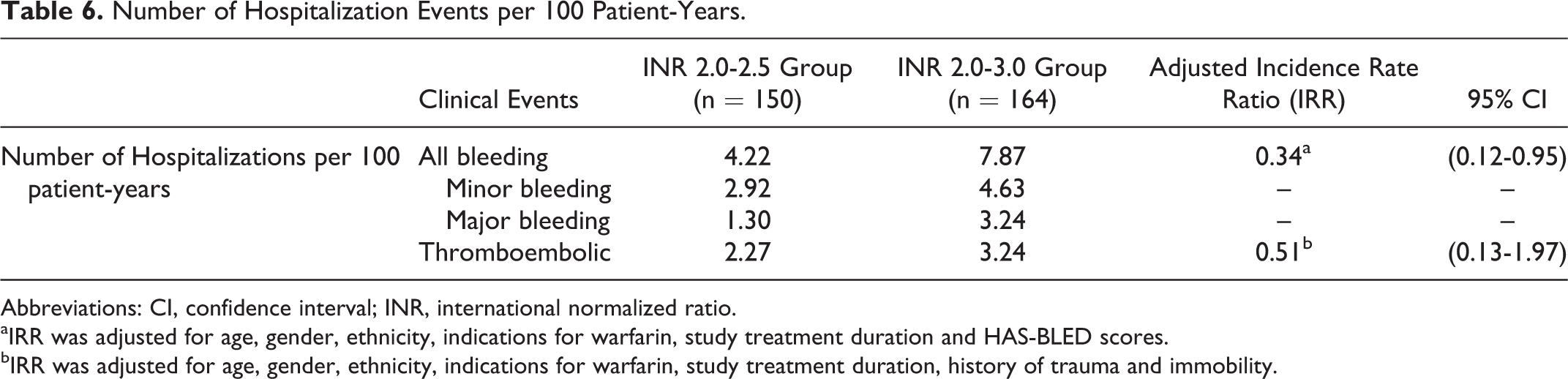
Abbreviations: CI, confidence interval; INR, international normalized ratio.
aIRR was adjusted for age, gender, ethnicity, indications for warfarin, study treatment duration and HAS-BLED scores.
bIRR was adjusted for age, gender, ethnicity, indications for warfarin, study treatment duration, history of trauma and immobility.
Discussion
Warfarin as an anticoagulant is underutilized in older adult patients, 11,22,23 and bleeding risk was often cited as the main reason clinicians were hesitant to start anticoagulation. 24,25 Among patients who were initiated on warfarin, the risk of hemorrhagic complications was substantial. 9,10 It was therefore logical to explore the feasibility of setting a narrow INR target range to improve the safety profile of anticoagulation, without compromising its efficacy.
Patients had a significantly lower mean percentage time above INR 3.0 when they were assigned the narrow INR target range. Consequently, patients in the narrow INR group spent a higher percentage of time at lower INR values when compared to their counterparts in the conventional INR group. In a similar study where older adult patients were assigned to either lower intensity (range 1.5-2.0) or standard intensity (range 2.0-3.0) group, the percentage time above INR 3.0 was reported to be 3.0% in the lower intensity group and 9.2% in the standard group. 26 This was consistent with our results. Since it has been established that INR ≥ 3.0 increased the risk of bleeding, the findings suggested that a narrow INR target range could potentially reduce the chances of bleeding.
One major concern with a narrow INR target range was the possible increased chance of underanticoagulation due to active warfarin dose reductions at a lower INR. Current literature suggests that an INR < 2.0 can be associated with stroke and other ischemic events. 18,27 However, the present findings showed no significant difference in the mean percentage time below INR 2.0 between both study groups, suggesting that a narrow INR target range does not compromise the efficacy of oral anticoagulation.
Bleeding and thromboembolic events are the major complications of oral anticoagulation. In this study, the adjusted IRR of bleeding events was lower in the narrow INR group with no difference in the IRR of thromboembolic events between both the groups. This reduced bleeding rate observed in the narrow INR group was also reported in a similar study by Naganuma et al whereby patients aged ≥ 70 years with an INR target of 1.5 to 2.5 showed a low incidence of major bleeding events. 28 However, the study by Naganuma et al had a lower target INR limit of 1.5 and was conducted only on patients with nonvalvular AF. Nonetheless, our study suggested that a narrow INR target range may reduce bleeding risk with no increase in thromboembolic complications.
Our study has several strengths. First, the baseline characteristics for the patients in this study were extensively collected. This allowed adjustments for potential confounders when analyzing the primary and secondary outcomes. Second, the retrospective nature of this analysis had the merit that it reflected real-world practice. Clinicians (pharmacists and hematologists) managing this cohort of patients did not work within the confines of prospective clinical trial protocols but treated these patients in a normal environment. We therefore expect our findings to be reproducible in actual clinical practice.
Despite the strengths, several limitations should be considered when interpreting the study findings. First, this study had the same limitations as all retrospective designs. Second, the primary outcome used in this study was a surrogate marker for clinical end points. This made head-to-head comparisons with other studies difficult because most of these studies utilized clinical end points as the primary outcome, but using clinical end points as the primary outcome would not be feasible due to large sample size requirements for rare events. Third, for the clinical end points, we captured data from the emergency department as well as hospitalized cases only. Data for patients who were treated at primary care offices were not captured. However, it was unlikely that patients who were suspected to have thromboembolism were treated at primary care offices because of the close proximity to tertiary care institutions in Singapore, which are better equipped to manage these conditions.
Conclusion
This study found that a significantly lower percentage time above INR 3.0 without increasing the percentage time below INR 2.0 can be achieved by setting a narrow INR target range at the commencement of warfarin therapy for older adult patients. Incidents of bleeding and thromboembolic complications were similar, despite patients in the narrow INR target range having higher risks of bleeding. These findings suggest that setting a narrow INR range of 2.0 to 2.5 in older adult patients could improve the safety of anticoagulation without compromising efficacy.
Footnotes
Authors’ Note
Peter Y. S. Ong and Narendran Koomanan contributed equally to this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.