
Abstract
Thrombocytopenia is common among surgical critically ill patients. The relationship between the duration of thrombocytopenia and mortality is not well studied. This retrospective 12-month cohort study was designed to evaluate the association between persistent thrombocytopenia and mortality among surgical critically ill patients to determine the risk factors for persistent thrombocytopenia. The study included adult patients consecutively admitted to the surgical intensive care unit (SICU) at our institution. Patients with a diagnosis of thrombocytopenia were identified from a prospective critical care database. We defined patients with persistent thrombocytopenia as those with thrombocytopenia lasting more than 7 consecutive days. The primary outcome of this study was 28-day mortality and the secondary outcomes were lengths of SICU stay and hospital stay. Fifty-one patients experienced persistent thrombocytopenia and 71 experienced nonpersistent thrombocytopenia. Among patients with persistent thrombocytopenia, mortality was significantly higher, and SICU and hospital stays were longer than those with nonpersistent thrombocytopenia. Risk factor analysis failed to predict which patients with thrombocytopenia would develop into persistent thrombocytopenia. Persistent thrombocytopenia is a clinically significant disorder and is associated with poorer outcomes. Future studies are needed to further define this process.
Introduction
Thrombocytopenia is a common laboratory abnormality among surgical critically ill patients. 1 –3 Studies have demonstrated that a low platelet count not only provides a diagnostic clue about the cause of the underlying disease or complicating circumstance but can also be used as a strong predictor of an adverse outcome. 4 It has been reported that thrombocytopenia in the intensive care unit (ICU) is associated with an independent risk of mortality. 5
Although thrombocytopenia has been independently linked to death in the ICU, the association between low platelet counts and poor clinical outcomes does not establish causality. 6 Thrombocytopenia in surgical intensive care unit (SICU) patients may be present at admission or can arise during hospitalization. Determining the etiology of this disorder can be difficult because SICU patients can have amass numerous potential causes of thrombocytopenia. The causes of thrombocytopenia differ in different patient populations, leading to variations in clinical characteristics, including episode duration. 7 Most research in thrombocytopenia among critical care patients has focused on the association between the occurrence of thrombocytopenia and mortality. 5,8 No studies have evaluated the impact of duration of thrombocytopenia on mortality in surgical critical care patients.
Our aims in this study were (1) to determine the incidence of hospital-acquired thrombocytopenia and persistent thrombocytopenia among surgical critical care patients, (2) to determine the association between persistent thrombocytopenia and patients’ outcomes, and (3) to elucidate the risk factors for persistent thrombocytopenia.
Method
Study Population
This retrospective database cohort study was conducted at Jinling Hospital, Nanjing, China. The study was approved by the institutional review board of Jinling Hospital, which is a tertiary academic medical center. As a national medical center for the treatment of gastrointestinal fistula, the SICU at Jinling Hospital is closed. The SICU is the primary critical care unit for patients with gastrointestinal fistula and is a secondary unit for general surgery and trauma patients. Consecutive adult SICU admissions from January 1 to December 31, 2012 were identified from a prospectively collected hospital database via individual chart review. Patient database information at our hospital is either collected automatically by computer or is entered by physicians. Specialized software (Haitai Software, Nanjing Haitai Medical Information System Company, Nanjing, China) is used to monitor integrity of the data.
Study Protocol
All patients were scanned for occurrence of thrombocytopenia after admission. In this study, thrombocytopenia was defined as a peripheral platelet count <100 × 109/L. 9 Patients who died within 24 hours of admission were excluded, as were patients who received organ transplant.
Based on the platelet counts at admission, patients were divided into a preexisting thrombocytopenia group and a nonpreexisting thrombocytopenia group. For patients with/without thrombocytopenia at admission, records of platelet counts during hospitalization were reviewed to identify episodes of thrombocytopenia. Patients who experienced thrombocytopenia during hospitalization were further categorized as persistently thrombocytopenic or nonpersistently thrombocytopenic according to the duration of thrombocytopenia. In this study, we defined patients with persistent thrombocytopenia as those who experienced thrombocytopenia for 7 consecutive days or more. For patients who experienced more than 1 episode of thrombocytopenia, the longest episode was selected for final analysis. Patients who died within 7 days of the onset of thrombocytopenia and whose last platelet count remained below normal were also classified as persistently thrombocytopenic. For patients who received platelet transfusion during an episode of thrombocytopenia, platelet counts 1 to 2 days after transfusion were evaluated. If platelet counts remained below 100 × 109/L within 2 days after transfusion, the patient was defined as persistently thrombocytopenic.
To explore the causes of persistent thrombocytopenia, database records of patients with a thrombocytopenia were reviewed. Using the disseminated intravascular coagulation (DIC) scoring system of the Japanese Association for Acute Medicine DIC scoring system (JAAM score) 10 and the DIC score of the International Society of Thrombosis and Haemostasis (ISTH score), 11 we determined if any episodes of DIC occurred during thrombocytopenia in our department.
Data Collection
Venous blood for all laboratory tests was drawn between 5 and 6
Statistical Analyses
The primary outcome of this study was 28-day mortality. Secondary outcomes were lengths of SICU and hospital stay. Risk factors associated with persistent thrombocytopenia were evaluated.
Data were analyzed with SAS software (SAS 9.1.3; SAS Institute Inc, Cary, North Carolina) and GraphPad Prism (GraphPad Software, San Diego, California). Data are presented as number (percentage) or mean ± standard deviation unless otherwise stated. Quantitative continuous variables were compared between groups with one-way analysis of variance. Categorical variables were compared with the chi-square test. The level of significance was set at .05. Cumulative survival curves were constructed with the Kaplan-Meier method, and the log-rank test was used to assess statistical differences between survival curves. To assess the risk factors for persistent thrombocytopenia and to determine if thrombocytopenia or persistent thrombocytopenia were independent predictors of mortality, multivariate analyses were performed with logistic regression.
Results
During the study period, 536 unique patients were admitted to the SICU (Figure 1). Among these, 12 were excluded because they died within 24 hours of admission. The remaining 524 patients were enrolled in our study.
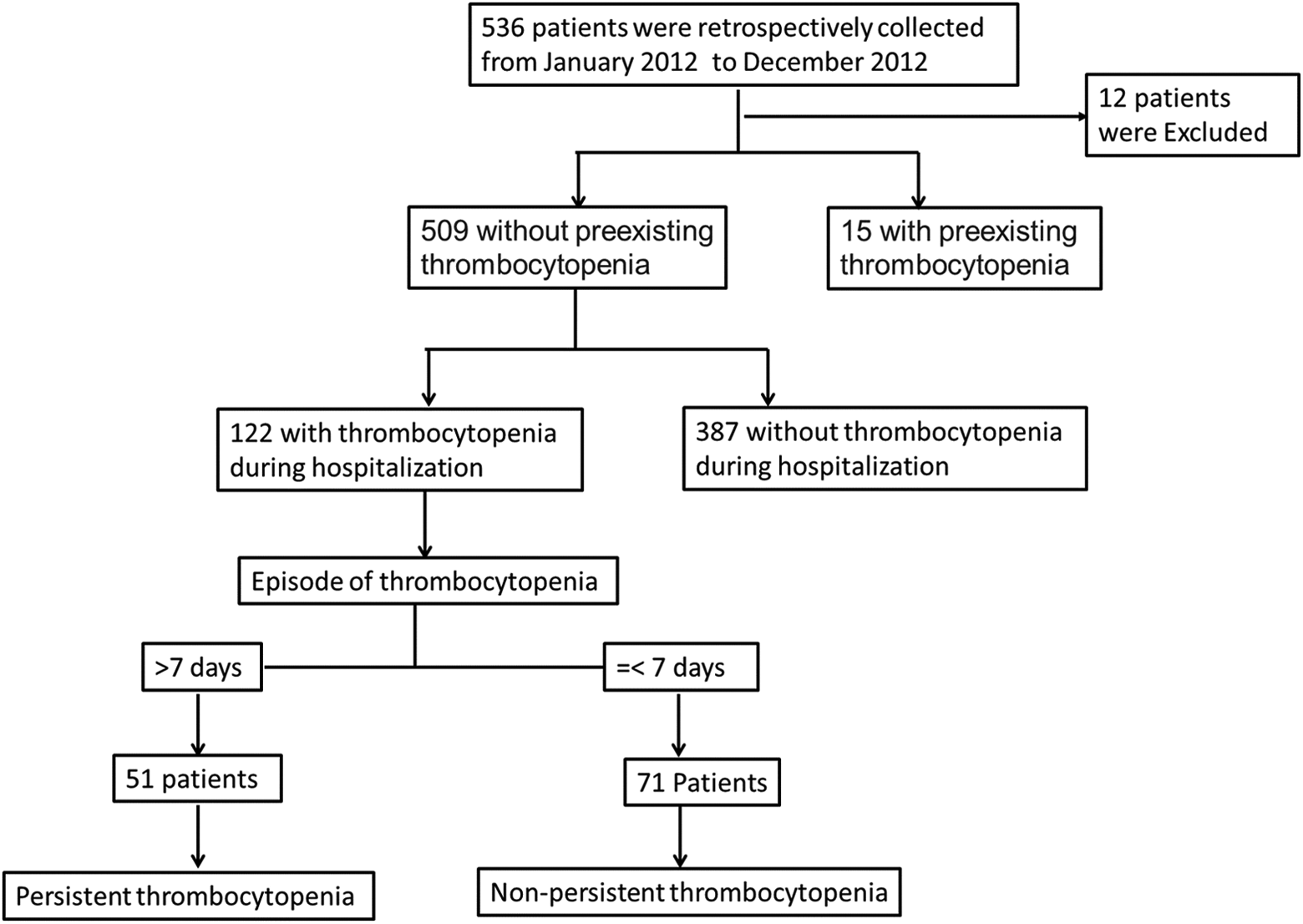
Flowchart of current study. A total of 536 patients was retrospectively collected and 524 of them met the criterion. Fifteen patients were admitted with preexisting thrombocytopenia. For 509 patients without preexisting thrombocytopenia, 122 patients experienced thrombocytopenia during hospitalization. Among them, patients were further divided into persistent thrombocytopenia group and nonpersistent thrombocytopenia group according to the episode of thrombocytopenia.
We first determined whether preexisting thrombocytopenia was present in enrolled patients. Fifteen (2.86%) patients were admitted with preexisting thrombocytopenia, while 509 (97.14%) were admitted without preexisting thrombocytopenia (Figure 1).
We divided patients without preexisting thrombocytopenia at admission into 2 groups based on the occurrence of thrombocytopenia during hospitalization (Figure 1). In our patient population, 122 (23.97%) patients without preexisting thrombocytopenia at admission experienced thrombocytopenia during hospitalization, while 387 (76.03%) did not. The incidence of hospital-acquired thrombocytopenia was 23.97% (122 of 509). The mortality rate among patients with thrombocytopenia was significantly higher than that among patients who did not experience thrombocytopenia (Table 1 and Figure 2A). Multivariate analysis indicated an independent association between the occurrence of thrombocytopenia and mortality (P = .008, Supplementary material S1).
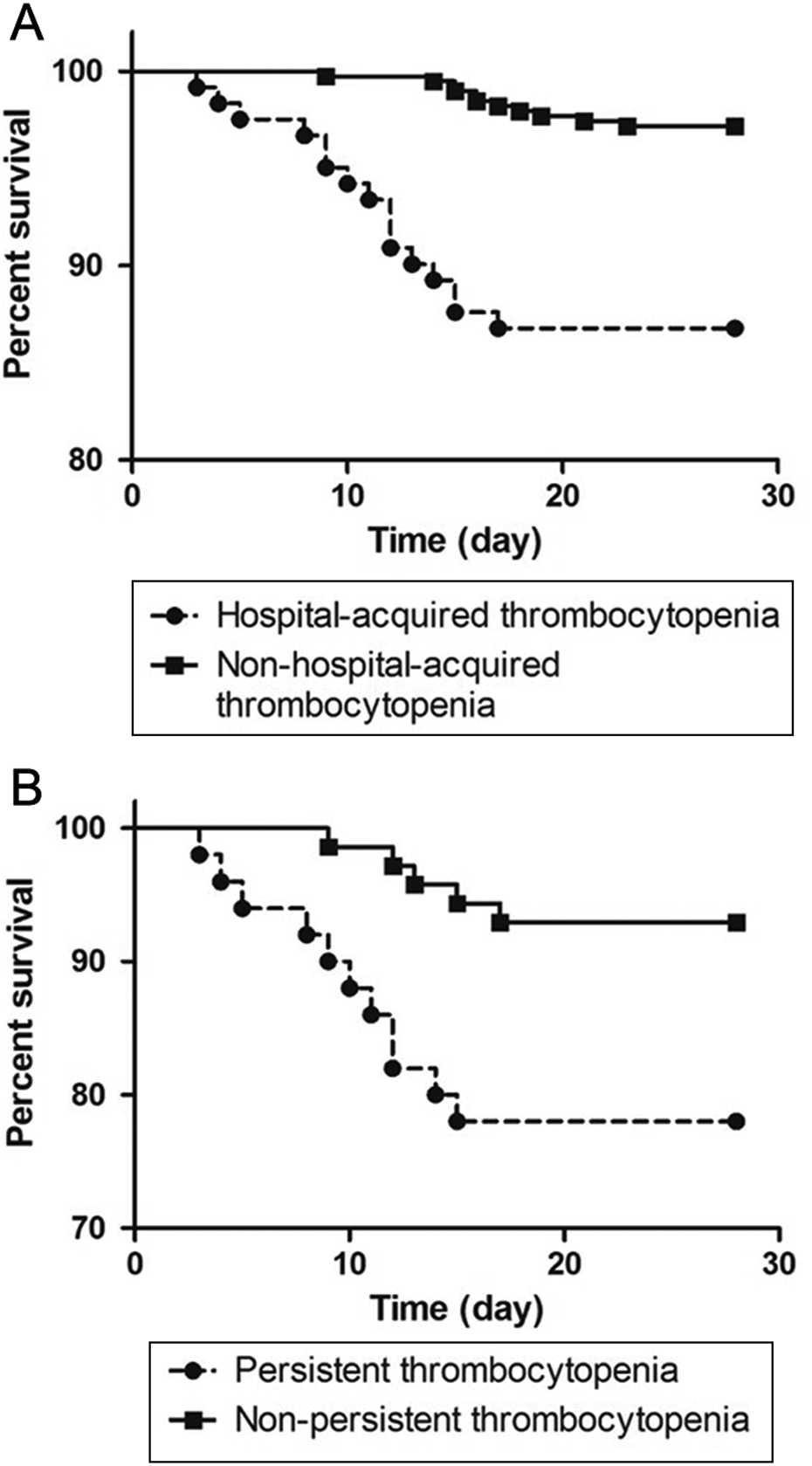
Survival analysis. A significant difference in mortality was observed between (A) patients with hospital-acquired thrombocytopenia and patients with nonhospital-acquired thrombocytopenia and (B) patients with persistent thrombocytopenia and patients with nonpersistent thrombocytopenia (P < .05).
Demographics, Clinical, and Outcome Data of Patients With/Without Thrombocytopenic Event During Hospitalization.
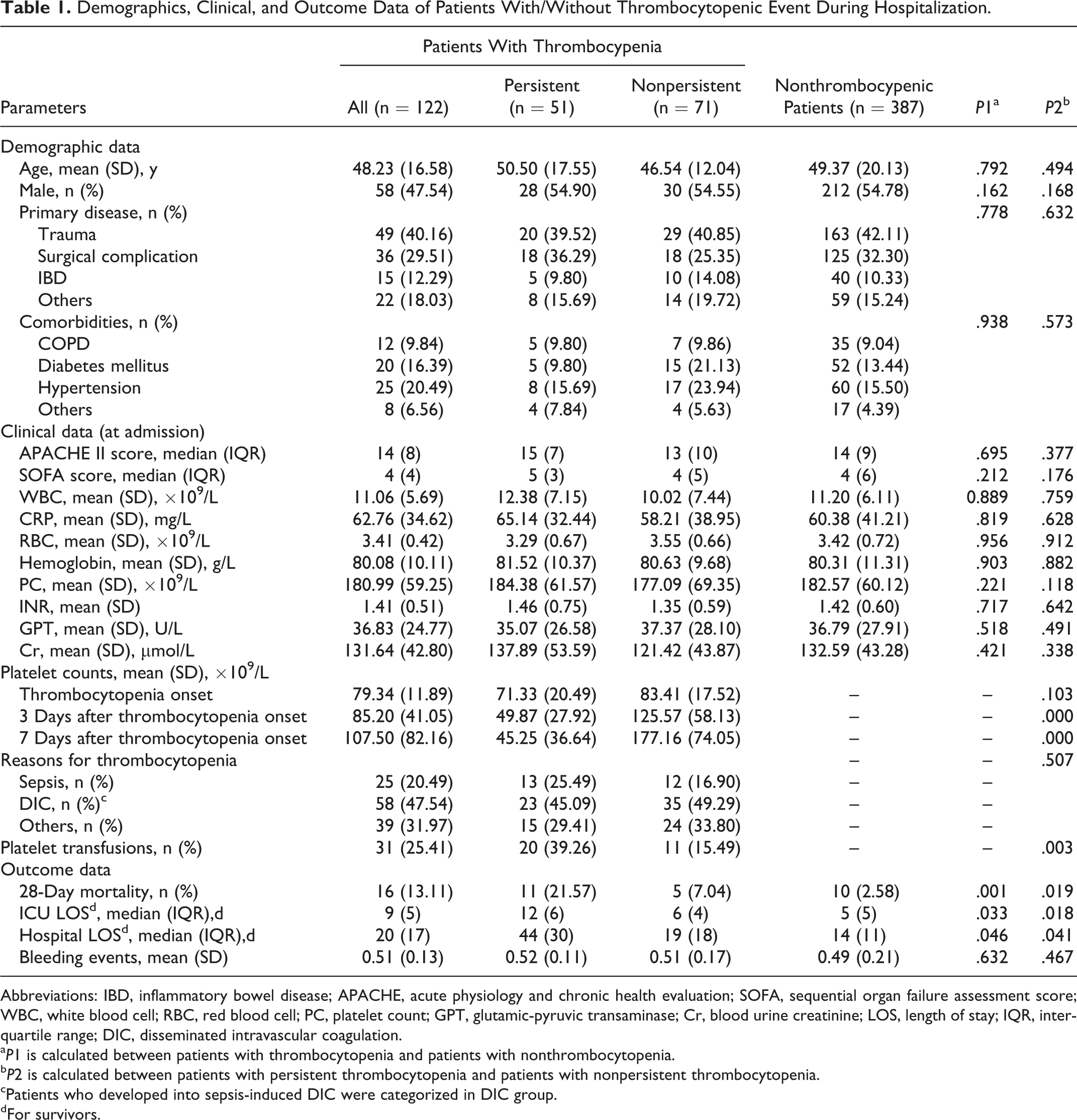
Abbreviations: IBD, inflammatory bowel disease; APACHE, acute physiology and chronic health evaluation; SOFA, sequential organ failure assessment score; WBC, white blood cell; RBC, red blood cell; PC, platelet count; GPT, glutamic-pyruvic transaminase; Cr, blood urine creatinine; LOS, length of stay; IQR, interquartile range; DIC, disseminated intravascular coagulation.
a P1 is calculated between patients with thrombocytopenia and patients with nonthrombocytopenia.
b P2 is calculated between patients with persistent thrombocytopenia and patients with nonpersistent thrombocytopenia.
cPatients who developed into sepsis-induced DIC were categorized in DIC group.
dFor survivors.
Among the patients with thrombocytopenia, 51 (41.80%) developed persistent thrombocytopenia and 71 (58.20%) experienced nonpersistent thrombocytopenia, according to our definition (Figure 1). To be specific, 8 patients in the persistent thrombocytopenia group died between 5 and 7 days after the onset of thrombocytopenia and their last platelet count remained below normal. The admission and inpatient clinical characteristics of these 2 groups were not significantly different (Table 1). Figure 3 shows changes in platelet counts after onset of thrombocytopenia in the persistent and nonpersistent thrombocytopenia groups. The 28-day mortality rates in the 2 groups were compared. Patients in the persistent thrombocytopenia group had a higher 28-day mortality compared with those in the nonpersistent thrombocytopenia group (Table 1 and Figure 2B). Moreover, nonpersistent thrombocytopenic patients had a shorter ICU stay and shorter hospital stay compared with patients who experienced persistent thrombocytopenia (Table 1). Multivariate analysis indicated that persistent thrombocytopenia was independently associated with mortality (P = .031, Table 2). Table 3 shows the fluctuation in platelet counts after the onset of thrombocytopenia. Mortality during an episode of thrombocytopenia was also significantly different between persistent and nonpersistent thrombocytopenia groups. There was no significant difference between the 2 groups in maximum fluctuation of platelet counts or decrease in platelet count within 24 hours of thrombocytopenia. The clinical data of patients with versus without persistent thrombocytopenia after thrombocytopenia onset are also evaluated (Supplementary material S2). There were no differences in clinical parameters at the onset of thrombocytopenia between the groups. However, WBC counts were significantly different 3 and 7 days after the onset of thrombocytopenia. Moreover, prothrombin time and activated partial thromboplastin time were significantly different between the 2 groups 7 days after the onset of thrombocytopenia.
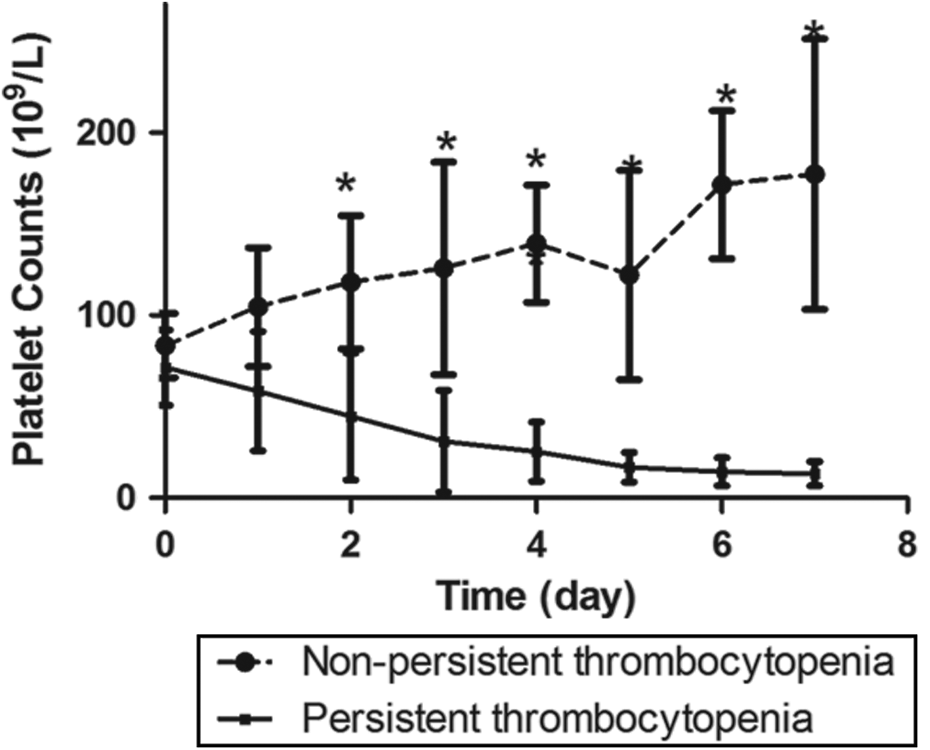
Changing trend of platelet counts after onset of thrombocytopenia over time. A significant changing trend of platelet counts was observed in this study. A statistically significantly difference was exhibited between the persistent thrombocytopenia group and nonthrombocytopenia group from the 2nd day after initiation of thrombocytopenia. *P < .05.
Multivariate Analysis of Persistent Thrombocytopenia and Other Covariates Associated With Mortality.a
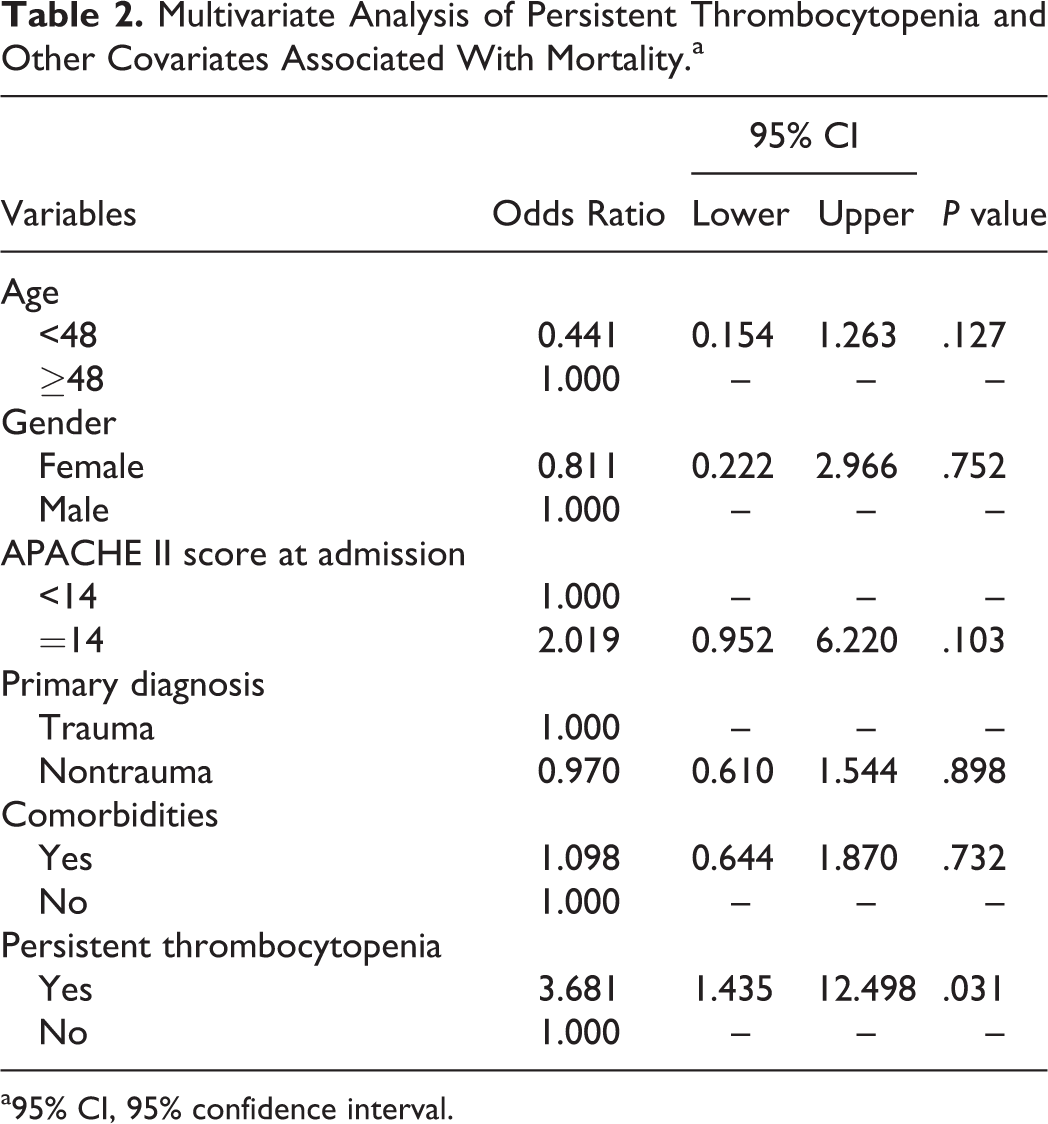
a95% CI, 95% confidence interval.
Comparison of Persistent Thrombocytopenia and Nonpersistent Thrombocytopenia Episodes.
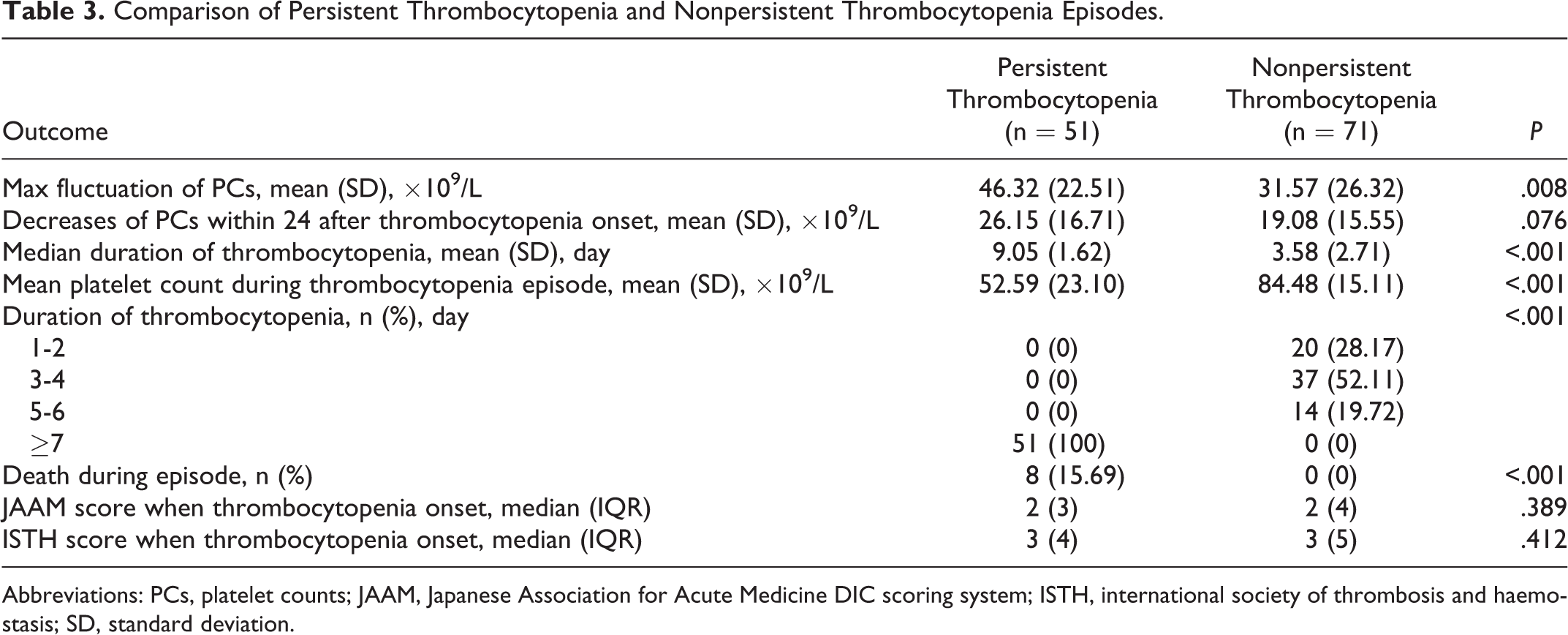
Abbreviations: PCs, platelet counts; JAAM, Japanese Association for Acute Medicine DIC scoring system; ISTH, international society of thrombosis and haemostasis; SD, standard deviation.
The reasons for thrombocytopenia during hospitalization were explored and are shown in Table 1. There was no significant difference between persistent and nonpersistent groups in the caused evaluated. We used logistic regression analysis to determine the risk factors for persistent thrombocytopenia (Table 4). In particular, demographics, comorbidities, baseline platelet count, and illness severity at the onset of thrombocytopenia did not predict persistent thrombocytopenia in the SICU.
Logistic Regression Analysis of Risk Factors for Developing Persistent Thrombocytopenia.a
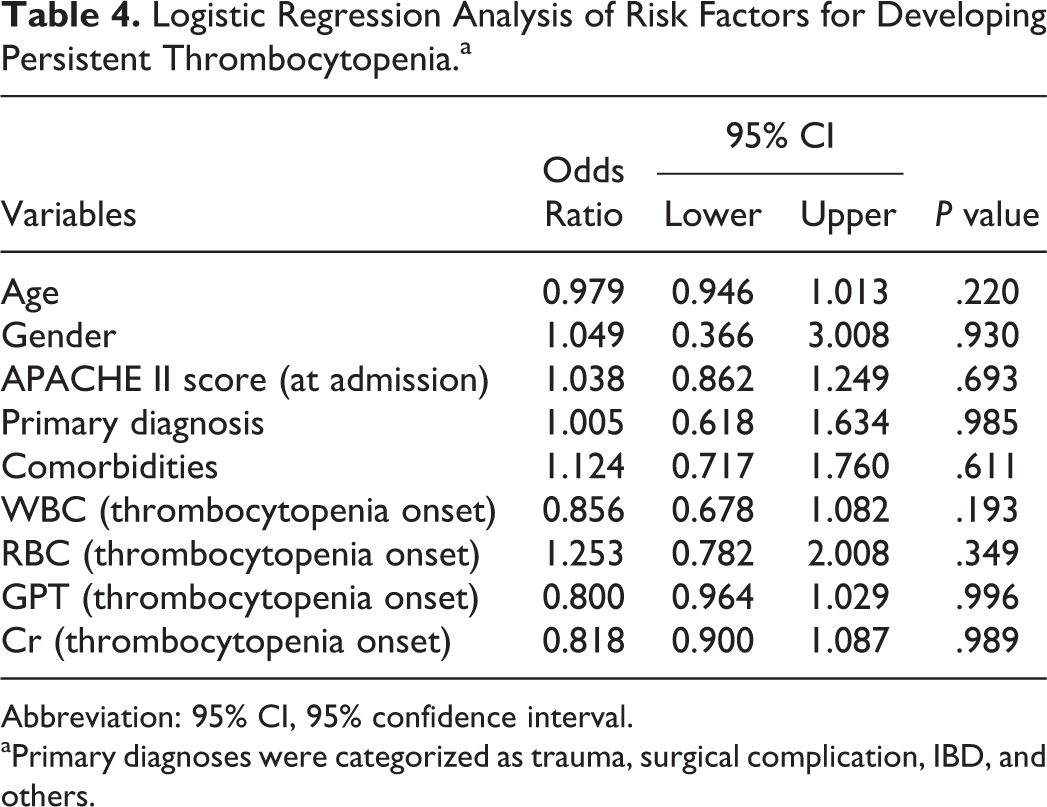
Abbreviation: 95% CI, 95% confidence interval.
aPrimary diagnoses were categorized as trauma, surgical complication, IBD, and others.
Discussion
This was a retrospective investigation of persistent thrombocytopenia in a cohort of surgical critically ill patients. The principal findings were that persistent thrombocytopenia was common among patients admitted to the SICU and was associated with worse outcomes and greater utilization of hospital resources than for patients without persistent thrombocytopenia. Unfortunately, risk factor analysis failed to determine predictors of persistent thrombocytopenia. Although it has been reported that thrombocytopenia at any time during an ICU stay is associated with poorer outcome, 3,12,13 our findings indicate that the adverse risk is present primarily for those patients with persistent rather than transient thrombocytopenia.
Thrombocytopenia is a clinically significant phenomenon that is common among critically ill patients, occurring in at least one-third of surgical critical care patients. 2 Several studies have demonstrated an association between thrombocytopenia and patient outcomes. 4,7 Thrombocytopenia on admission appears to be a risk factor for mortality in critically ill patients and is related to higher illness severity, organ dysfunction, sepsis, and renal failure. 2,8,14 Recent studies have evaluated decreased platelet counts among patients with ICU-acquired pneumonia and have found the association between septicemia-related thrombocytopenia and mortality. 15,16
Although thrombocytopenia has an independent association with death in the ICU, the association does not establish causality, nor does it provide adequate evidence to support platelet transfusion. 6 In this study, we investigated persistent thrombocytopenia among surgical critical care patients. Because there is no consensus on the definition or classification of persistent thrombocytopenia, we defined it as platelet counts below the normal range for 7 consecutive days. This time interval was chosen based on the half-life of platelet under physiological conditions. The impact of platelet transfusions was also evaluated in our study. The decision to administer a platelet transfusion was made by the physicians and may have been based on various criteria. We choose to evaluate the platelet counts within 2 days after transfusion to determine whether platelet counts returned to normal. Patients are rarely transfused to achieve a platelet count above 100 × 109/L. Platelet transfusions had little impact on our patient classification. In 2013, we had conducted a prospective study to evaluate the efficiency of recombinant human thrombopoietin, which has a direct effect on platelet count. Thus, we chose the patients admitted in 2012 for analysis in the present study. 17 For patients who died within 7 days of the onset of thrombocytopenia and whose last platelet count remained below normal in our study, we considered them as patients with persistent thrombocytopenia because those patients died between 5 and 7 days after the onset of thrombocytopenia and their platelet counts have limited possibility to return to a normal level within at most 2 days.
Thrombocytopenia in surgical critical care patients can result from various causes, including sepsis and DIC. 3,18 In our study, half of patients with thrombocytopenia had concurrent DIC. However, there were no significant differences in JAAM score or ISTH score in patients with thrombocytopenia versus those without, indicating that DIC was not the main cause of thrombocytopenia. Because this was a retrospective study, the cause of thrombocytopenia was not always clear. Also, we did not measure heparin-induced antibody levels, the key diagnostic test for heparin-induced thrombocytopenia. Thus the role of heparin- and drug-induced thrombocytopenia may have been underestimated in our study for persistent thrombocytopenia.
We analyzed the risk factors for persistent thrombocytopenia and found that patients’ condition at the onset of thrombocytopenia was not associated with persistent thrombocytopenia. Risk factor analysis did not predict persistent thrombocytopenia during hospitalization. This finding indicates that various factors were involved in the process of persistent thrombocytopenia. According to our data, patients with sepsis were more likely to have persistent thrombocytopenia than nonpersistent thrombocytopenia. We speculate that the persistent thrombocytopenia in surgical critical care patients was mainly associated with persistent infections.
Our results confirmed the finding of the study by Akca et al 19 that changes in platelet count among the critically ill patients have a biphasic pattern that differs in survivors versus nonsurvivors. The average platelet counts of nonsurvivors in Akca’ s study were higher than those in our study. One possible reasons for this difference is the differences between the study populations.
In the present study, we performed a multivariate analysis to determine the potential risk factor for persistent thrombocytopenia. Although risk factor analysis failed to predict differences between patients with versus without persistent thrombocytopenia, our findings might help explain why a low platelet count is such an important measure of illness in ICU patients. Although patients with persistent thrombocytopenia constitute a minority group, they often consume an important portion of health care resources, because they have severe illnesses requiring prolonger hospitalization. Our study raises the possibility that the major negative impact of thrombocytopenia results from its duration.
This study has several important limitations. Because surgical patients have unique clinical conditions and risk factors for thrombocytopenia and may have increased risk of persistent thrombocytopenia resulting from perioperative care, these findings may not be representative of persistent thrombocytopenia in other patient populations. Because of the study design, making a diagnosis of cause of thrombocytopenia is extremely challenging and the causes of thrombocytopenia were not fully determined. In classifying thrombocytopenia as a singular process, we may have missed differences among common etiologies such as malperfusion, administration of agents that are associated with the risk of persistent thrombocytopenia or agents that may cause the phenomenon. Future work will assess these variables. Although our findings indicate that persistent thrombocytopenia is clinically important, information on long-term outcomes among patients who survived from persistent thrombocytopenia is lacking. Finally, as with all retrospective database studies, there are concerns about observation bias. Despite these weaknesses, this study does provide an important and novel evaluation of persistent thrombocytopenia in critically ill surgical patients.
Footnotes
Acknowledgments
We want to express our sincere thanks to Rebecca Tollefson for the help in revising the manuscript.
Authors Contribution
QW, JR, and JL designed the whole study. JR, YZ, and JL supervised the whole project. QW, GL, and DH performed data analysis. GW, XW, GG, JC, ZH, and HR supervised patient diagnosis and recruitment. QW, GL, and NA conducted data analyses and drafted the manuscript. DH and XW participated in the manuscript writing. All authors critically reviewed the article and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work was supported by grants from the National Natural Science Foundation of China (81270478).