
Abstract
Heparin-induced thrombocytopenia (HIT) antibodies are screened by an enzyme-linked immunosorbent assay (ELISA). Polyspecific ELISA detects anti-PF4/heparin IgG, IgA, and IgM. Recently, anti-PF4/heparin IgG ELISA has been shown to be more specific. However, the impact of using the IgG-ELISA on the incidence of isolated HIT (thrombocytopenia alone without clinically evident thrombosis) and the risk of developing subsequent thrombosis are still unknown.
Introduction
Heparin-induced thrombocytopenia (HIT) is a transient autoimmune disorder where heparin exposure results in the formation of antibodies against platelet factor 4 (PF4) and heparin complex that activates platelets and causes thrombocytopenia with or without thrombosis.1,2 Heparin-induced thrombocytopenia occurs between 5 and 14 days following unfractionated heparin (UFH) exposure in about 1% to 5% of patients, and thrombosis occurs in 30% to 50% of these patients.3,4 Up to two thirds of patients diagnosed with HIT have thrombocytopenia alone as initial manifestation of HIT without clinically evident thrombosis (the so-called isolated HIT). These patients are thought to have up to 30% to 50% risk of thrombosis within the subsequent 28 days.5,6
Heparin-induced thrombocytopenia antibodies are commonly screened by an enzyme-linked immunosorbent assay (ELISA) test by the GTI Diagnostics (Brookfield, Wisconsin), because it is simple, sensitive, and has a rapid turnaround time compared with functional tests such as the serotonin release assay (SRA). It is considered positive if the optical density (OD) of a patient’s serum is >0.4. In the absence of HIT clinical syndrome, there is a high incidence of false positivity with ELISA, especially in cardiac surgery patients who are often exposed to very high amounts of heparin. 7
Polyspecific ELISA detects anti-PF4/heparin immunoglobulin G (IgG), IgA, and IgM. These polyspecific ELISAs are highly sensitive, but have lower specificity and higher false-positive rate. 8 The literature suggests that the IgG interacting with FcγRIIA receptors on platelets has potential to cause HIT.9–11 Recently, anti-PF4/heparin IgG ELISA has been shown to be sensitive but more specific than the polyspecific IgG, IgM, and IgA ELISAs. 12 However, the incidence of isolated HIT and the risk of developing subsequent thrombosis with the IgG ELISA are still unknown. Therefore, we performed a retrospective review of our data to address these 2 questions.
Methods
This retrospective observational study was performed at The University of Texas Southwestern Medical Center and affiliated hospitals. We included all consecutive patients being tested for the anti-PF4/heparin IgG from December 2008 to May 2010, using the IgG-specific anti-PF4/heparin ELISA with a 2-step assay using high-dose heparin in the second step to demonstrate heparin specificity. A positive test was defined as OD >0.4 with greater than 50% inhibition.
Results
A total of 492 patients were tested during the study period. A diagnosis of HIT was made in 29 patients (6%) based upon clinical findings (4T score ≥4) and positive ELISA. In 19 (65%) of 29 patients, a thrombosis was seen at the time of diagnosis; whereas 10 (35%) of 29 had only isolated HIT.
All the 10 patients with isolated HIT had serial follow-up for at least 3 months following the time of diagnosis (Table 1). Only 3 of these 10 patients were treated with direct thrombin inhibitors (DTIs) and only 5 of them were treated with warfarin for at least 1 month upon discharge. While only 5 of these 10 patients had compression ultrasonography to rule out occult lower extremity thrombus, none of them (including 6 with an OD >1.0) developed symptoms or signs of thrombosis in the subsequent 3 months after the diagnosis of isolated HIT.
All the 10 patients with isolated HIT had serial follow-up for at least 3 months following the time of diagnosis (Table 1). Only 3 of these 10 patients were treated with direct thrombin inhibitors (DTIs) and only 5 of them were treated with warfarin for at least 1 month upon discharge. While only 5 of these 10 patients had compression ultrasonography to rule out occult lower extremity thrombus, none of them (including 6 with an OD >1.0) developed symptoms or signs of thrombosis in the subsequent 3 months after the diagnosis of isolated HIT.
Further Information About Patients With Isolated Heparin-Induced Thrombocytopenia
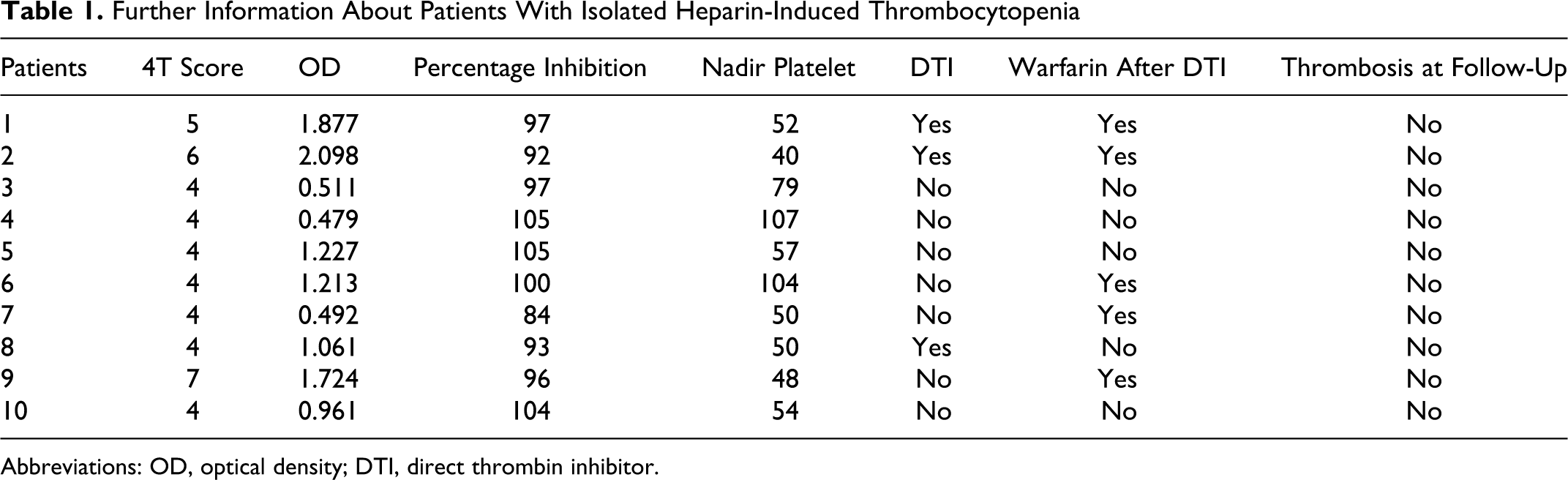
Abbreviations: OD, optical density; DTI, direct thrombin inhibitor.
Discussion
The incidence of isolated HIT in this study was 35% (of all patients diagnosed with HIT), which is significantly lower than previously reported by others, including our own historical data (57.4%) 5 using the IgG, IgM, and IgA polyspecific anti-PF4/heparin ELISAs. It is possible that some patients previously thought to have HIT by the polyspecific anti-PF4/heparin ELISA had false-positive results. The IgG-specific anti-PF4/heparin ELISA appears to improve the specificity of the ELISA, and it also significantly reduces the number of patients with isolated HIT who appear to have lower risk of subsequent thrombosis.
A recent literature review by Cuker and Ortel, 12 found 5 studies13–17 that compared the 2 assays. In pooled analysis of these studies, the IgG-specific ELISA had higher specificity (93.5% vs 89.4%) but lower sensitivity (95.8% vs 98.1%) than the polyspecific ELISA. They recommended the use of the more sensitive polyspecific ELISA as a screening test for HIT despite the IgG-specific ELISA yields fewer false-positive results than the polyspecific ELISA. However, as the authors state, these results suffer from limited validity by differences in the study populations, “gold standard” definitions of HIT, and the immunoassays utilized.
Despite the small number of patients reviewed, its retrospective nature, and the absence of confirmation by more specific functional assays, this study identifies a lower incidence of isolated HIT and a significantly lower risk of subsequent thrombosis in our patient population when the IgG-specific anti-PF4/heparin ELISA was used. Obviously, a larger prospective study is required to confirm these findings. Another important correlative issue needed in this area is an economic analysis to define the costs of false-positive and false-negative tests. This would help determine a better “trade-off,” a more sensitive, or a more specific ELISA for patients with suspected HIT.
Footnotes
This work was presented in part at the 52nd Annual Meeting of the American Society of Hematology, Orlando, FL, December 4-7, 2010.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.