
Abstract
Objective:
For the present study, the authors hypothesized that the
Methods:
Doppler ultrasonography of lower limbs was performed pre- and postoperatively to evaluate for deep vein thrombosis in 150 patients who underwent open reduction and internal fixation (ORIF). Plasma
Results:
Plasma
Conclusion:
Using a threshold of 3 mg/L, the
Introduction
Venous thromboembolism (VTE) is the major cause of morbidity and mortality in posttraumatic patients who have undergone orthopedic surgeries. 1 Although, the condition is often asymptomatic, life-threatening pulmonary embolism (PE) is the first clinical manifestation of posttraumatic deep vein thrombosis (DVT) of the lower limb in many patients. 2 Of all trauma admissions with complicated injury, PE has been reported up to 0.55%. 3 Thus, the prevention of postoperative DVT and PE must be balanced with the increased bleeding risks of anticoagulation. 4,5
Although low plasma
For the present study, we hypothesized that the activation of blood coagulation after surgery among patients younger than 50 years with lower limb fractures would elevate plasma
Methods
Patients
This study was conducted at Shanghai Tenth People’s Hospital, Tongji University, Shanghai, China. After obtaining institutional review board approval (SHSY-IEC-pap3.0/14-11), a prospective study was carried out from October 2012 until March 2014.
Several previous studies have demonstrated that
Cases were selected from patients younger than 50 years with lower limb fractures admitted to the Department of orthopedics, Shanghai Tenth People’s Hospital, Tongji University, Shanghai, China. The exclusion criteria were gravidity, age less than 18 years, perioperative administration of blood products, abnormal blood coagulation, administration of anticoagulation therapies, liver disease, and preoperative diagnosis of DVT. A total of 155 consecutive patients met the primary inclusion criteria and signed the informed consent.
Five patients were excluded from the study because of age less than 18 years (n = 2) or administration of aspirin for anticoagulation therapies (n = 3). Of the remaining 150 patients, 58 were females and 92 were males. Their mean age (±standard deviation) was 43 ± 19.1 years (range 18-49 years). All patients were diagnosed by X-ray or computed tomography (CT) of lower limb fractures, including 29 (19.3%) femoral fractures, 33 (22%) patella fractures, 35 (23.3%) tibial plateau fractures, 37 (24.7%) tibia-fibula fractures, and 16 (10.7%) ankle–foot fractures (Table 1). Table 1 summarizes the clinical variables.
Clinical Parameters of the VTE+ and VTE– Subgroups.a
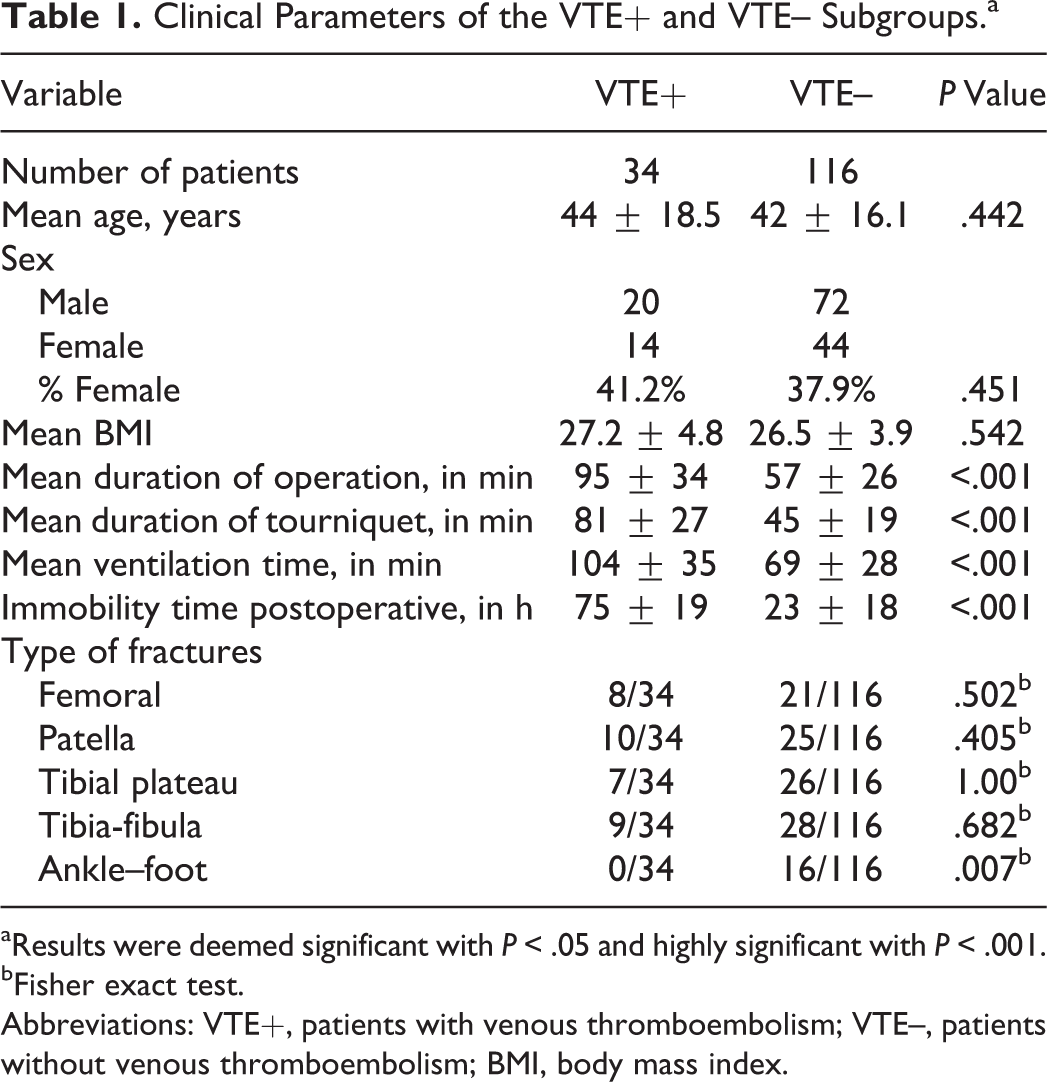
aResults were deemed significant with P < .05 and highly significant with P < .001.
bFisher exact test.
Abbreviations: VTE+, patients with venous thromboembolism; VTE–, patients without venous thromboembolism; BMI, body mass index.
All patients were treated with open reduction and internal fixation (ORIF) under general anesthesia with ventilation. The duration of surgery, from incision to wound closure, was recorded. All patients received similar prophylactic anticoagulant, with administration of low-molecular-weight (LMW)-heparin 4000 U once a day, from the first postoperative day until discharge. No other prophylactic treatments were performed. When VTE was diagnosed, therapeutic anticoagulation therapy was carried out, with administration of LMW-heparin 4000 U twice a day. All patients were followed up for 3 months or more.
d -Dimer Plasma Levels
Doppler Ultrasonography and Diagnosis of DVT or PE
All examinations were conducted with the same device (Sonoline Antares, Siemens Sector Healthcare, Forchheim, Germany) by the qualified examiners. Examinations were performed 2 days before surgery and between the third and seventh days after surgery. Diagnosis of DVT was based on direct thrombus detection by incomplete compressibility of the vessel, observation of lack of blood flow, or both. All patients were examined on both sides of lower limbs. Pulmonary embolism was diagnosed by CT examinations, which were performed if patients were diagnosed with DVT by Doppler ultrasonography or showed symptoms of PE, including thoracic pain, unexplained loss of consciousness, acutely reduced blood pressure, or acutely reduced oxygen saturation. All radiologists were blind to patients’
Statistical Analysis
All data were entered in Excel database and analyzed with IBM SPSS Statistics 19.0. The mean values of
Results
Postoperative VTE was diagnosed in 34 (22.7%) of all patients. Deep venous thrombosis was seen in 28 (18.7%) patients. Of the 28 diagnosed cases with DVT, 7 were symptomatic with calf swelling. Of 28 diagnosed cases with DVT, 4, 2, 2, 16, 2, and 2 clots were located in deep femoral vein, superficial femoral vein, distal femoral vein, popliteal vein, peroneal vein, and posterior tibial vein, respectively. Of the 7 symptomatic cases with DVT, 2, 4, and 1 clots were located in distal femoral vein, popliteal vein, and posterior tibial vein, respectively. Pulmonary embolism was detected in 9 (6%) of the patients. Of the 9 diagnosed cases with PE, 6 were diagnosed without DVT because of thoracic pain, and 3 PE was diagnosed by CT examinations, which were performed after patients were diagnosed with DVT. During all the follow-up period, there was no incidence of new VTE diagnoses or major bleeding events.
Risk Factors for VTE
Various clinical variables were assessed and analyzed for their potential impact regarding incidence of VTE (Table 1). A highly significant difference (P < .001) was demonstrated for duration of surgery, tourniquet time, ventilation time, and time of postoperative immobility of lower limbs. In patients with VTE, the mean duration of surgery was 95 minutes, whereas it was 57 minutes in patients without VTE. The mean ventilation time was 104 minutes in patients with VTE and 69 minutes in patients without VTE. The mean tourniquet time was 81 minutes in patients without VTE and 45 minutes in patients with VTE. The mean time of postoperative immobility was 75 hours in patients with VTE and 23 hours in patients without VTE.
There was no significant difference in the other clinical variables, including age, sex, body mass index (BMI), and type of fractures, between the patients with and without VTE (P > .05).
Plasma d -Dimer Level: Comparison of Mean Values
Student t test was used to compare the mean values of plasma
Comparison of
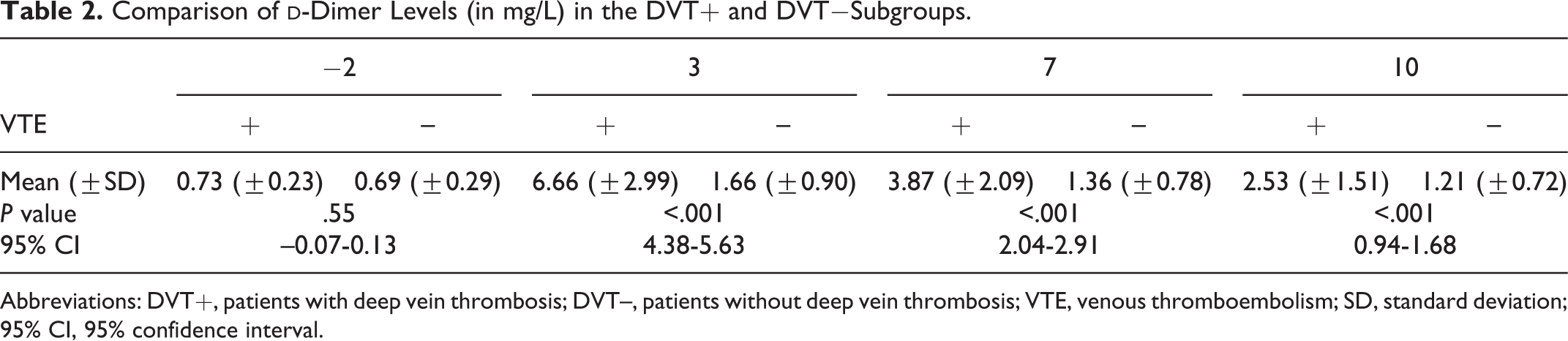
Abbreviations: DVT+, patients with deep vein thrombosis; DVT–, patients without deep vein thrombosis; VTE, venous thromboembolism; SD, standard deviation; 95% CI, 95% confidence interval.
Determination of Discrimination Points: Plasma d -Dimer Level Thresholds
Considering the
An ROC analysis was used to evaluate plasma
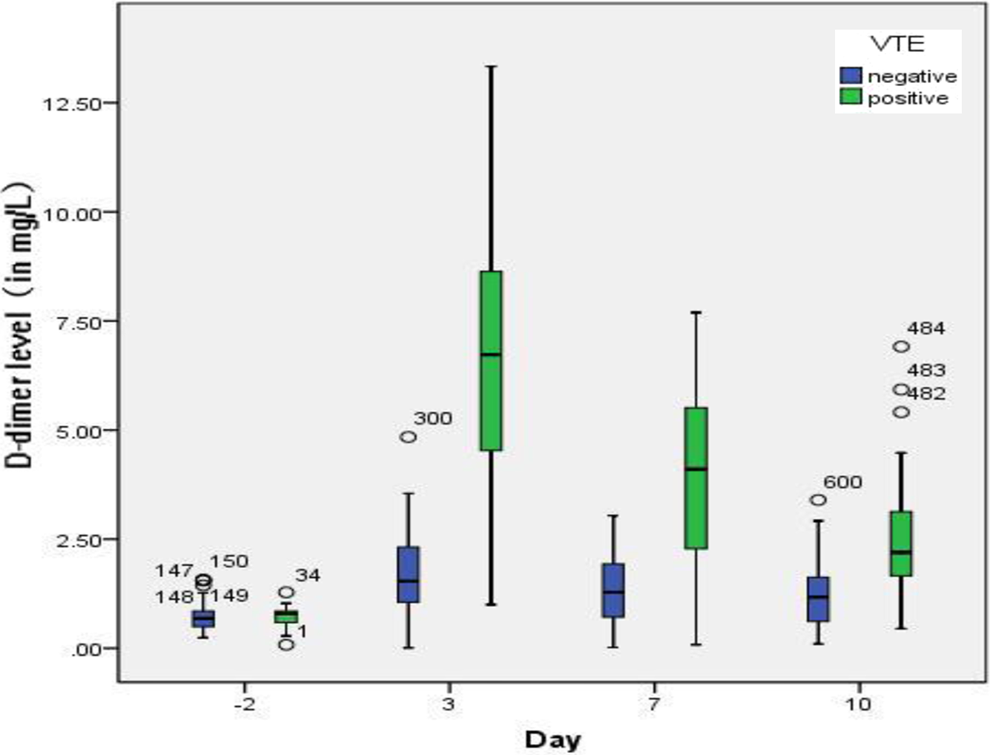
Boxplot of
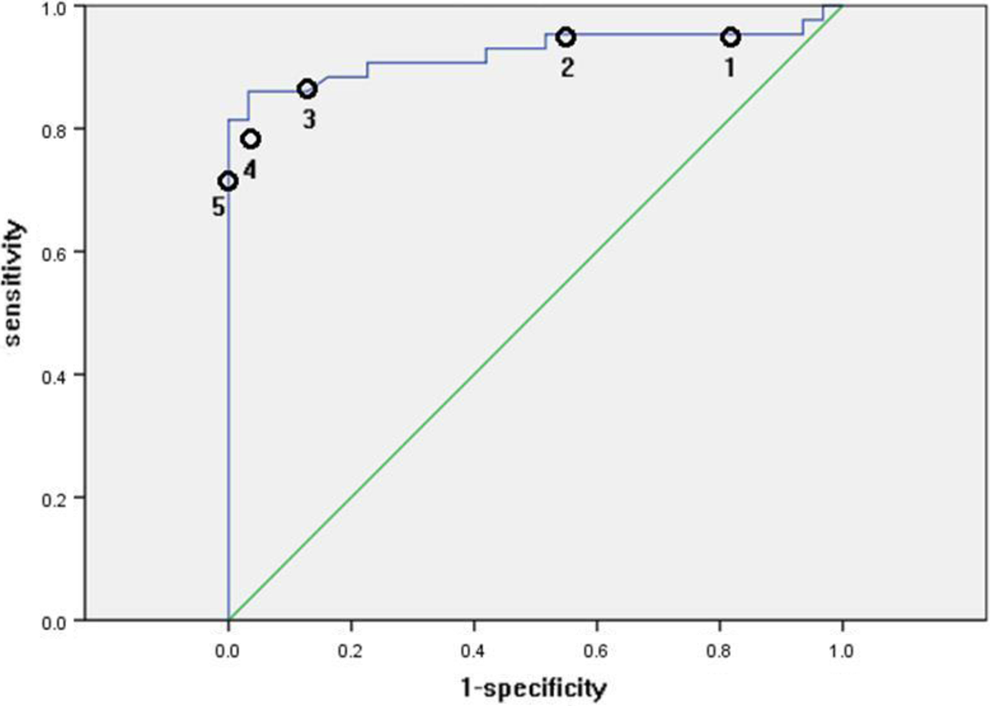
The receiver operating characteristic (ROC) curve for
Sensitivities and Specificities of Different Thresholds on Third Day Postoperation.
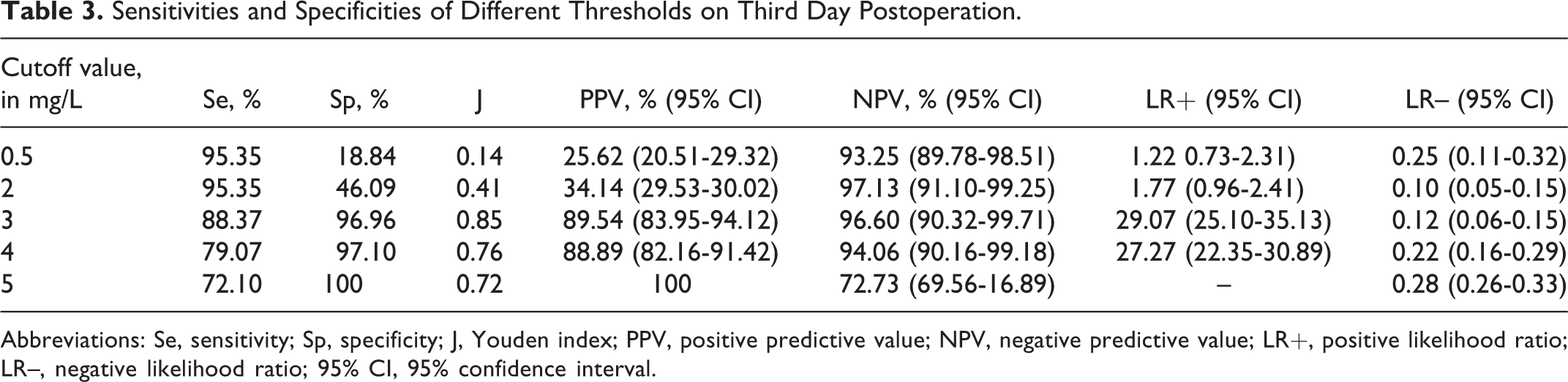
Abbreviations: Se, sensitivity; Sp, specificity; J, Youden index; PPV, positive predictive value; NPV, negative predictive value; LR+, positive likelihood ratio; LR–, negative likelihood ratio; 95% CI, 95% confidence interval.
The Youden index (J), PPV, NPV, and LR+, of 0.85, 89.54% (95% CI 83.95-94.12), 96.60% (95% CI 90.32-99.71), 29.07 (95% CI 25.10-35.13), respectively, reach their maximum distance to the diagonal reference line and optimizes the discriminatory power of a test, assuming that sensitivity and specificity are of the same value. Thus, a cutoff value of 3 mg/L was calculated (J = 0.85). The sensitivity was 88.37%, and the specificity was 96.96% (Table 3).
Discussion
Several studies have established that patients with trauma carry a significantly increased risk for the development of venous thromboembolic disease. 17,18 And VTE is the major cause of morbidity and mortality in posttraumatic patients who have undergone orthopedic surgeries. 1 Therefore, the postoperative diagnosis and management of VTE attract wide attention clinically.
The data from present study supports the hypothesis that undergoing ORIF for patients younger than 50 with lower limb fractures raises plasma
For this study, the development of VTE was not influenced by patient’s age, sex, type of fractures, or BMI. This finding is inconsistent with other studies, 22 which have demonstrated a higher risk of VTE in patients with older age. We consider that the contradiction in our study may be due to the sample size of 150 patients. However, longer duration of surgery, longer duration of tourniquet, longer ventilation time, and longer time of immobility are proved to be risk factors for the development of VTE in consistence with other studies.
In 1997, Wells et al carried out a prospective cohort trial of outpatients with symptoms and suspected DVT. 23 The DVT was diagnosed by ultrasound or venography. The results showed 3%, 17%, and 75% of the patients with low, moderate, and high pretest probability, respectively, had DVT. According to Wells’ study, young patients undergoing ORIF with lower limb fractures were at moderate pretest probability (recent immobilization of the lower extremities and major surgery). Of the 150 patients included in our study, the overall incidence of VTE and DVT were 22.7% and 18.7%, respectively. We consider that the discrepancy of the incidence between our study and other studies may be due to the small sample size of 150 patients in our study. We hope further studies with larger sample size in this area would be performed.
In 1884, Rudolph Virchow first proposed that thrombosis was the result of at least 1 of 3 underlying etiologic factors: 1) vascular abnormalities and endothelial dysfunction, 2) hypercoagulability and 3) stasis. This theory was widely accepted during the following hundred years. We failed to find the original report from the database. So we cited the articles that support Rudolph Virchow’s theory. 24,25 For patients undergoing ORIF for lower extremities, trauma and operation lead to an injury of soft tissue and then activate tissue and clotting factors, promoting thrombosis; trauma and surgical stress cause platelet adhesion and lead to fibrin deposition and thrombosis; anesthesia cause peripheral venous dilated, tourniquet during operation, and postoperative immobility of fractured limb lead to stasis of venous blood flow.
From the present study, a highly significant deviation from the ROC was found in prediction of plasma
Based on our data, we propose
In 88.37% of all patients with plasma
Limitations
Our study has several limitations. First, we diagnosed DVT or PE with Doppler ultrasonography or CT, however, venography is considered as the gold standard for diagnosis of DVT or PE because venography is invasive, and there is a risk that the examination itself may cause a PE.
26
Several studies have demonstrated the value of Doppler ultrasonography or CT for diagnosis of DVT or PE,
27
–29
and we believe that our results were reliable. Second, our finding partially contradicts other studies
22
that have demonstrated a higher risk of VTE in patients with older age, thus further studies are needed. Third, our study was performed among young patients undergoing ORIF for lower limb fracture, and we hope further study is needed and
Conclusion
Using a threshold of 3 mg/L, plasma
Footnotes
Authors’ Note
Yong Yang and Pengfei Zan contributed equally to the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.