
Abstract
The hypercoagulable state accompanying inflammatory bowel diseases (IBDs) is still poorly understood. The aim of this study was to assess antiphospholipid antibodies (APAs) and a large panel of inherited and acquired thrombotic markers simultaneously in a sample of Tunisian patients with IBD. In total, 89 consecutive patients with IBD (mean age 38 ± 15 years; 48 with Crohn disease and 41 with ulcerative colitis) and 129 controls were prospectively evaluated for immunoglobulin (Ig) G, IgM, and IgA antibodies against cardiolipin (aCL), β2glycoprotein I (aβ2GPI), and prothrombin (aPT); IgG and IgM antibodies against phosphatidic acid (aPA), phosphatidylinositol (aPI), and annexin V (aAnnV); lupus anticoagulant (LA); coagulation factors; natural inhibitors; and thrombotic genetic polymorphisms. Levels of fibrinogen, factors II, V, and VIII and von Willebrand factor, antithrombin, and protein C were significantly higher in patients with IBD than in controls (P < .05 for all comparisons). At least 1 APA subset was detected in 54 patients. The frequencies of antibodies against anionic phospholipids—aCL, aPI, and aPA—in patients with IBD were 15.9%, 21.3%, and 14.6%, respectively. The frequencies of antiphospholipid cofactor antibodies were 39.8% for aβ2GPI and 15.7% for both aAnnV and aPT. Isolated aβ2GPI IgA was detected in 22 patients, and 12 (13.5%) patients had LA. The IgA aβ2GPI antibodies were frequently detected in Tunisian patients with IBD. These results are of potential diagnostic, prognostic, and therapeutic interest.
Introduction
Patients with inflammatory bowel diseases (IBDs) have a higher than normal risk of thromboembolic complications, which occur in 1% to 7.7% of cases, particularly in the presence of active disease. 1 –3 The risk of thrombosis has been attributed to a hypercoagulable state, the mechanism of which is not well understood. Hypercoagulability is frequently observed in IBD and has been implicated in both the pathogenesis and the morbidity of the disease. 1,2 Many inherited and acquired hemostatic abnormalities associated with the hypercoagulable state in patients with IBD may account for the higher risk of thrombosis: thrombocytosis, 1,4 high concentrations of clotting factors, such as fibrinogen, 1,3,5 factor V (FV), 1,3,6 factor VII (FVII), 1,3 and factor VIII (FVIII), 1,3,6 a dysregulation of natural anticoagulation, 1,3,7,8 and fibrinolytic activity. 1,3 The role of hyperhomocysteinemia and other inherited thrombophilia factors, such as factor V Leiden G1691A (FVL) and the G20210A prothrombin gene mutation, has also been evaluated. 1,3,9 However, conflicting results have been published concerning the association of these markers with IBD and their precise role in the occurrence of thrombotic events. Moreover, there is a growing evidence to suggest that antiphospholipid antibodies (APAs) play a role in the pathogenesis of both arterial and venous thrombotic events. 10
Antiphospholipid autoantibodies belong to a group of heterogeneous autoantibodies directed against phospholipids and their protein cofactors. The APA may contribute to the hypercoagulable state in patients with IBD and their prevalence differs considerably between ethnic groups and regions. The occurrence of APA is thus influenced by anthropological factors. Studies assessing the clinical relevance of APA have involved principally the characterization of anticardiolipin (aCL) and anti-β2glycoprotein I (aβ2GPI) antibodies, which are included in the definition of antiphospholipid syndrome, whereas antibodies with other specificities and lupus anticoagulant (LA) are rarely considered. 3,11 Moreover, APAs are frequently considered alone, without reference to the global hypercoagulability profile of patients with IBD. Nevertheless, thrombosis in patients with IBD may result from interactions between multiple acquired and inherited factors. 3,11
The aim of this study was to evaluate the frequency of positive APA subtypes in a series of Tunisian patients with IBD and healthy controls (blood donors) and to assess their correlation with disease activity. We also investigated a large panel of inherited and acquired thrombotic risk factors.
Patients and Methods
Patients
Over a 2-year period, 89 consecutive patients with IBD followed up as outpatients or inpatients at the Gastroenterology Unit of Sahloul Teaching Hospital (Sousse, Tunisia) were prospectively enrolled in the study. In all, 48 patients had Crohn disease (CD) and 41 had ulcerative colitis (UC). Informed consent was obtained from the patients, and the study was approved by the local ethics committee.
Diagnosis was based on medical history, clinical examination, endoscopic, radiologic, and histopathologic criteria. Disease activity was assessed, at the time of the study, on clinical scales based on the Crohn’s Disease Activity Index 12 and Truelove-Witts criteria 13 in patients with CD and UC, respectively. Crohn disease was classified as quiescent (score <150), mildly to moderately active (score between 150 and 450), or severe active (score >450) disease. Similarly, UC was classified as quiescent, mildly active, moderately active, or severe by assessing the following criteria: number of stools per day, blood in the stools, fever, tachycardia, hemoglobin level, and erythrocyte sedimentation rate.
For comparison, we included a group of 129 healthy blood donors matched for age, sex, and ABO blood group. None of the controls had a history of arterial hypertension, hyperlipidemia, diabetes, or thrombosis. All controls and patients were from the central area of Tunisia.
Samples
Venous blood samples for coagulation tests were collected in plastic tubes containing sodium citrate (0.1 mol/L; 1:10) before the initiation of anticoagulant therapy. Plasma was obtained by 2 rounds of centrifugation at 2500g for 15 minutes each. Aliquots of plasma were then frozen at −80°C until use. Blood samples for platelet counts and DNA extraction were collected in tubes containing EDTA. For APA determinations, blood was collected into dry tubes, and serum was isolated and stored at −80°C.
Coagulation Study
Platelet count was determined with a hematological analyzer (XT2000i; Sysmex, Japan). Coagulation tests were performed on a coagulation analyzer (STA Compact; Diagnostica Stago, France). Standard techniques were used to determine prothrombin time, activated partial thromboplastin time (APTT), and thrombin time (Neoplastine CI plus, PTT-A, Thrombin; Diagnostica Stago). Fibrinogen was determined by the Clauss method (STA-fibrinogen; Diagnostica Stago), whereas factor II (FII), FV, FVII, factor XI (FXI), and FVIII were determined by 1-stage assays with factor-deficient plasma (Diagnostica Stago). Von Willebrand factor (vWF) antigen was determined by immunoturbidimetry (Liatest FvW; Diagnostica Stago). Factor XIII (FXIII) activity was determined by a chromogenic method (Berichrom FXIII, Siemens Healthcare, Germany).
Antithrombin (AT) activity was measured by a chromogenic method, with the STA-Stachrom AT assay (Diagnostica Stago). Free protein S (PS) antigen was determined by immunoturbidimetry, with the STA-Liatest Free PS kit (Diagnostica Stago). Protein C (PC) activity was assessed by a clotting method, with the STA-Staclot PC assay (Diagnostica Stago). Functional activated protein C resistance (APCR) was assessed with the STA-Staclot APCR kit, an APTT-based method, with FV-deficient plasma (Diagnostica Stago). We assessed the possible effect of inflammation on coagulation abnormalities by determining acute-phase protein C-reactive protein (CRP) with routine laboratory techniques (normal: <5 mg/dL).
Characterization of Antiphospholipid Antibody
Lupus anticoagulant was detected according to the criteria of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. 14 Screening and confirmation procedures were carried out with the following 3 tests: APTT with 4 different commercial reagents (CK-Prest, PTT-A, and PTT-LA; Diagnostica Stago and Pathromtin; Siemens Healthcare); the tissue thromboplastin inhibition test, at a dilution of 1:500 (Neoplastine CI plus; Diagnostica Stago); and the dilute Russell viper venom test (LA1, LA2; Siemens Healthcare, Germany).
Commercial enzyme-linked immunosorbent assay (ELISA) kits (Orgentec Diagnostica; Mainz, Germany) were used to determine serum levels for the following APAs: immunoglobulin (Ig) G, IgM, and IgA for aCL, aβ2GPI and antiprothrombin (aPT) antibodies; IgG and IgM for antiphosphatidic acid (aPA), antiphosphatidylinositol (aPI), and antiannexin V (aAnnV) antibodies.
The procedures and cutoff values used have been reported elsewhere. 15 Titers >7 MPLU/mL for IgM aCL, >8 U/mL for IgM, IgG, and IgA for aβ2GPI and IgM and IgG for aAnnV, >10 U/mL for aPT, and >10 GPL U/mL (MPL U/mL or APL U/mL) for the other APA were considered to be positive. These values were close to the 95th percentile for a group of healthy Tunisian blood donors. Antiphospholipid antibody titers above 40 units/mL were considered to be moderate or high, as suggested by Miyakis et al. 16
We assessed the possible association between high total serum IgA levels and positivity for the APA IgA subset, by testing serum samples from patients with this subset of APA for total IgA in a nephelometry assay (normal range: 70-380 mg/dL).
Genetic Study
DNA samples were extracted from whole-blood samples collected in EDTA, with a commercial DNA isolation kit (Wizard Genomic; Promega, Madison, Wisconsin). We tested for the FVL, prothrombin G20210A, and methylene tetrahydrofolate reductase (MTHFR) C677T and A1298C mutations by polymerase chain reaction restriction fragment length polymorphism, as described previously. 17
Statistical Analysis
The results obtained are expressed as means ± standard deviations (SDs), together with the range, for normally distributed variables, or as medians ± interquartile ranges, together with the range, for variables not conforming to a normal distribution (ELISA-based APA titers and levels of fibrinogen and vWF).
Chi-square tests were performed to compare frequencies between groups. The Mann-Whitney rank sum test was performed to compare ELISA-based APA titers and levels of fibrinogen and vWF between groups. Student t test was used to compare the means of the other hemostatic variables between groups. Differences in hemostatic variables between the 4 stages of the disease were analyzed by variance analysis or Kruskal-Wallis tests. Spearman rank correlation test was used to evaluate correlations.
GraphPad prism software (GraphPad, San Diego, California) version 6.0 Demo was used to generate ELISA-based APA titer distribution graphs. SPSS-13.0 software was used for the statistical analysis, with P < .05 considered significant in 2-tailed tests.
Results
The demographic and clinical features of patients with IBD are summarized in Table 1. Disease was active in 42 patients and quiescent in 47, as defined in the Patients and Methods section. At the time of the study, 72 patients were on medical treatment, 5 (5.6%) patients had undergone surgical treatment but none were on antithrombotic drugs or hormonal treatments (oral contraceptives). Mean disease duration was 42 months (range: 1-216 months).
Demographic and Clinical Features of Patients With Inflammatory Bowel Disease.
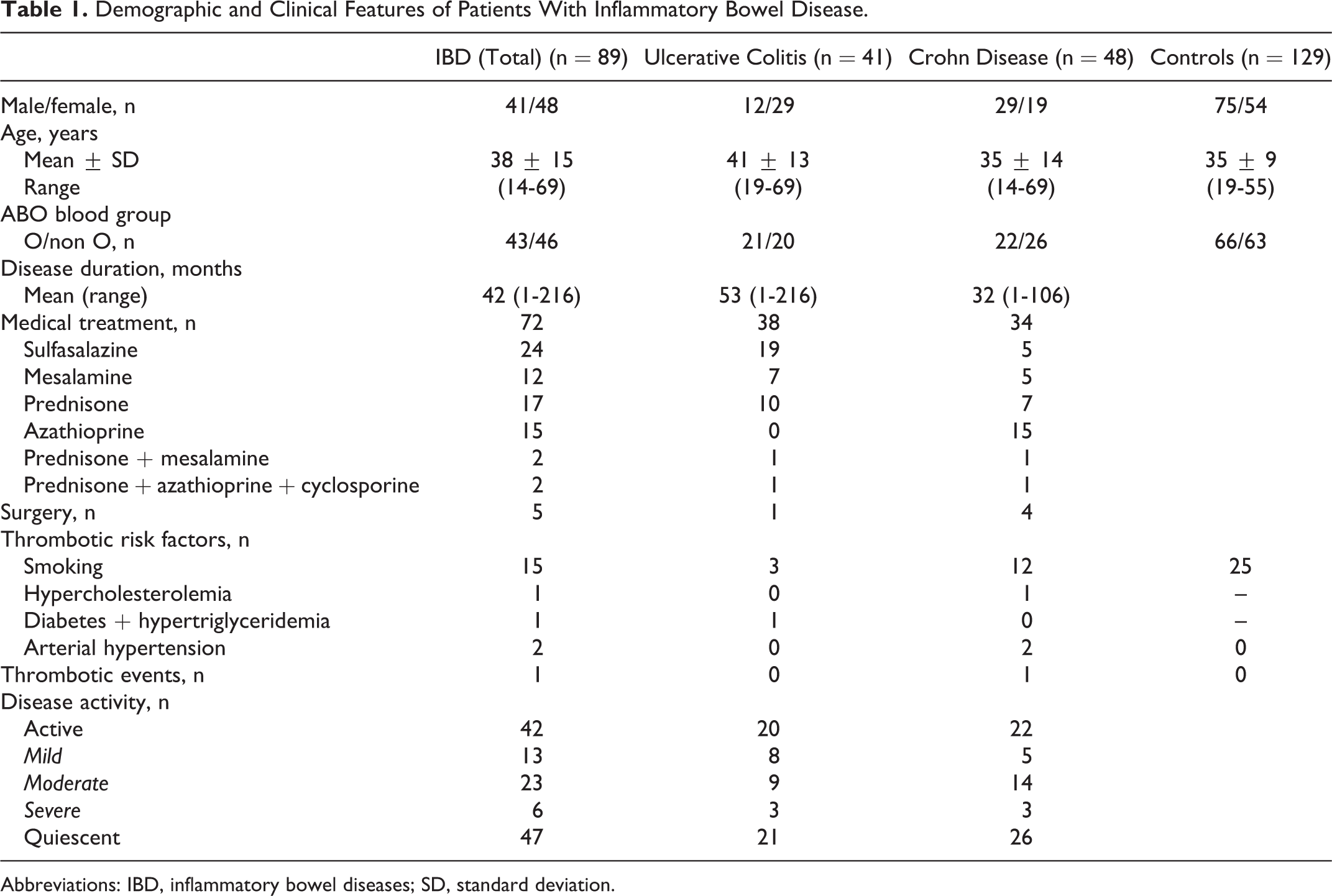
Abbreviations: IBD, inflammatory bowel diseases; SD, standard deviation.
One 48-year-old female patient had a history of deep venous thrombosis of the left leg 3 months before the onset of clinical symptoms leading to diagnosis of CD. The patient presented with inactive disease and was free of thrombosis at the time of the study. She was heterozygous for FVL and had the MTHFR A1298C mutation and high levels of coagulation factors II, V, VII, VIII, and fibrinogen. She also had low aPI IgG titers.
Coagulation Study
Platelet count did not differ significantly between patients with active IBD (mean ± SD: 301 ± 97 ×109/L) and patients with quiescent disease (mean ± SD: 298 ± 104 × 109/L). Thrombocytosis (platelet count >4 × 109/L) was observed in 18.2% of patients with IBD, with no difference in frequency between patients with active (17.1%) and quiescent (19.1%) IBD. The main coagulation parameters are presented, with comparisons between patients with IBD and controls and between active and quiescent disease, in Table 2. The levels of coagulation factors (fibrinogen, FII, FV, FVIII, and vWF) and of natural coagulation inhibitors (AT and PC) were significantly higher in patients with IBD than in controls, whereas no significant difference in FVII, FXI, FXIII, or PS levels was found between these 2 groups. FXIII levels were significantly lower in patients with active disease than in patients with quiescent disease. However, the levels of the other hemostatic factors were similar in patients with active IBD and those with quiescent disease. Nevertheless, among patients with active disease, mean FVIII levels were significantly higher in patients with severe IBD than in those with mild IBD (P = .012). The FVIII and vWF levels were higher in patients with non-O blood group than in group O patients with quiescent IBD (P = .047 for FVIII; P = .018 for vWF). In blood group O patients, the concentration of FVIII was significantly higher in patients with active IBD than in those with quiescent disease (P = .028).
Coagulation Parameters in Controls and in Patients With Inflammatory Bowel Diseases, as a Function of Disease Activity.
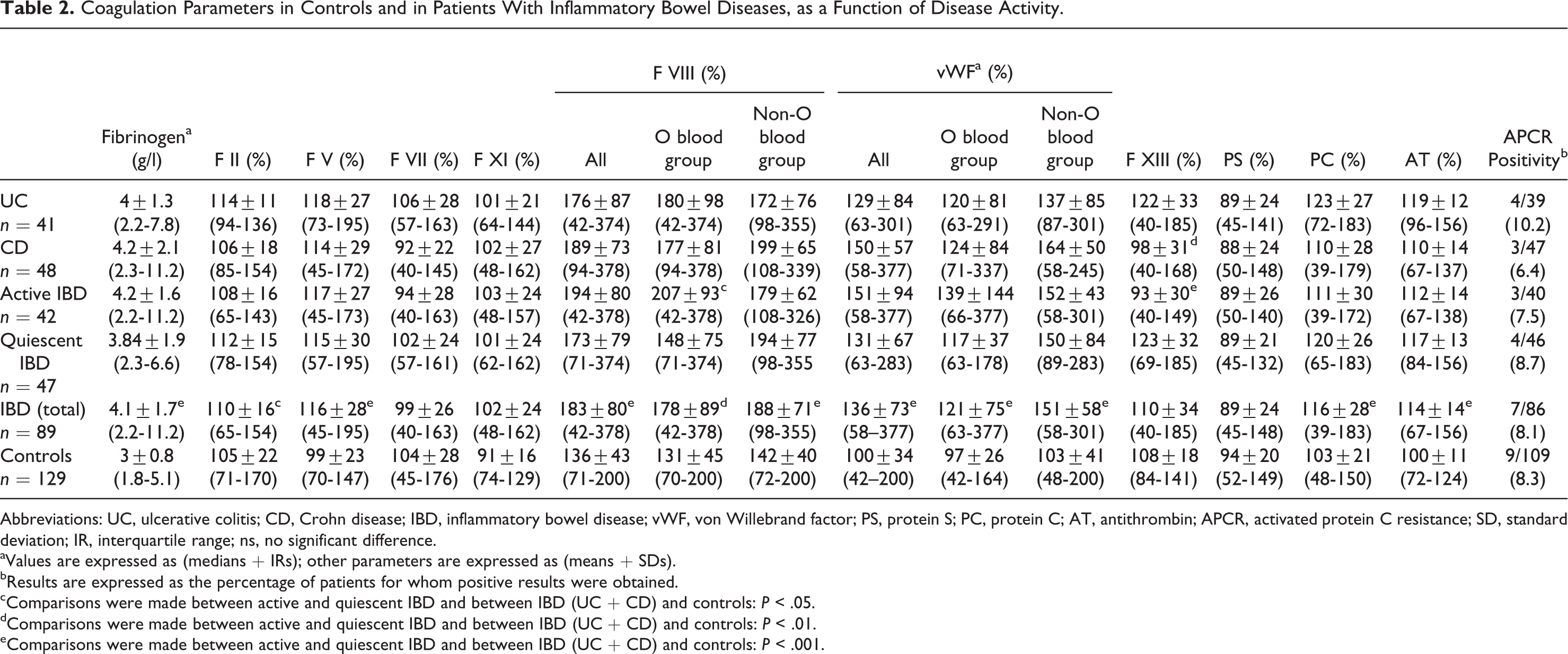
Abbreviations: UC, ulcerative colitis; CD, Crohn disease; IBD, inflammatory bowel disease; vWF, von Willebrand factor; PS, protein S; PC, protein C; AT, antithrombin; APCR, activated protein C resistance; SD, standard deviation; IR, interquartile range; ns, no significant difference.
aValues are expressed as (medians + IRs); other parameters are expressed as (means + SDs).
bResults are expressed as the percentage of patients for whom positive results were obtained.
cComparisons were made between active and quiescent IBD and between IBD (UC + CD) and controls: P < .05.
dComparisons were made between active and quiescent IBD and between IBD (UC + CD) and controls: P < .01.
eComparisons were made between active and quiescent IBD and between IBD (UC + CD) and controls: P < .001.
We assessed the influence of inflammation on the size of the increase in coagulation factor levels, by analyzing the correlation between fibrinogen, CRP, and other factors, such as FVIII, vWF, and FXIII in particular. Fibrinogen concentration was found to be weakly correlated with FVIII (Spearman, ρ = .227, P = .037), FV (Spearman, ρ = .381, P < .001), FII (Spearman, ρ = .328, P = .002), and FXI (Spearman, ρ = .375, P = .003) levels but not with vWF in patients with IBD. The FVIII and vWF concentrations were also correlated (Spearman, ρ = .463, P < .001). In patients with active IBD, no correlation was found between the concentration of fibrinogen and those of the other coagulation factors considered.
Concentration of CRP was correlated with vWF (Spearman, ρ = .29, P = .009) and fibrinogen (Spearman, ρ = .558, P < .001) levels but not with FVIII concentration in patients with IBD. Moreover, concentration of CRP was inversely correlated with FXIII activity (Spearman, ρ = −.293, P = .03).
Frequency of Inherited Thrombotic Markers
Of the patients with IBD, 4 (5.5%) were heterozygous for FVL, none (0%) had the G20210A prothrombin mutation, 41 (47.1%) had the MTHFR C677T mutation (30 heterozygous and 11 homozygous), and 43 (49.4%) had the MTHFR A1298C mutation (31 heterozygous and 12 homozygous). These frequencies were similar to those in controls, and no significant difference in the frequencies of these mutations was found between active and quiescent IBD.
Frequency of APAs
Of the 89 patients with IBD, 54 (60.7%) had at least 1 type of APA. The frequencies of antianionic phospholipid antibodies in patients with IBD were 15.9% for aCL, 21.3% for aPI, and 14.6% for aPA. Antiphospholipid cofactor antibody detection rates in patients with IBD were 39.8% for aβ2GPI and 15.7% for aAnnV and aPT. Lupus anticoagulant was found in 12 (13.5%) patients. The frequencies of the various types of APA and LA did not differ significantly between active and quiescent IBD (Table 3).
Frequencies of Antiphospholipid Autoantibodies in Patients With Inflammatory Bowel Diseases, According to Type of Disease (Ulcerative Colitis/Crohn Disease) and Disease Activity (Active/Quiescent).
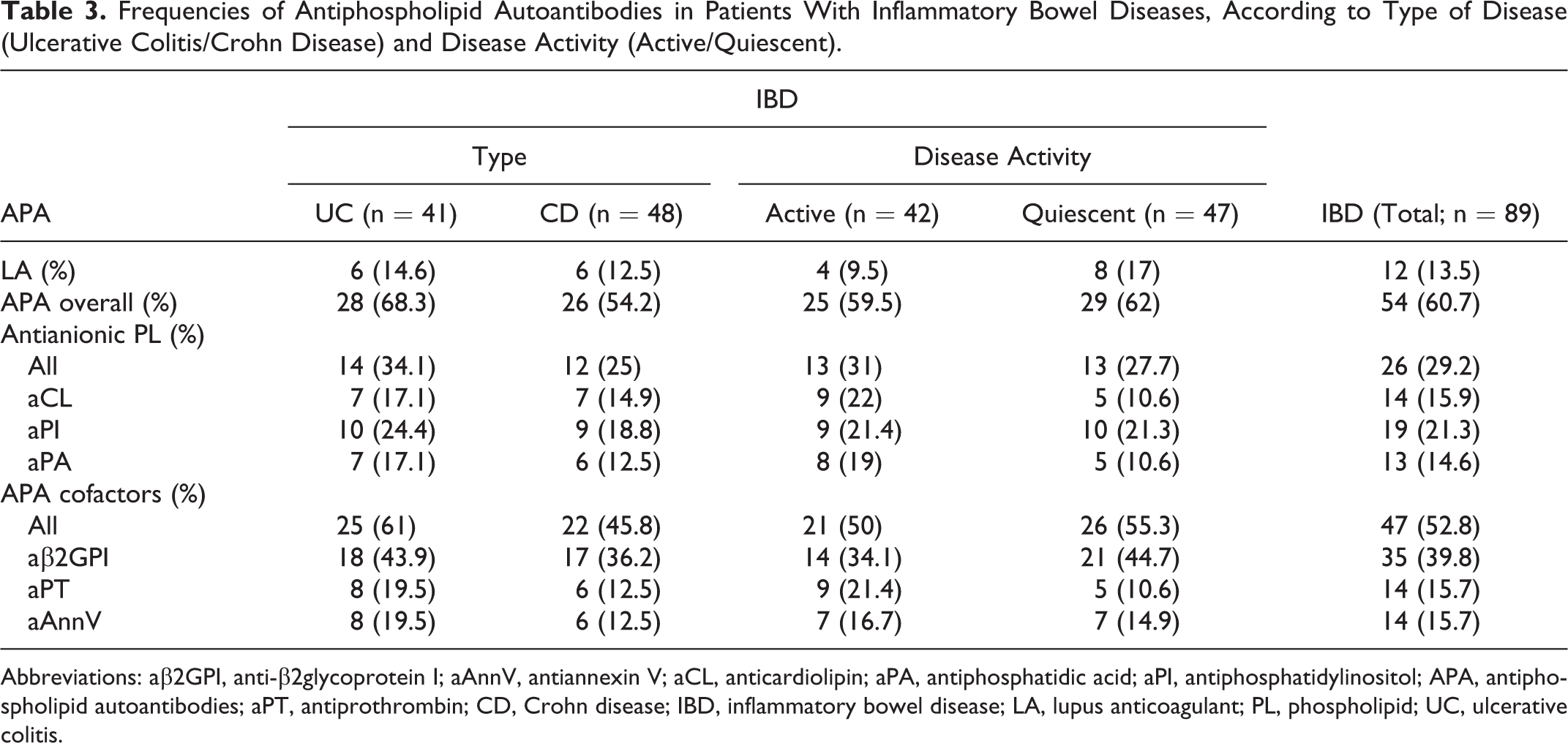
Abbreviations: aβ2GPI, anti-β2glycoprotein I; aAnnV, antiannexin V; aCL, anticardiolipin; aPA, antiphosphatidic acid; aPI, antiphosphatidylinositol; APA, antiphospholipid autoantibodies; aPT, antiprothrombin; CD, Crohn disease; IBD, inflammatory bowel disease; LA, lupus anticoagulant; PL, phospholipid; UC, ulcerative colitis.
The distribution of isotypes for the various APA subsets is summarized in Table 4. The frequency of APA isotypes did not differ between active and quiescent IBD. The IgA aβ2GPI was the most frequently detected isotype in our patients and was the only isotype detected in 22 (63%) cases.
Frequencies of Antianionic Phospholipid Antibodies and Anticofactor Antibodies and Their Isotypes in Patients With Inflammatory Bowel Disease.a
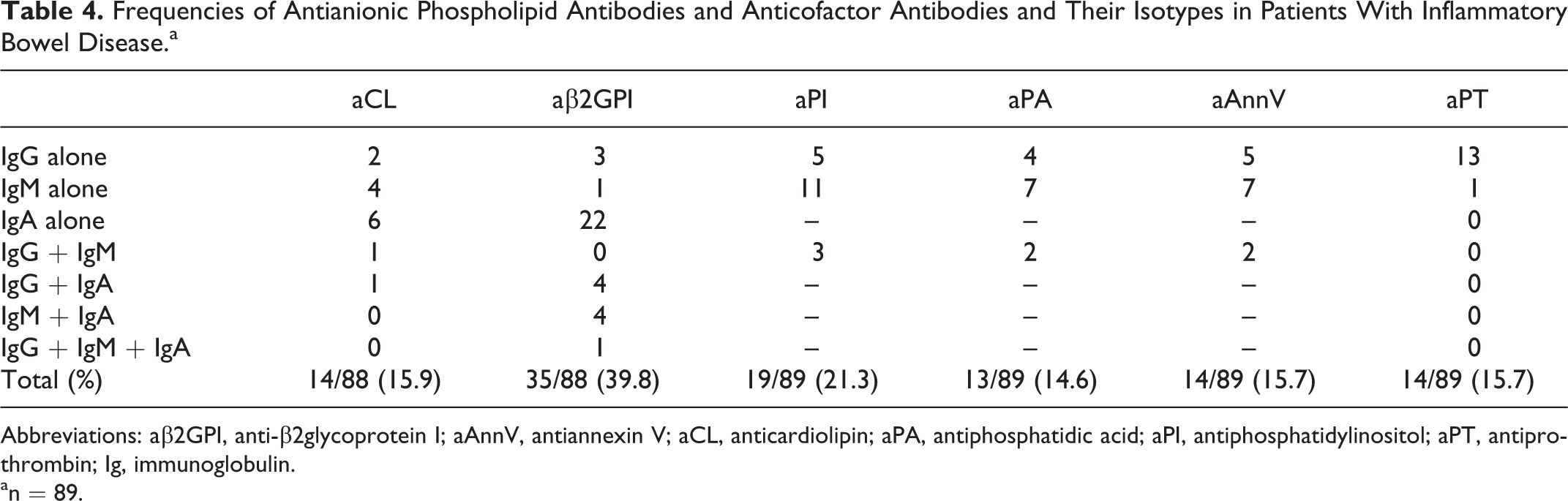
Abbreviations: aβ2GPI, anti-β2glycoprotein I; aAnnV, antiannexin V; aCL, anticardiolipin; aPA, antiphosphatidic acid; aPI, antiphosphatidylinositol; aPT, antiprothrombin; Ig, immunoglobulin.
an = 89.
The ELISA-based APA detection was associated with the presence of LA in 7 patients, as follows: IgM aPI; IgA aβ2GPI; IgG aAnnV; IgA aβ2GPI and IgM aAnnV; IgA aβ2GPI and IgM aPI; IgA aβ2GPI, IgM aPI, IgM aAnnV, and IgG aAnnV; and IgG aβ2GPI, IgA aβ2GPI, IgG aPI, IgM aAnnV, and IgG aPT.
Titers of APAs
The titers of the various APA are shown in Figure 1. Of the 54 APA-positive patients, 16 (29.6%) had moderate or high titers of APA arbitrarily defined as titers above 40 units/mL (9 with quiescent disease vs 7 with active disease).
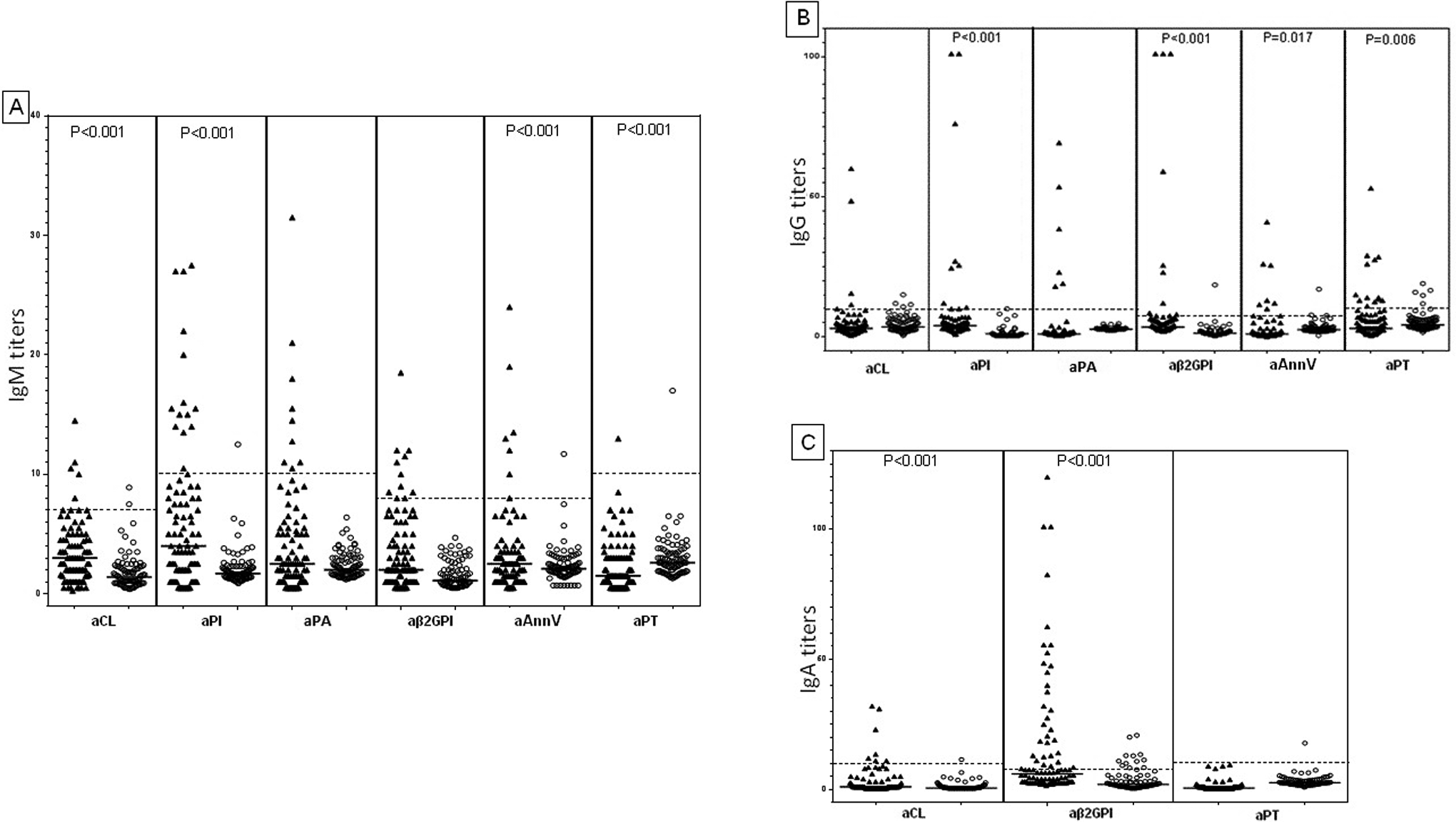
Distribution of antiphospholipid antibodies: anti-cardiolipin (aCL), anti-phosphatidylinositol (aPI), anti-phosphatidic acid (aPA), anti-β2glycoprotein I (aβ2GPI), anti-annexinV (aAnnV), and anti-prothrombin (aPT) antibody titers in patients with IBD (
Serum total IgA levels in 9 patients with high IgA aβ2GPI titers (from 40 to 120 U/mL) varied between 170 and 432 mg/mL. The IgA levels were in the normal range (70-380 mg/mL) in 8 patients and slightly high (432 mg/mL) in the remaining patient.
Persistence of APA
Only 16 of the 54 APA-positive patients were reevaluated at least 3 months later: 13 remained positive, but negative results were obtained for the other 3. Two patients also had LA, which persisted for more than 3 months in one and disappeared in the other.
Discussion
This prospective study identified APA as the major prothrombotic abnormality associated with IBD in Tunisians. The frequency of APA was high, and we detected LA and APA of various specificities by ELISA, in both patients with UC and CD. The IgA isotype of aβ2GPI was the most prevalent APA subset found in our patients. Hemostatic deregulation, with high levels of coagulation factors, was also demonstrated. However, none of these abnormalities were correlated with disease activity.
Conflicting findings have been published concerning the hemostatic abnormalities in patients with IBD. The significant increase in fibrinogen, FV, FVIII, and vWF levels observed in our patients with IBD is consistent with the findings of many previous studies. 5,6,18 –21 Moreover, this and other studies have shown that these abnormalities are not correlated with disease activity. 22 However, some authors have reported significantly higher levels of fibrinogen, 21 FV, 6 FVIII, 6 and vWF 6,18,21 in the active form than in inactive IBD. Consistent with the findings of Chiarantini et al, 5 we found that FXIII levels were lower in patients with active IBD than in those with inactive disease. We found no difference between patients with IBD and controls in terms of PS levels or the frequency of FVL, prothrombin G20210A, MTHFR C677T, and A1298C polymorphisms. However, our patients had significantly higher levels of PC and AT than healthy blood donors. Saibeni et al and Zezos et al also reported high PC levels in 74 IBD 19 and 51 UC cases, 23 respectively. Conversely, some studies have reported lower concentrations of PC, 7 PS, 7,8,23 and AT 7,21 in patients with IBD than in controls, with significant correlations between these abnormalities and disease activity. 7,20 Such findings require confirmation in larger series. A number of biases relating to the size of the series studied, the inclusion criteria, disease stage, and methods of determination used may account for these discrepancies. The hemostatic abnormalities observed in patients with IBD may be related to the interaction between chronic inflammation and the coagulation cascade. 11 Alternatively, they may be a primary feature of IBD that worsens during active disease. 22 Further studies are required to determine the real involvement of these mechanisms in the pathogenesis of thrombosis and IBD.
The prevalence of APA in IBD has rarely been studied, and the data published to date concern aCL antibodies, 4,5,8,24 –27 aβ2GPI antibodies, 4,25 aPS antibodies, 28 and LA. 5,21 Our study is the first, to our knowledge, to have assessed the frequencies of aPI, aPA, aAnnV, and aPT antibodies in patients with IBD.
Only LA and the IgG and IgM isotypes of aCL and aβ2GPI are included in the definition of antiphospholipid syndrome, 16 a clinical and biological entity characterized by the presence of at least one of the aforementioned APA together with the occurrence of thrombosis or recurrent fetal loss. However, many other studies have suggested that other APA with other specificities may also be associated with these complications. 29
The frequency of aCL antibodies (15.9%) was high in our patients with IBD. Similar findings have been reported for many previous studies, with aCL antibody frequencies of between 9.4% and 27%. 4,5,8,24,25,27 By contrast, Souto et al 28 and Webberley et al 26 reported a low frequency (1% and 0.9%, respectively) of aCL in patients with IBD.
Few data are available concerning the frequency of aβ2GPI in patients with IBD. Lonjon et al 25 and Koutroubakis et al 4 reported a frequency of 1.7% in 138 patients with CD and of 8.6% in 128 patients with IBD, respectively. The frequency of aβ2GPI antibodies obtained for our patients (39.8%) is the highest ever reported. The antibodies detected were mostly of the IgA isotype. Interestingly, IgA was the only isotype detected in 63% of cases. The IgA aβ2GPI has been detected in patients with antiphospholipid syndrome, systemic lupus erythematosus, and several other diseases, 30 –32 but the frequency of IgA aβ2GPI in patients with IBD has never before been reported. It is possible that the detection of IgA aβ2GPI in our patients is a false-positive finding resulting from nonspecific binding attributable to high concentrations of IgA immunoglobulins, a common feature of bowel disease. 33 We checked total serum IgA levels in some of our patients with aβ2GPI, but none were found to have high total IgA levels. Patients with IBD have been reported to display IgA autoreactivity against various human antigens. 34 We can therefore conclude that IgA aβ2GPI production may result, at least partly, from this autoimmune mechanism and that it may be triggered by inflammation. Conversely, our findings are consistent with previous suggestions that the IgA APA isotype may be a genetic marker in some populations, supporting recommendations to revise the laboratory criteria for APS and to include testing for IgA aβ2GPI in such populations. Nevertheless, it remains unclear how the immune response to β2GPI is generated and biased toward IgA production. A genetic polymorphism of β2GPI has been characterized that might affect APA production. 35
None of the APA-positive patients with IBD, including those with high titers of APA on ELISA or of LA, had thrombosis. However, we investigated the persistence of the APA in only a few cases, so we cannot entirely rule out the possibility of subclinical thrombosis. Moreover, thrombosis is a multifactorial condition that often results from the interaction of several risk factors, including hereditary, acquired, and environmental factors. The absence of thrombosis should not lead to an underestimation of the pathogenic role of IgA APA, the prevalent subset in our patients with IBD. Indeed, IgA aβ2GPI has been reported to recruit β2GPI to the surface of macrophages and endothelial cells highly efficiently and is thus highly effective at triggering thrombosis. 36
Further well designed, large prospective studies on patients from different ethnic groups are required to determine whether genetic differences underlie the epidemiological pattern of disease and to determine the precise pathogenic significance and clinical relevance of IgA aβ2GPI. Caution is required in the interpretation of our results, due to the small size of the series, the short follow-up period, the lack of APA persistence assessments for most patients, and a lack of evaluation of the effect of drug treatments.
In conclusion, the hemostatic profile of patients with IBD is characterized by several abnormalities. Antiphospholipid autoantibodies, mostly IgA aβ2GPI antibodies, emerged as a frequent feature of this disease among Tunisian patients. This finding may have implications for diagnosis, prognosis, and treatment. Further large-scale prospective studies are now required to determine the precise etiopathogenic role and clinical relevance of this marker.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.