
Abstract
The close relationship between inflammation and thrombosis affects the progression and severity of inflammatory bowel disease (IBD). The prevalence of venous thromboembolism (VTE) varies between 1% and 7% among patients with IBD. The VTE risk in patients with IBD is at least 3 times higher than that in the normal general population. The absolute risk is very high during hospitalization, active disease, and surgery. The IBD-related VTE occurs at younger ages and recurs more frequently. The development of thrombosis in IBD is due to the interaction of many hereditary and acquired risk factors. Each patient diagnosed with IBD should be evaluated for a personal and family history of thrombosis and for prothrombotic drug use. Although procoagulant factors are increased during the natural course of inflammation, natural anticoagulants and fibrinolytic activity are decreased. Although IBD is accepted as a prothrombotic condition, there is no treatment that can remove this risk from daily practice. Patient training is required to control important factors, such as long-term immobilization and smoking. Oral contraceptives and hormone replacement therapy should be avoided. Inducing permanent disease remission must be the key approach for the prevention of thrombosis. Low-molecular-weight heparin (LMWH) is the basis of prophylactic treatment, which reduces the thrombosis risk by 50%. Prophylaxis with LMWH should be administered to all patients with IBD hospitalized due to disease attack or surgery. Long-term or even life-long anticoagulation therapy should be planned if there is insufficient disease control, recurrent VTE attacks, positive thrombophilia tests, or thrombosis in vital veins.
Keywords
Introduction
The close relationship between inflammation and thrombosis, as observed in many other inflammatory diseases, affects the progression and severity of inflammatory bowel disease (IBD), which is composed of 2 main types, Crohn disease (CD) and ulcerative colitis (UC). 1 It is known that the risks of arterial and venous thrombosis have increased in IBD since they were first reported in 1936 by Bargen and Barker. 2 Although nearly 80 years have passed, the interaction between IBD and thrombosis has still not been clearly defined. Although thrombosis is accepted as an ordinary complication by some authors, many authors believe that it is the most common extraintestinal sign and/or plays an important role in the etiopathogenesis of IBD. 3 –6 In the present article, we try to describe the main aspects of the relationship between IBD and thrombosis and summarize the prevention and treatment recommendations.
Thromboses are commonly observed in deep leg veins and the pulmonary system. Less frequently, the cerebrovascular system, portal vein, mesenteric vein, hepatic veins, and retinal veins are also affected. Thrombosis prevalence varies between 1% and 7% in patients with IBD, and the rate is increased up to 39% to 41% in autopsy series. 2 –9 The thrombosis rate is higher than other well-known extraintestinal manifestations of IBD, such as primary sclerosing cholangitis, erythema nodosum, and pyoderma gangrenosum. Only spondyloarthropathies, which has a prevalence of 12% to 23%, are more frequent than thrombosis. 3,6,10,11
Epidemiology
In the retrospective cohort study by Bernstein et al, 12 investigating thrombosis risk in IBD, a total of 5529 patients with IBD were compared with individuals randomly selected at a 1:10 ratio from the general population between 1984 and 1997. In this important study, it was determined that the risks of deep venous thrombosis (DVT) and pulmonary embolism (PE) were increased 3- to 3.5-fold in patients with IBD compared with the general population. The risk was not affected by gender or type of IBD (UC or CD). On the contrary, the thrombosis risk in patients with IBD aged below 40 years was found to be 6-fold higher than that among same-aged individuals in the general population. A 7-year prospective observational study was performed on venous thromboembolism (VTE) in approximately 2 million individuals in the United Kingdom, and it was determined that VTE risk was increased in patients with IBD by 1.84-fold. 13 In this study, 17 diseases were evaluated for VTE risk, and only cancer and cardiac failure were found more risky than IBD.
Grainge et al 14 also reported important findings in their retrospective cohort study performed on 13 756 patients with IBD. Although the general VTE risk among patients with IBD was 3.6-fold higher than that among controls, the risk was increased up to 8.4-fold during the acute attack period and 6.5-fold in the presence of chronic active disease. Although VTE risk was decreased during the remission period, it was again 2.1-fold higher than the general population. In a retrospective Danish study performed on nearly 50 000 patients with IBD, it was reported that VTE risk was increased 2-fold, and the relative risk was increased in inverse proportion with age, despite increased thrombosis incidence with age. 15 In this Danish study, the thrombosis risk of patients with CD was found to be slightly higher than that of patients with UC. Nguyen and Sam 16 evaluated patients who were hospitalized because of VTE and found that the mortality risk was 2.1-fold higher in patients with IBD. Additionally, they reported that the patients with IBD stayed longer in the hospital. In contrast to the Danish study, 15 according to Nguyen and Sam, 16 VTE risk was higher in patients with UC than in patients with CD. In a study investigating recurrences, it was determined that the recurrence of a VTE attack was 2.5-fold higher in patients with IBD. 17
Although no consensus was reached about the relationship between IBD and arterial thrombosis, there are data indicating that the risks of cardiac, cerebral, and mesenteric embolism are increased in patients with IBD, especially during the postoperative period among young patients with IBD. 3,5,17 –20 Meta-analysis data recently revealed that arterial thromboembolism and cardiovascular (CV) mortality were not higher among patients with IBD compared with the general population, but ischemic heart disease and mesenteric ischemia might be observed more commonly. 19
In a recently published meta-analysis, the correlation between IBD and VTE was confirmed. 21 It was determined in that meta-analysis that IBD increased VTE risk approximately by 2-fold. Furthermore, cases with UC might be at higher risk; the disease was active in 60% to 80% of patients during the VTE attack, and patients with CD having colonic involvement and patients with CD having pancolonic involvement were at greater risk.
Miehsler et al 22 performed a study investigating whether VTE risk was specific for IBD, and they compared IBD with rheumatoid arthritis as an inflammatory disease control and with celiac disease as an intestinal disease control. They proposed that the VTE risk was specific for IBD because they found that although the VTE risk was increased in IBD by 3.6-fold, no increase was detected in patients with rheumatoid arthritis or celiac disease. In addition, it is known that IBD is rarely seen in patients with hemophilia or von Willebrand disease. 23 Because of the presence of microthrombi, even in biopsies taken from normal-appearing intestinal mucosa, it is believed that thrombotic conditions might play a role, especially in the pathogenesis of CD. 24 Although it was proven that IBD was a specific risk factor for VTE, the pathogenetic relationship between VTE and IBD was not clearly defined. Many genetic and acquired factors that may cause thrombosis in IBD have been identified (Tables 1 and 2). At least 1 risk factor was determined, especially in young patients with IBD who were complicated by VTE. 25 In general, it can be claimed that the development of thrombosis in IBD is due to the interaction of many hereditary and acquired risk factors (Figure 1). Each patient diagnosed with IBD should be evaluated for a personal and family history of thrombosis and for prothrombotic drug use.
Hereditary Factors That Increase Thrombosis Risk in IBD.

Abbreviations: IBD, inflammatory bowel disease; PAI-1, plasminogen activator inhibitor type 1.
Acquired Factors That Increase Thrombosis Risk in IBD.
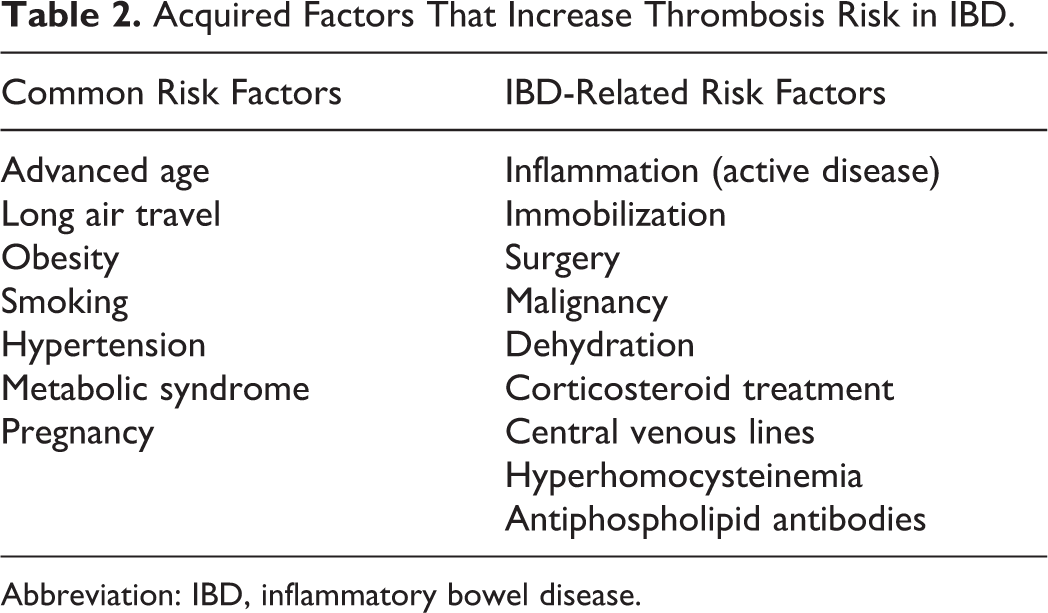
Abbreviation: IBD, inflammatory bowel disease.

Possible causes of thrombosis in patients having inflammatory bowel disease. APC indicates activated protein C; IBD, inflammatory bowel disease; MTHFR, methylene tetrahydrofolate reductase; PAI-1, plasminogen activator inhibitor type 1; tPA, tissue plasminogen activator.
Hereditary Risk Factors
Factor V Leiden (FVL) mutation is the name given to the Arg506Gln mutation in factor V, which is commonly encountered among Caucasians (2%-8%) and is more rarely observed among Asian, Africans, and American Indians. Coagulation factor V with this FVL mutation is resistant to breakdown (inactivation) by activated protein C (APC). 26 –28 As it is the most common hereditary thrombophilic factor in the general population, its relationship with IBD has been most widely investigated. Although it was determined meta-analytically that FVL mutation frequency was not different in patients with IBD compared with the general population, there are publications that have reported that it was more commonly seen in IBD as well as reports suggesting increased frequencies only in CD or only in UC. However, the common consensus is that FVL mutation frequency is not higher among patients with IBD, but its presence increases thrombosis risk, especially in younger patients with IBD (<45 years of age). 29 –31
It has been reported that protein S and antithrombin levels were also decreased along with protein C levels, especially during the activation period of patients with IBD. It has also been determined that phenotypic APC resistance was more common in patients with IBD (even during remission) compared with the healthy population. It should be emphasized that deficiencies in natural anticoagulants under such conditions may increase the tendency of thrombosis to occur. 32,33
Methylene tetrahydrofolate reductase (MTHFR) gene mutation increases both arterial and venous thrombosis risk by causing hyperhomocysteinemia. Although hyperhomocysteinemia is commonly observed in IBD, the frequency of the MTHFR mutation is not different in this population compared with the general population. Folate and vitamins B6 and B12 are important cofactors for this enzyme. Deficiencies in these vitamins are common in patients with IBD because of inadequate oral intake, insufficient absorption due to mucosal damage, and the effects of drugs, such as sulfasalazine. These deficiencies are among the important causes of hyperhomocysteinemia. Although hyperhomocysteinemia is common in patients with IBD, the relationship between hyperhomocysteinemia and thrombosis has not been definitively proven. 34,35
The presence of prothrombin gene mutation increases the risk of thrombosis, but a correlation was not found between IBD and prothrombin gene mutation. 29,30 Coagulation factor XIII val34leu mutation reduces the risk of thrombosis, but no difference has been identified in patients having IBD with or without thrombosis. 30 It has been reported that the plasminogen activator inhibitor type 1 (PAI-1) polymorphism is more common in patients having IBD with thrombosis, and the imbalance between PAI-1 and thrombin activatable fibrinolysis inhibitor may contribute to the hypercoagulability seen in IBD. 4,36 The prothrombotic risk factor and myeloproliferative disease indicator Janus kinase 2 mutation have been investigated in 48 patients with IBD having thrombosis, but it was not found in any of the patients. 37
Currently, it is accepted that there is no correlation between FVL, prothrombin gene, MTHFR mutations, and IBD. Although the very complicated genetics of IBD have not been clearly elucidated, they have been shown to be more commonly associated with genes located on chromosomes 12 and 16. 38 In contrast, hereditary prothrombotic gene mutations have been located on chromosomes 1 and 11. 39 Therefore, it is not surprising that there is no association between IBD and hereditary prothrombotic factors; however, it should be considered that in the presence of these prothrombotic risk factors, the risk of thrombosis is high in patients with IBD, similar to that in other patients with these prothrombotic risk factors. It should also be noted that when a patient with IBD develops thrombosis, the presence of these factors should be investigated.
Acquired Risk Factors
General factors, such as air travel, obesity, advanced age, and smoking, as well as IBD-related factors, such as hospitalization, long-term immobilization, surgical interventions, steroid treatment, and central venous catheters, also increase the risk of thrombosis (Table 2). 13 –15 There is a linear correlation between age and VTE. Nguyen and Sam 16 reported that an increase in 1 decade of age caused a 20% increase in thrombosis risk. Although the annual VTE incidence in patients with IBD ≤20 years of age was 85% lower than that in those ≥60 years of age, the relative risk of young patients with IBD was 4-fold higher than the relative risk of elderly patients with IBD compared with the general population. 15 In one study investigating factors increasing thrombosis risk, only steroid use was found significant, 40 but in another study, active disease, intestinal stenosis, and presence of fistula were determined to be significant. 17 The risk is increased not only in hospitalized patients but also in patients with IBD who are followed up at outpatient clinics with active disease. It has been proposed that patients with active disease may have a higher risk while waiting to be hospitalized than after they are admitted. 40 As mentioned above, thrombosis risk is further increased during active periods of the disease as well as in patients with chronic active disease and it is lower during remission. 14,17 The presence of IBD increases the risk of thrombosis among patients with emergent medical disease, and emergency disease increases the risk of thrombosis in a patient with IBD. Thus, the presence of IBD has been included in the thrombosis risk evaluation scales of hospitalized patients. 41
Inflammation and Thrombosis
It is well known that there is an uncontrolled chronic intestinal inflammation in IBD. Arachidonic acid metabolites (such as prostaglandin E2, thromboxane A2 (TXA2), and leukotriene B4), cytokines (such as tumor necrosis factor-α [TNF-α], interferon γ, and interleukins [IL-1, IL-2, and IL-8]), platelet-activating factor (PAF), and intercellular adhesion molecule are among the mediators that have important roles in aggravating chronic inflammation. Interleukin 4, IL-10, and IL-13 are mediators that inhibit inflammation. Transforming growth factor β acts in tissue healing. 42 The PAF increases thrombocyte aggregation and stimulation. 43 Interleukin 8 increases smooth muscle contraction. It has been shown that TXA2 increases thrombocyte aggregation, especially in CD, independent of disease activation. 4
Currently, it is known that systemic inflammation is a potent prothrombotic stimulant. 44 Although procoagulant factors are increased during the natural course of inflammation, natural anticoagulants and fibrinolytic activity are decreased (Table 3). Hemostatic changes observed in IBD are partly related to the activity and severity of the IBD. Thrombocytosis and decreases in mean platelet volume are directly related to active disease. Evidence clearly indicates that thrombocyte activity is increased in patients with IBD. It has been shown that prothrombin fragment 1 + 2 levels, which indicate the activation of the coagulation cascade, and fibrin(ogen) degradation products (FDP), which indicate the activation of the fibrinolytic system, are both increased continuously in patients with IBD independent of disease activity. 45 In one study, it was reported that FDP levels were significantly lower in patients receiving corticosteroids, and the authors claimed that the use of steroids increased the risk of thrombosis by reducing fibrinolysis. 40 In another study investigating the conversion of thrombin from prothrombin, which is an indicator of the activation of coagulation, thrombin generation was correlated with C-reactive protein levels and disease activity. Therefore, it was suggested that this increase in thrombin generation is related to the increased risk of thrombosis during the active period. 46 Additionally, an inhibition of the fibrinolytic system has been observed in patients with IBD. It was reported that tissue plasminogen activator (tPA) levels were decreased, but PAI-1 levels were increased in IBD. 45 Antibodies against coagulation compounds, especially phospholipids and protein S, are common in patients with IBD.
The Effect of Inflammation on Hemostatic Factors.
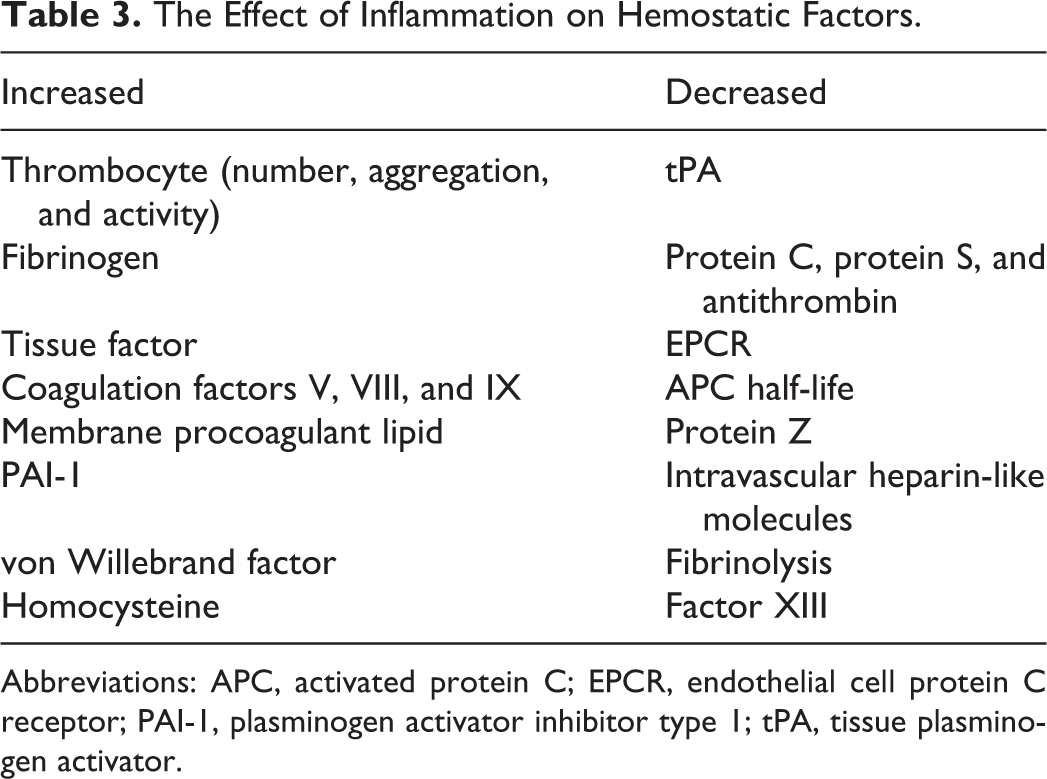
Abbreviations: APC, activated protein C; EPCR, endothelial cell protein C receptor; PAI-1, plasminogen activator inhibitor type 1; tPA, tissue plasminogen activator.
Drugs and Thrombosis
When drugs used in IBD were reviewed, it was theoretically expected that none of them would have thrombogenic effects, with the exception of thalidomide. 6 In a meta-analysis on patients with multiple myeloma, it was reported that the VTE risk was increased 2.6-fold with thalidomide, 2.8-fold with steroids, and 8-fold when both were used. 47 Prophylaxis with low-molecular-weight heparin (LMWH) or warfarin was found to be useful; however, there are no data for patients with IBD. The cases with CD receiving thalidomide should be closely followed up for thromboembolic complications if they are also receiving steroids.
Corticosteroids suppress fibrinolysis by increasing fibrinogen and decreasing tPA. 6,40 They also inhibit prostacyclin synthesis by decreasing arachidonic acid in the vessel wall. Therefore, platelet-derived thromboxanes become dominant and lead to increased vasoconstriction and thrombosis risk. It is expected that steroids that are indispensable agents in IBD treatment theoretically decrease prothrombotic risk by decreasing inflammation and tissue damage; however, as mentioned above, thrombosis risk is increased in patients with IBD receiving steroids, so these patients should be closely followed up.
It is hypothetically correct that 5-aminosalicylic acid (5-ASA) preparations may have antiplatelet effects because they are similar to acetylsalicylic acid. Studies performed in vitro on thrombocytes obtained from patients with IBD using 5-ASA did not prove this probable antiplatelet effect. Clinical experience has also shown that the use of 5-ASA does not increase bleeding. 6
Azathioprine inhibits adenosine diphosphate-dependent thrombocyte aggregation. Therefore, it is believed to have antithrombotic activity; however, a more important issue regarding azathioprine and 6-mercaptopurine is that these drugs may cause warfarin resistance in some patients. The mechanism of this resistance is unknown, but it necessitates 2.5-fold increases in the dose of warfarin. 48
As methotrexate is a folate antagonist, it may cause hyperhomocysteinemia. It has been reported that high homocysteine levels and folate deficiency may cause increased colorectal cancer risk in patients with UC, and folate treatment may decrease this risk. 49 Although oral folic acid replacement at 0.5 to 5 g doses decreases homocysteine levels by 25%, the addition of vitamin B12 provides an additional decrease of 7%, but vitamin B6 has no additional contribution. Giving 400 μg folic acid orally to patients receiving methotrexate is adequate to decrease homocysteine levels. Additionally, vitamin deficiencies should be investigated and corrected during the routine follow-up of patients with IBD. 6
Cyclosporine and tacrolimus are used in the treatment of fulminant colitis cases that are resistant to steroids. Studies have shown that cyclosporine decreases antithrombin levels and increases the aggregation of thrombocytes and the activation of endothelial cells in vitro. Cyclosporine-related DVT, PE, cerebral, and renal vein thrombosis have been reported clinically 50 ; however, it was determined in prospective studies that thromboembolic complications were not increased in transplant patients receiving cyclosporine or tacrolimus. 51 Therefore, it is difficult to conclude whether cyclosporine increases thrombosis risk.
Infliximab and adalimumab inhibit TNF-α, which is a proinflammatory and prothrombotic cytokine. The CD40/CD40L pathway is the most important pathway connecting inflammation and coagulation. These TNF-α-blocking agents suppress the CD40/CD40L pathway, which is increased in the mucosal microcirculation of patients with IBD. 52 Despite these potential anticoagulant properties, patients receiving anti-TNF therapies should also be followed up for thrombosis, similar to other patients with IBD, because there have been many reports of thrombosis in this patient population. 53
Heparin and IBD
Because IBD is a prothrombotic condition and because there are microthromboses even in normal-appearing intestinal mucosa of patients with IBD, heparin has been occasionally used in the treatment of patients with IBD. Heparin provides its anticoagulant effect by inhibiting coagulation factor X in the presence of antithrombin; however, heparin also has many immunomodulatory and anti-inflammatory effects, including TNF-α inhibition. 54,55 Heparin treatment was evaluated in cases with steroid-resistant UC in 3 studies published in the 1990s. 56 –58 Heparin was used at a 25 000 to 40 000 IU dose for 4 to 6 weeks so that the activated partial thromboplastin time was stabilized at 60 seconds, and remission rates varying between 54% and 90% were reported. Colonic bleeding, which was the most feared possible complication of heparin treatment, was observed in only 5% of the cases. In a study published in 1999, an LMWH, dalteparin sodium, was used at 2 × 5000 U dose subcutaneously on 12 steroid-resistant patients with UC for 12 weeks, and it was reported that half of the patients achieved complete remission, whereas 5 of the 6 remaining patients had partial clinical improvement. 59 The investigators did not report any side effects, and they proposed that LMWH treatment was a good alternative because of its safety; however, Shen et al 60 reported in a meta-analysis that neither standard heparin nor LMWH treatment was superior to conventional treatments.
Who Should Be Investigated?
A routine thrombophilia investigation is not recommended in healthy individuals without thrombosis. It is recommended that thrombophilia screening should be performed if the result would affect the treatment approach. Although IBD itself is a thrombophilic condition, and it is accompanied by many thrombotic risk factors, routine thrombophilia screening is not recommended in patients with IBD because it will not affect the decision of thromboprophylaxis; however, the thrombosis risk should always be considered. Family VTE history should be carefully investigated. If there is a history of heart attack or stroke among first-degree relatives younger than 50 years, recurrent pregnancy losses during the second and third trimesters of gestation, or DVT and PE of unknown origin in these patients, then they should be investigated in more detail. Another issue that requires emphasis is the necessity to complete all of the investigations conducted in the general population before deciding that this thrombosis is related to IBD, because it is possible that cancer may be the underlying cause that provokes the development of thrombosis in a patient with IBD. 61
Prevention/Treatment
Although IBD is accepted as a prothrombotic condition, there is no treatment that removes this risk from daily practice (Table 4). Patient training is required to control important factors, such as long-term immobilization and smoking. Oral contraceptives and hormone replacement therapy should be avoided. Inducing permanent disease remission must be the key approach for the prevention of thrombosis. If acute exacerbations of IBD are treated rapidly, the disordered coagulation factor profile and thrombocyte activation can be corrected, at least partially. Anticoagulant treatment may decrease inflammation. Hereditary thrombophilia screening should not be performed routinely, and it should be investigated only if there is a high risk in the family or if a patient has had a VTE.
Recommendations for the Prevention and Treatment of Thrombosis in Inflammatory Bowel Disease.a
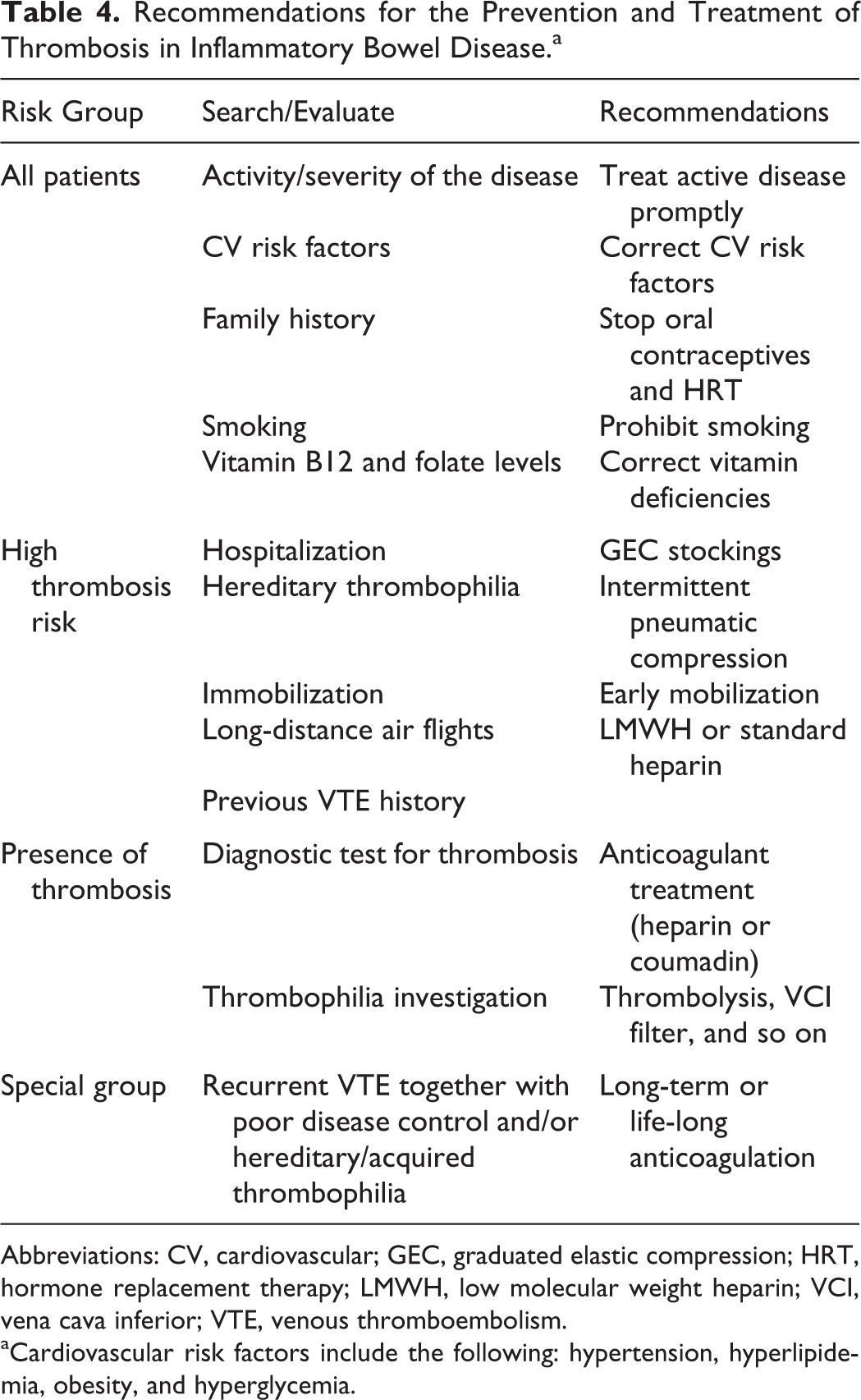
Abbreviations: CV, cardiovascular; GEC, graduated elastic compression; HRT, hormone replacement therapy; LMWH, low molecular weight heparin; VCI, vena cava inferior; VTE, venous thromboembolism.
aCardiovascular risk factors include the following: hypertension, hyperlipidemia, obesity, and hyperglycemia.
In situations that increase the risk of VTE (such as long-term immobilization, hospitalization, surgical intervention, or active disease), mechanical and pharmacological (with heparin or LMWH) prophylaxis should be performed (Table 4). This is also recommended in various consensus reports and guidelines. 62 –66 Heparin or LMWH is the basis of prophylactic treatment. In this way, the risk of thrombosis is reduced by 50%. The benefits of other preventive measures, such as graduated elastic compression (GEC) stockings, early mobilization, and the careful use and care of intravenous lines, is controversial. Although it has been established that heparin or LMWH is effective and should be used in prophylaxis, it is not clear how long patients should continue prophylactic treatment. Classically, prophylactic treatment is stopped when patients are discharged from the hospital; however, it seems reasonable to continue prophylactic LMWH treatment for some time after discharge because the disease activity continues during the early discharge period. This issue is not clear yet.
Another controversy surrounds the use of pharmacological prophylaxis in addition to mechanical measures during long air travels. A recent study determined that the VTE risk per long air travel is 1.6% among low-risk individuals and 5% among high-risk individuals. In the same study, it was found that GEC stockings only decreased DVT but not PE and PE-related deaths. 67 It is suggested that patients with IBD having active disease should also receive pharmacological prophylaxis as they are in the high-risk group. The current debate involves whether patients with inactive disease also require prophylaxis.
Several guidelines recommend routine heparin or LMWH prophylaxis for patients with IBD having particular risks (ie, hospitalization, surgery, active disease, or VTE history); however, only 30% to 50% of physicians dealing with patients with IBD are following this recommendation. 17,68 This issue should be considered seriously, and physicians treating patients with IBD should get accustomed to providing prophylaxis to these patients.
Although it is a medical truth that if a person has a cardiac risk factor, it should be defined and treated; such an approach is not encountered in clinical daily practice for patients with IBD. It should be considered that patients with IBD may also develop CV diseases, and they should also be investigated in this aspect. If hyperlipidemia or dyslipidemia is detected, then required treatment should be initiated. It is still debatable whether low-dose aspirin contributes to CD development. 69,70 There are few studies that indicate that aspirin use activates disease in patients with IBD. If a patient has to take aspirin due to CV disease, then he/she should be closely followed up. If aspirin does not activate the disease and is well tolerated by the patient, then treatment continuation should be recommended.
When an acute thrombosis attack occurs, all required standard treatments (including heparin, LMWH, aspirin, warfarin, mechanical treatment, surgical thrombectomy, and inferior vena cava filter) should be applied. It is well known that full-dose heparinization can increase bleeding from diseased intestines, but this risk is smaller than the risk of an acute thromboembolic attack in a patient who is not adequately anticoagulated. The use of new anticoagulants, such as anti-IIa/anti-Xa inhibitors and fondaparinux, in patients with IBD is not yet clear. New studies should be performed on this subject. Additionally, the duration of anticoagulant treatment after an acute attack is undefined. The recurrence of VTE events is higher among patients with IBD. If remission is induced after the first VTE event developed during active disease, then anticoagulant treatment can be stopped after 3 to 6 months. Long-term or even life-long anticoagulation therapy should be indicated if there is insufficient disease control (chronic active disease), recurrent VTE attacks, positive thrombophilia tests, or thrombosis in severe risk areas, such as the hepatic veins (Figure 2).

Management algorithm of acute thrombosis attack in inflammatory bowel disease. CT indicates computerized tomography; IBD, inflammatory bowel disease; LMWH, low-molecular-weight heparin; MRI, magnetic resonance imaging; USG, ultrasound; VTE, venous thromboembolism.
In recent years, the main topic of discussion has been whether thromboprophylaxis is being performed in patients who require it most. 71 It is not yet clear whether prophylaxis is required in patients who have an acute attack of IBD at home without requiring hospitalization. Although the risk of thrombosis was 6-fold lower in these patients than in hospitalized patients, they still have a higher risk than the normal population. Nguyen and Sharma recently published 2 interesting studies. In their first study performed using the Markov decision analysis method, they proposed that anticoagulant prophylaxis decreased VTE risk during IBD attacks in patients who were not hospitalized, but it was not cost-effective. 72 In the second study performed via the same method, they claimed that anticoagulant treatment extended for up to 5 years was both more effective and more cost-effective compared with short-term anticoagulation therapy in patients with IBD who had VTE without any provoking causes. 73 A study from surgery clinics reported that VTE risk was increased by 2.7-fold in patients with IBD when patients who underwent bowel surgery due to colon cancer were compared to those who had surgery for IBD. Therefore, it was proposed that anticoagulant therapy should be performed in patients with IBD for at least 4 weeks after discharge, as was the case with patients having surgery for colon cancer. 74
The Canadian Association of Gastroenterology recently performed an innovation and published a consensus for the risk, prevention, and treatment of VTE in IBD. 75 According to the main principles of this consensus, (1) VTE risk in patients with IBD is 3-fold higher than that in the normal general population, and the absolute risk is very high during hospitalization; (2) moderate–severe disease activity is an important factor that increases VTE risk, and it should be accepted as a provoking factor; and (3) VTE risk during IBD attacks requiring hospitalization is 6-fold more common than that during attacks not requiring hospitalization. In this consensus, the recommendations for the prevention of VTE are as follows: (1) anticoagulant thromboprophylaxis (using LMWH, heparin, or fondaparinux) should be performed in patients who are hospitalized with a moderate–severe IBD attack and who have no severe bleeding; (2) anticoagulant prophylaxis is recommended for patients with IBD who are hospitalized for a non-IBD cause; (3) thromboprophylaxis by intermittent pneumatic compression is recommended for patients with IBD hospitalized with severe hemorrhage until bleeding is controlled, and anticoagulant thromboprophylaxis is recommended when bleeding is no longer a threat; (4) anticoagulant thromboprophylaxis should be performed on all patients with IBD who are planning to undergo major surgical interventions during hospital stays; (5) anticoagulant thromboprophylaxis is recommended for patients with IBD who have moderate–severe IBD attacks without requiring hospitalization and who have previous VTE history; (6) anticoagulant thromboprophylaxis is not recommended during IBD attacks that do not require hospitalization if there have been no previous VTE attacks or if previous VTE attacks were related to major surgical interventions; (7) anticoagulant thromboprophylaxis is not recommended for patients with IBD younger than 18 years if they have no previous VTE history; and (8) anticoagulant thromboprophylaxis is recommended during hospitalization for pregnant patients with IBD who plan to have a cesarean section. Treatment recommendations may be summarized as follows: (1) patients with IBD who have a VTE attack during clinical remission and who have no other provoking factors should receive life-long anticoagulant treatment; (2) for patients with IBD who have a VTE attack during clinical remission and who have one or more provoking factor(s), anticoagulant treatment should be given for 1 month after the provoking factor has been resolved at a minimum duration of 3 months; and (3) anticoagulant treatment is recommended for patients with IBD who experience a VTE attack during a moderate–severe IBD attack until they are in remission for 3 months (Figure 2).
In conclusion, it is an undeniable reality that venous thrombosis risk is increased in patients with IBD. It appears that arterial thromboembolic disease risk is also increased. In IBD, fibrinolytic activity and natural anticoagulant efficacy are decreased, and the tendency to coagulate is increased due to inflammation, which is the nature of IBD. Moderate–severe IBD attacks, hospitalization, and surgery are the main factors that increase the risk of thrombosis. The IBD-related thrombosis is encountered at earlier ages, recurs more commonly, and is associated with higher morbidity and mortality rates. Although it is not wrong to use mechanical methods, they are not as effective as pharmacological treatment. Therefore, LMWH prophylaxis should be given to all patients with IBD who are hospitalized.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.