
Abstract
Objective:
Antiphospholipid antibodies (aPL Abs) represented an independent factor that was associated with the occurrence and/or progression of nephropathy in patients with antiphospholipid syndrome, but their role in diabetic nephropathy is not elucidated. Therefore, we evaluated the association of aPL Abs with the renal impairment parameters in patients with diabetic nephropathy.
Methods:
Concentrations of analyzed antibodies were measured by enzyme-linked immunosorbent assay.
Results:
Cystatin C and anticardiolipin (aCL) antibodies of the immunoglobulin (Ig) G (r = .349, P = .004) and the IgM isotype (r = .316, P = .009) were in positive correlation. The IgG isotype of the aCL Abs was in positive correlation with creatinine (r = .252, P = .038), urea (r = .241, P = .048), and uric acid (r = .271, P = .025). The concentrations of the IgG isotype of the aCL Abs were significantly different between subgroups of patients with diabetic polyneuropathy and patients without this clinical finding (Mann-Whitney, P = .033).
Conclusion:
This is the first report on positive correlation between aCL Abs and renal impairment parameters. Larger studies are necessary for elucidation whether this association is involved in further progression of the disease.
Keywords
Introduction
The presence of antiphospholipid antibodies (aPL Abs) is associated with the antiphospholipid syndrome (APS). It is an autoimmune disease that is clinically characterized by the presence of thromboses (arterial and/or venous) and/or recurrent miscarriages. 1 –3 Thrombotic manifestations of the APS can occur in almost every organ of the human body. Kidney represents a major target organ for the aPL Abs in patients with APS, and it was reported that aPL Abs represented an independent factor that was associated with the occurrence and/or progression of nephropathy in patients with APS. 4
Diabetic nephropathy is one of the most severe microvascular complications of diabetes mellitus. 5 The alterations in the hemostatic system have been associated with the development of microvascular and macrovascular complications (MVCs) in patients with diabetes mellitus. 6 These alterations include activation of the intrinsic coagulation system, decreased fibrinolytic activity, and endothelial cell dysfunction. 6 It was reported that autoantibodies that target antigens expressed on endothelial cells are involved in the initiation of vascular injury and that aPL Abs target phospholipids (or phospholipid-binding proteins) expressed on cell membranes of different cell types. 7 Previously published papers in regard to the importance of aPL Abs in diabetic nephropathy are contradictory. Therefore, we evaluated the association of aPL Abs (immunoglobulin [Ig] G and IgM isotypes of the anticardiolipin [aCL] and anti-β2glycoprotein I [anti-β2gpI]) with the renal impairment parameters in patients with diabetic nephropathy.
Patients and Methods
Patients
Our study was approved by the local ethical committee, and all participants gave their written informed consent. Study included group of 68 consecutive patients with type 2 diabetic nephropathy (mean ± standard deviation, 62.89 ± 7.28). Male to female ratio was 45:23.
According to the disease duration, patients were divided in the following subgroups. Subgroup 1 included patients with the disease duration ≤10 years and subgroup 2 included patients with disease duration from 11 to 20 years. Patients in the subgroup 3 had disease duration from 21 to 30 years, while subgroup 4 included patients with disease duration ≥ 31 years.
Among analyzed patients, 49 of 68 received insulin, 45 of 68 used oral hypoglycemic therapy, 14 of 68 received beta-blockers, and 28 of 68 patients received angiotensin-converting enzyme inhibitors.
Prior to inclusion in our study, all patients with diabetic nephropathy were examined in order to analyze the presence of potential chronic complications. Therefore, in order to diagnose retinopathy (RP), the presence of positive history of the disease was considered or standard fundus eye examination was performed (detection of microaneurysms, neovascularization, cotton-wool spots, venous dilatation, or hemorrhage). Neurologic examination and interrogation about paresthesia, pain in foot, and so on were used for assessment of clinical neuropathy. Cranial computerized tomography or magnetic resonance was used for the confirmation of cerebrovascular disease. Coronary artery disease was clinically assessed by the presence of angina pectoris or by the presence of abnormal coronary angiogram. Peripheral artery disease was confirmed when peripheral pulse was absent/reduced or intermittent claudication or foot lesion was present. Analyzed patients did not have any of the features of the systemic lupus erythematosus, APS or other autoimmune disease.
Methods
Immunoinhibition test was used for hemoglobin A1c (HbA1c) measurement on AU400 OLYMPUS Chemistry analyzer (commercial reagents of Beckman Coulter, Clinical Diagnostics).
Cholesterol, triglycerides, and high-density lipoprotein (HDL)-cholesterol concentrations were measured by standard enzymatic color tests on AU400 OLYMPUS Chemistry analyzer (commercial reagents of Beckman Coulter, Ireland). Friedwald formula was used for calculation of low-density lipoprotein (LDL) cholesterol concentrations. The intra- and interassay coefficient of variation (CV) for HbA1c, HDL, cholesterol, and triglycerides were less than 1.78%, 5.1%, 1.6%, and 1.1%, respectively (according to the procedure recommended by reagent manufacturer).
The automated latex-enhanced immunoturbidimetric assay and commercial DIAZYME kits (Poway, California) were used for determination of serum cystatin C levels with an intra- and interassay CV less than 5% (according to the procedure recommended by reagent producer).
The kinetic color test (Jaffe method) and commercial Beckman Coulter kits (Galway, Ireland) were used for measurement of serum creatinine levels with an intra- and an interassay CV less than 2.45% (and according to the procedure recommended by reagent manufacturer).
The standardized enzymatic peroxidase-anti-peroxidase (PAP) method with uricase and peroxidase and commercial Beckman Coulter kits (Galway, Ireland) were used for determination of serum uric acid levels with an intra- and interassay CV less than 2.44% and in accordance to the procedure recommended by the manufacturer. Serum urea concentrations were determined on OLYMPUS AU 400 with an intra- and interassay CV less than 3.44%. Proteinuria was determined in 24-hour urine samples on analyzer ADVIA 1800 (commercial kits, Siemens Health Care Diagnostics, Tarrytown, New York). Cutoff values for all above-mentioned parameters were set in accordance with the manufacturer’s recommendations.
Concentrations of analyzed antibodies were measured by enzyme-linked immunosorbent assay using commercial reagents of Orgentec Diagnostika GmbH, Germany, for detection of aCL and aβ2gpI antibodies. Cutoff values for analyzed antibodies were set as manufacturer recommended. The concentration of aCL was measured in MPL or GPL international units (a unit being equivalent to the binding activity of 1 mg of aCL/mL). The intra- and interassay CV for aCL IgG was 5.8% and 3.8%, respectively, while for aCL IgM, it was 5.3% and 3.4%, respectively. Also, the intra- and interassay CV for ab2gpI IgG was 5.0% and 7.9%, respectively, while for ab2gpI IgM was 3.8% and 6.3%, respectively (according to the procedure recommended by the manufacturer).
Statistical Analysis
Descriptive statistics was used to summarize features of analyzed patients. Kolmogorov-Smirnov test was used to study whether analyzed variables followed a normal distribution. The association between the presence of aCL or anti- β2gpI antibodies and the features of patients was examined by χ2 test, Mann-Whitney U test, or t test, when appropriate. The correlation between two quantitative variables was determined with the correlation tests (Spearman, Pearson, when appropriate). Comparison among groups of investigated participants was done by Mann-Whitney U test. In all of the above-mentioned tests, P < .05 was considered statistically significant. Analyses were conducted in SPSS 20 (SPSS Inc, Chicago, Illinois).
Results
Features of patients with diabetic nephropathy are presented in Table 1. Retinopathy was present in 50 patients, while polyneuropathy (PNP) was present in 44 of 58 analyzed patients with available data. Macrovascular complications were present in 27 of 68 patients. Retinopathy and PNP (RP + PNP) were present in 35 patients, while RP and MVC (RP + MVC) were present in 20 patients. Simultaneous presence of RP, PNP, and MVC (RP + PNP + MVC) was observed in 18 patients. Statistical analysis revealed no significant association between the duration of the disease and the presence of RP, PNP, or MVCs. No statistically significant differences in levels of analyzed parameters between subgroup of patients according to the disease duration were found.
Features of the Analyzed Patients With Diabetic Nephropathy.
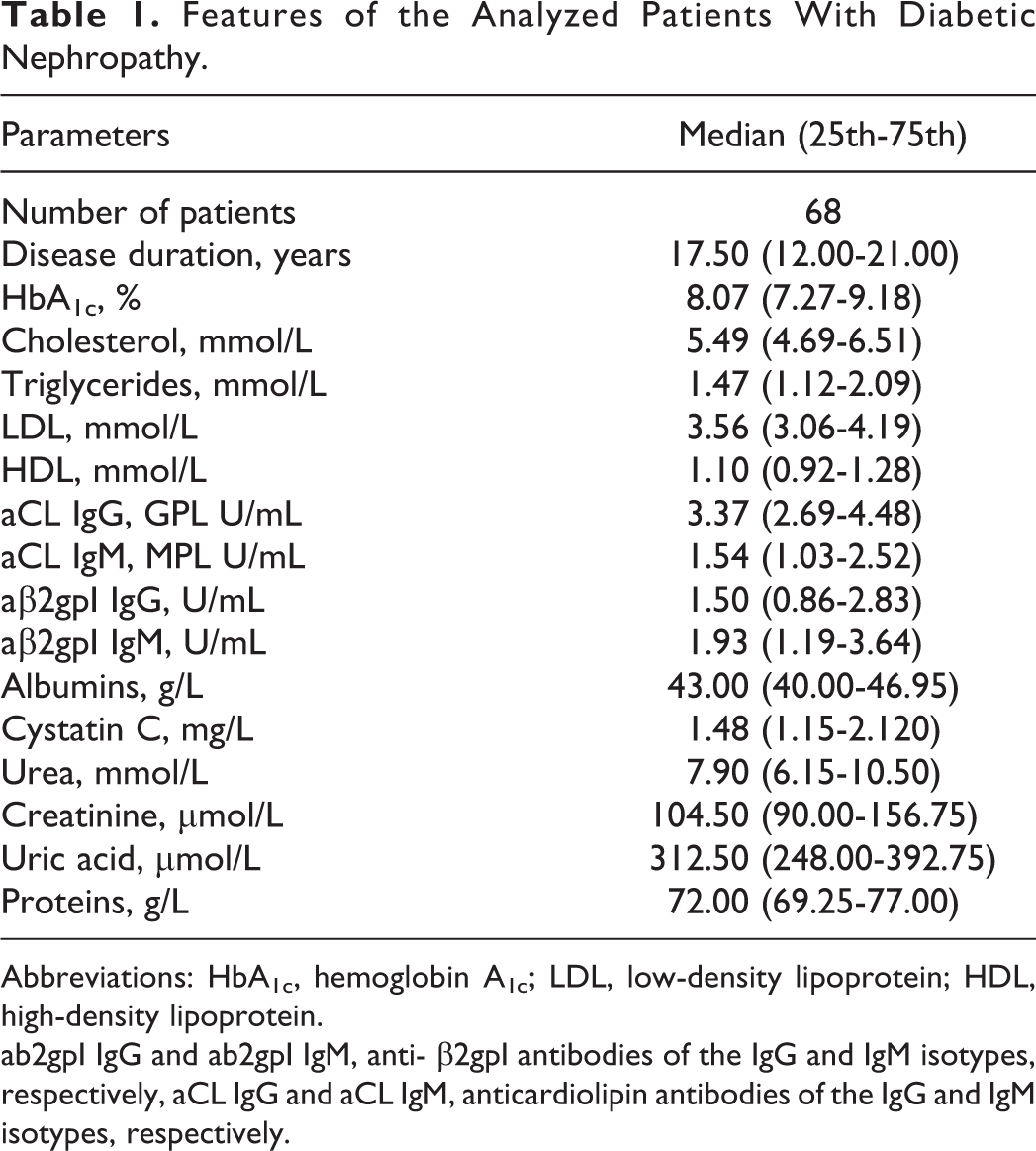
Abbreviations: HbA1c, hemoglobin A1c; LDL, low-density lipoprotein; HDL, high-density lipoprotein.
ab2gpI IgG and ab2gpI IgM, anti- β2gpI antibodies of the IgG and IgM isotypes, respectively, aCL IgG and aCL IgM, anticardiolipin antibodies of the IgG and IgM isotypes, respectively.
In analyzed group of patients with diabetic nephropathy, only 7 (10.29%) had increased aPL Abs titers. One patient had increased IgG aCL Abs titers, four patients had increased IgM aCL, and two patients had increased titers of the IgG ab2gpI Abs.
Although only two female patients had significantly elevated titers of the IgG (χ2 = 4.032, P = .045) and IgM class (χ2 = 4.032, P = .045) of anti-β2gpI antibodies, there was statistically significant difference in comparison to male patients. In addition, two female patients had simultaneous presence of aCL and anti-β2gpI antibodies of the IgM isotype (χ2 = 4.032, P = .045). Neither of the analyzed patients had simultaneous presence of the IgG isotype of aCL and anti-β2gpI antibodies.
The concentrations of the IgG isotype of the aCL Abs were significantly different between subgroups of patients with diabetic PNP and patients without this clinical finding (Mann-Whitney, P = .033). Anticardiolipin Abs of the IgM isotype were in positive correlation with the IgG (r = .245, P = .044) and IgM (r = .547, P = .000) isotypes of the aβ2gpI Abs, while the IgG and IgM isotypes of the aβ2gpI Abs were in positive correlation (r = .440, P = .000).
Figure 1 represents correlation between cystatin C concentrations and the IgG and IgM isotypes of the aCL antibodies. Table 2 represents association between IgG and IgM isotypes of aCL Abs and creatinine, urea, and uric acid.
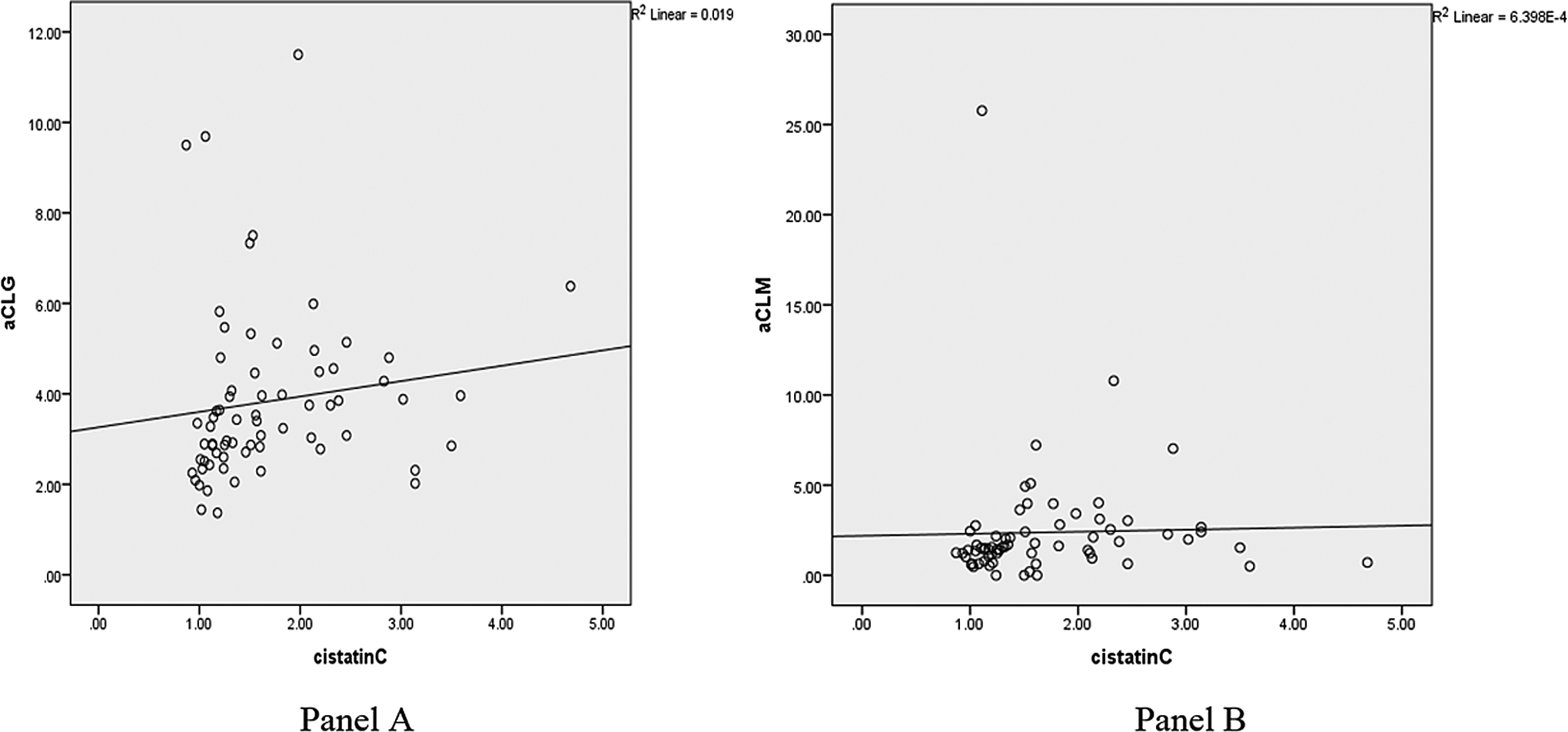
Correlation between cystatin C and anticardiolipin (aCL) antibodies of the immunoglobulin (Ig) G isotype (r = .349, P = .004; panel A) and the IgM isotype (r = .316, P = .009; panel B).
Correlation Between aCL Abs of the IgG and IgM Isotypes and Renal Impairment Parameters.
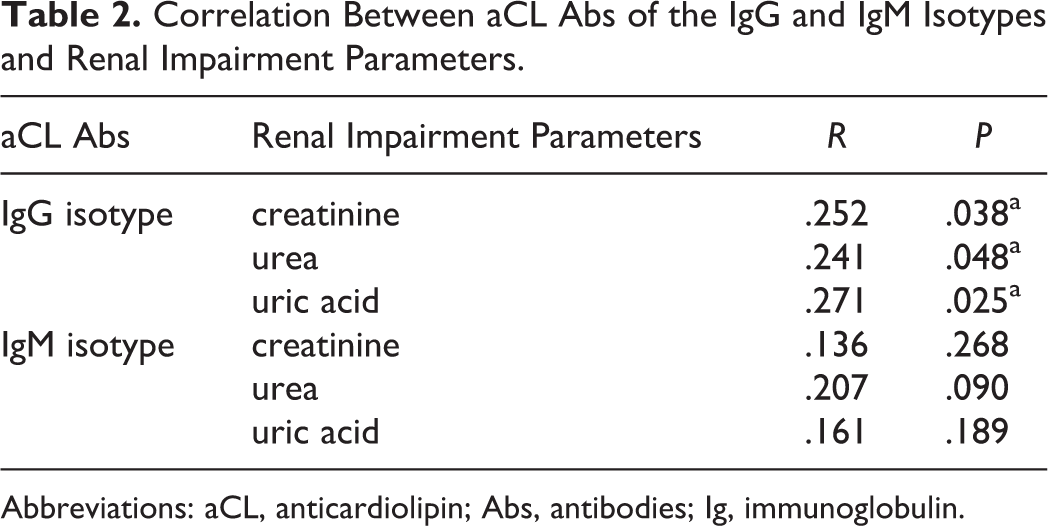
Abbreviations: aCL, anticardiolipin; Abs, antibodies; Ig, immunoglobulin.
Discussion
Diabetic nephropathy is the major culprit of the end-stage renal disease 8 and unfortunately, the earliest clinical sign of diabetic renal disease is microalbuminuria (which represents a sign for therapeutic intervention). The identification of early structural and functional alterations in renal function is very important in diabetic nephropathy. Determination of serum creatinine levels is not very sensitive due to the fact that creatinine levels do not significantly rise until the glomerular filtration rate is reduced (to less than 50% of normal values). 9 Serum cystatin C levels might increase earlier than serum creatinine levels in patients with diabetic nephropathy, 10 and serum cystatin C has advantages over serum creatinine levels for predicting the glomerular filtration rate due to the facts that cystatin C is less affected by age, gender, muscle mass, dietary intake, changes in tubular secretion, and various drugs. 11 In addition to aforementioned advantages, contradictory results were obtained in regard to the fact that cystatin C could be used as a cardiovascular risk marker independent of estimated creatinine clearance. 12 Similarly, there are contradictory reports on association of aCL Abs with coronary artery disease 6 but no reports that analyze potential synergistic role of cystatin C and aCL Abs in regard to the presence of cardiovascular diseases are available. In our study, 39.70% of patients with diabetic nephropathy had macrovascular disease, but no association between cystatin C and/or aPL Abs was found.
Previously reported prevalence of aPL Abs was 9.4% in a group of type 1 diabetic patients and 9.5% in type 2 diabetic patients. 13 Borderline, insignificant association was found for the IgG isotype of aCL antibodies and neuropathy. 14 In our patients with diabetic nephropathy, 10.29% of them had increased titers of aPL Abs. All patients with increased aPL Abs titers had PNP. In addition, we observed that patients with PNP had simultaneous presence of the IgM isotype of aCL and anti-β2gpI antibodies, but this was not statistically significant. Due to the nature of our study and in corroboration with above-mentioned study, 14 it is not elucidated whether aPL Abs were involved in the pathogenesis of endothelial or neurological dysfunctions in diabetic patients, 14 and therefore it is not clear whether aPL Abs were the cause or the result of the disease. 14
No association was found between aPL Abs and gender in a previously published study. 14 Our results are in agreement with a mentioned study considering the fact that we did not find any difference in distribution of aCL antibodies between female and male patients, but we did find significantly elevated levels of both the IgG and IgM isotypes of anti-β2gpI antibodies only in female patients.
Early detection of abnormalities in renal function may provide information in which way to influence the course of diabetic renal disease. 15 In this sense, determination of aPL Abs would be beneficial. This is the first report on positive correlation between aCL Abs and renal impairment parameters. Larger studies are necessary for elucidation whether this association is involved in further progression of the disease.
Footnotes
Ethical Approval
Compliance with Ethical Standards: All procedures performed in our study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Authors’ Note
Mirjana Bećarević contributed to the design of the study, data analysis, and interpretation of data. Velibor Čabarkapa contributed to the acquisition of data and interpretation of the data. Mirjana Đerić and Svetlana Ignjatović critically revised the article for important intellectual content. All authors have read and approved final version of the article to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The present work was supported by the Ministry of Science and Education of the Republic of Serbia on the basis of contract No175036. None of the authors had the conflicting financial interest.