
Abstract
Thromboelastography (TEG) has long been available for routine monitoring of perisurgical and postpartum hemostasis, especially at point of care. The purpose of this study is to retrospectively compare TEG parameters to concomitant standard clotting test results in an unselected cohort of patients with Gaucher disease to ascertain whether TEG values are specific and sensitive enough to substitute for classic coagulation tests for decision making. This remains a cogent concern because of high incidence of thrombocytopenia in patients with Gaucher disease. Thromboelastography values were compared to concomitant platelet counts, partial thromboplastin time, international normalization ratio, and plasma fibrinogen. Demographic characteristics were collected from patients’ files. There were 22 patients with Gaucher disease (2 children; 12.5%) for whom there were 24 TEG results at the same time as classic coagulation test results and 30% performed platelet function tests. The current study shows linear and/or monotonic relationships between platelet counts and several TEG values that were significant over a range of platelet counts including severe thrombocytopenia. The fibrinogen component, correlating only with the rate of clot lysis, played a lesser role. Based on these preliminary results albeit in a small cohort with only 1 case of hemorrhage, there is putative support for the intention to treat patients with Gaucher disease based on TEG results using the same TEG protocol as for other patients undergoing comparable procedures in our institution.
Keywords
Introduction
Thromboelastography (TEG) has been available for monitoring perisurgical hemostasis and as a surrogate for transfusion management in major surgery, trauma, and hemophilia. The goal of TEG, a more time-sensitive and dynamic assay than classic coagulation profiles, is evaluation at the point of care. 1,2 The computerized Thrombelastograph Hemostasis System automatically records kinetic changes in whole blood, plasma, or platelet-rich plasma as the sample clots, retracts, and/or lyses. 3 The resultant coagulation profile is a measure of the kinetics of clot formation and dissolution and clot quality, potentially averting some complications resulting from indiscriminate/premature administration of blood products while awaiting classic coagulation results. 4
The purpose of this study is to compare TEG parameters to concomitant standard clotting results 5 in an unselected cohort of patients with Gaucher disease to ascertain whether TEG is specific and sensitive enough to substitute 6 for decision making.
The choice of Gaucher disease is predicated on the existence of chronic thrombocytopenia, sometimes despite long-term disease-specific enzyme replacement therapy (ERT), 7 which is especially effective in correcting anemia and thrombocytopenia and hepatosplenomegaly of Gaucher disease. 8 Heretofore, it had been recommended that, in addition to routine coagulation profiles, platelet function tests 9 are required 10 –12 in Gaucher disease presurgery and/or delivery. 13 Second, there are coagulopathies that impact tendency to bleed even in nonthrombocytopenic patients who are partly responsive to ERT. 14 Finally, there are coagulation factor deficiencies that are relatively more prevalent among Ashkenazi Jews who have a predilection for the nonneuronopathic form of Gaucher disease. 8
Admittedly, the full range of abnormal adhesion–aggression abnormalities and of coagulation factor deficiencies in Gaucher disease, 15 whether or not impacted by ERT, is multifactorial, including features not Gaucher induced as well. In a survey of Egyptian children with Gaucher disease, 5 with ERT and 5 newly diagnosed, factor deficiencies II, V, VII, VIII, X, XI, and XII were noted in 20% to 60% and low levels of serum fibrinogen in the untreated children 15 ; factor XI deficiency is prevalent among Ashkenazi Jews. 16 Therefore, the option of TEG as a more universal surrogate marker for bleeding tendency would be attractive.
Materials and Methods
Institutional Review Board (Helsinki Committee) approval was received for this study. This is a retrospective study of archival material plus results of routine laboratory tests. Whole blood was collected prior to surgery in tubes with sodium citrate and kaolin-activated TEG was assessed. Because of concern about reproducibility, all tests were performed within 4 hours of blood sampling.
For each patient prior to surgery, the following TEG parameters (as described by the TEG manual, see Figure 1) were collected:
R = reaction time (in minutes) of latency from time blood is placed in TEG analyzer until initial fibrin formation (the enzymatic aspect of coagulation);
K = speed (in minutes) to reach a certain level of clot strength (kinetic feature)
angle (α) = rapidity of fibrin build-up and cross-linking (represents fibrinogen level);
CI = coagulation index derived from the R, K, MA, and angle of native or kaolin/celite-activated whole blood tracings; normal values lie between [−3.0] and 3.0 with CI > 3.0 indicative of hypercoagulability, CI < −3.0 indicate hypocoagulability;
MA = maximum amplitude, a direct function of the maximum dynamic properties of fibrin and platelet bonding via GPIIb/IIIa and ultimate strength of the fibrin clot (represents platelet function/aggregation);
A = amplitude (in mm); width of tracing at last time point equal to MA until MA is determined (represents clot strength or elasticity);
G = shear elastic modulus strength (as dyne/cm2 divided by 1000) is derived from A and its calculation stops when MA is reached;
LY30 = percent clot lysis; that is, rate of amplitude reduction 30 minutes after MA (based on reduction of area under the TEG tracing from time MA is measured until 30 minutes after the MA);
EPL = estimated percent lysis at 30 minutes after MA and is continually updated until 30 minutes after MA is reached when EPL equals LY30; and
PMA = projected MA, an estimator of MA; that is, whether the MA value will achieve at least the lower limit of the normal value for samples treated with kaolin/celite; described as 0 = likely to achieve normal limit and 1= unlikely; affords detection of platelet dysfunction before MA is available
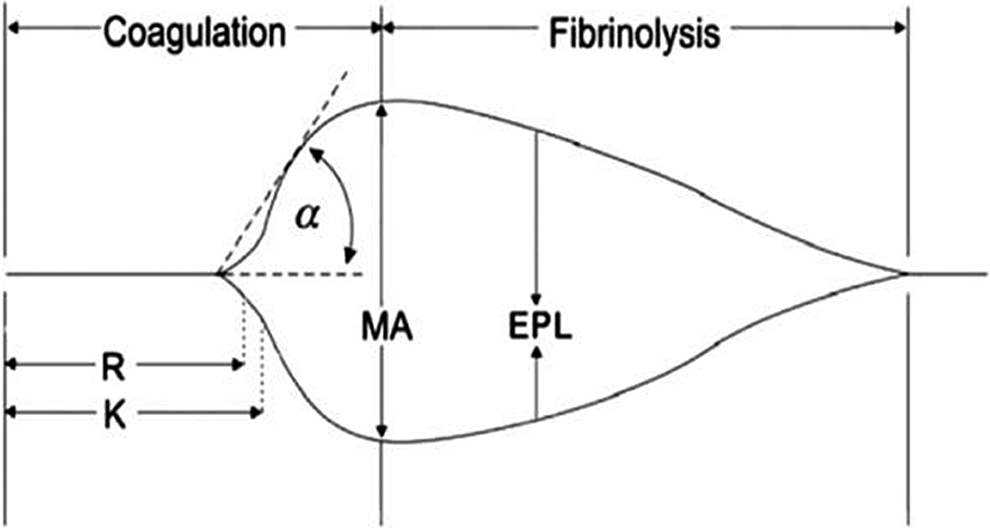
Classic normal thromboelastography (TEG) graph. The following TEG parameters are recorded from standard tracings: split point (SP), reaction time (R, minutes), coagulation time (K, minutes), angle (α, °), maximum amplitude (MA, mm), clot strength (G, dynes/scm), and percentage lysis (LY30, Lysis at 30 minutes, %). The coagulation index (CI) is a linear combination of R, K, angle, and MA that is believed to represent the overall coagulation status (TEG Manual, 2008).
In our institution, TEG is performed on whole blood samples. Once the CI value is obtained, the TEG analysis is reset for MA analysis.
Platelet function testing was performed at the National Hemophilia Center as previously described. 13,17 In brief, aggregations were performed on a 4-channel optical aggregometer (aggram, Helena laboratories, Beaumont, Texas). Epinephrine (5 mg/mL), ADP (1.0 mmol/L), collagen (1.0 mg/mL, final concentration), and ristocetin (0.5 and 1.5 mg/mL) were used as agonists. Normal platelet-rich plasma, obtained from healthy individuals, was used as a parallel control in each experiment. Aggregation was considered abnormal if maximum aggregation was <70% of control. 13 Results were expressed as percentage of aggregation relative to control. Platelet function was also measured in whole citrated blood under shear force and flow conditions, using the cone and platelet analyzer (CPA-Impact R, Diamed, Cresier, Switzerland). The CPA procedure involved placing 200 µL samples of citrated whole blood in polystyrene 4-well plates (Nunc; Roskilde, Denmark) precoated with 1% bovine serum albumin to minimize cell adhesion. Blood was subjected to shear stress (1800 L/s) for 2 minutes using a rotating Teflon cone. The plates were washed with phosphate-buffered saline, stained with May-Grunwald stain, and analyzed using an image analysis system (Impact-R, Sresier, Switzerland). Two quantifiable parameters of platelet function were evaluated: platelet adhesion, defined as percentage of total area covered by platelets (surface coverage; SC), and platelet aggregation, defined as the average size (AS) of bound objects (either aggregates or single platelets). The normal adult values in our laboratory were derived from 98 healthy adult controls and were SC = 11.72% ± 3.1%, and AS = 44.93 ± 16.4 µM2. Abnormal SC or AS values were defined if results were <70% expected control values.
In addition, the following standard coagulation 10,13 profile assessments were collected at the presurgical assessment and were performed in the routine clinical laboratories: platelet counts, partial thromboplastin time (PTT; reference range 60-70 seconds), international normalization ratio (INR; reference range: 0.8-1.1), and plasma fibrinogen (reference range: 1.5-4.0 g/L) concentration. Demographic characteristics were culled from records at the Gaucher Clinic. Data about perioperative and peripartum bleeding were collected from patients’ files.
Statistical Analyses
Descriptive statistics were used for patient characteristics and test results. For comparison of independent variables, the Levene test for equality of variances and t test were employed. Both the Pearson product moment correlation coefficient and Spearman correlation coefficient were applied to ascertain if there were any general monotonic trends when comparing the traditional coagulation values with those derived from TEG.
Results
The demographic characteristics and results of the various features of the TEG test are presented in Table 1. Although all patients had been recommended to undergo platelet function testing, only 9 (30%) patients actually had done so with the explanation of inconvenience. However, among this cohort, 3 patients had abnormal aggregation and adhesion; 2 patients had factor XI deficiency (1 was the woman who bled); 1 patient had a mild aggregation defect only; 1 patient had abnormal CPA only; and 2 patients had no abnormalities.
Demographic Characteristics of 24 Results of Coagulation Testing Including TEG Subanalyses.
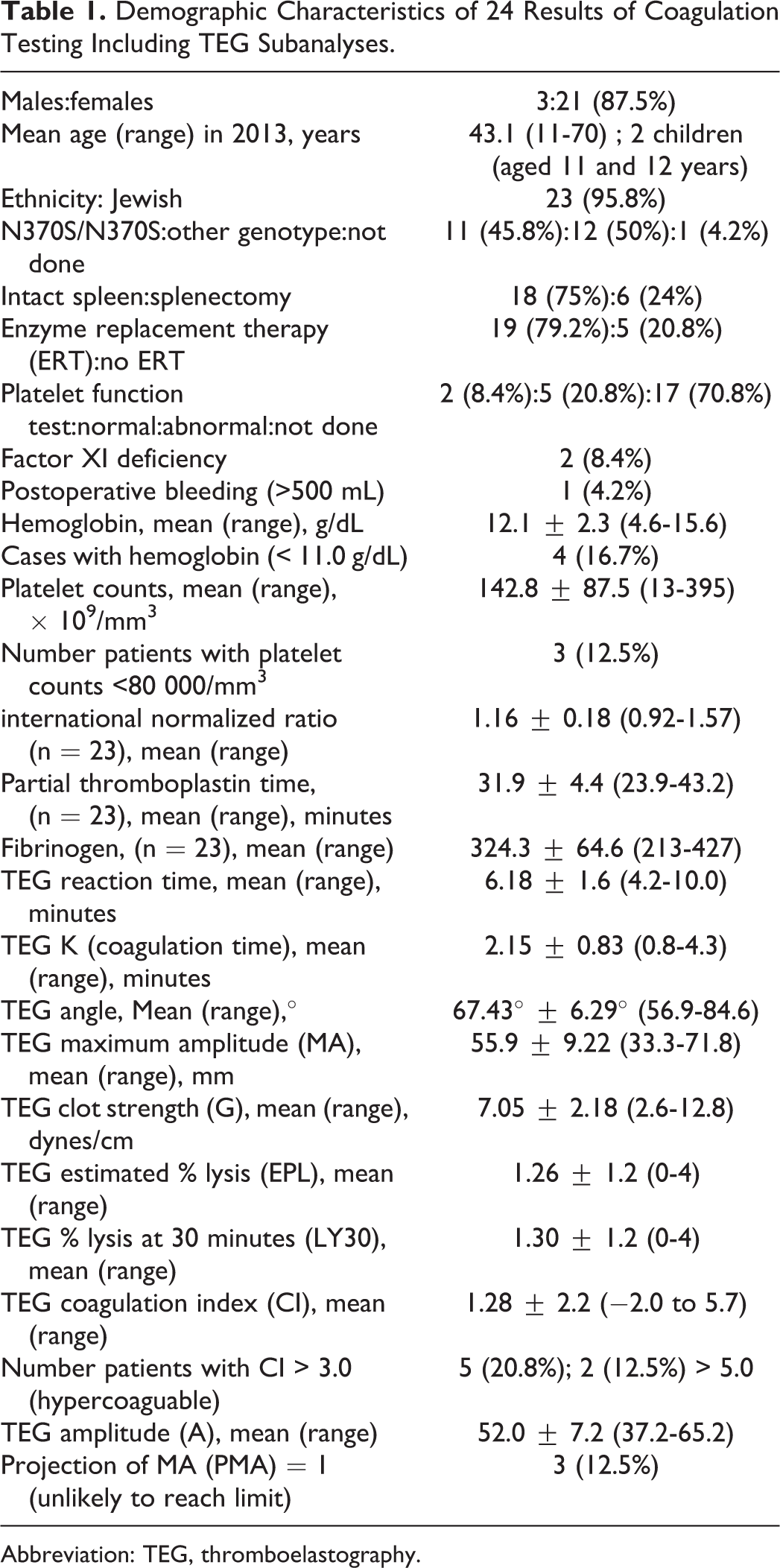
Abbreviation: TEG, thromboelastography.
There was only 1 case of hemorrhage (defined as >500 cm3), and this was postpartum in an untreated patient with a history of a previous postpartum hemorrhage and factor XI (56%) deficiency but with normal TEG values; hemoglobin was 11.7 g/dL, platelet counts 94 000/mm3 (with normal platelet function test), PTT 34.1 seconds, and INR 1.03.
Other than the above-mentioned outliers, most patients showed values within normal ranges for most parameters except 3 female patients (aged 11, 33, and 48 years) who were the only 3 with a PMA = 1 (unlikely to reach lower limit of normal) and in addition were among the patients with low platelet counts (44, 13, and 96 × 109/mm3, respectively), with low MA (34.4, 42.3, and 56.8 mm), and among the 5 patients with abnormally high CI values (5.7, 3.8, and 5.2, respectively); the child and older (splenectomized) patients were receiving ERT.
There was no correlation between abnormal classical platelet function tests and clinical bleeding. None of the 5 patients who performed the platelet function tests with some mildly abnormal results had abnormal MA values (range: 56.7-58.9 mm).
There were no significant differences in the mean results of the TEG features when comparing (Levene’s t test for equality of means) patients homozygous for the N370S mutation and the other patients (data not shown) or between patients receiving ERT relative to the untreated patients (data not shown); however, comparing patients with splenectomy to those with an intact spleen, there was a significant difference (P = .037) for reaction time (R).
Table 2 presents those tests for which there was a statistically significant correlation when applying the Pearson r test and/or the Spearman ρ tests. There were no significant correlations with CI although there were 5 tests with values >3.0, indicating hypercoagulability.
Results of Comparison of Correlation Coefficients of Classical Coagulation Test Results and TEG Values for Significance (2-tailed).
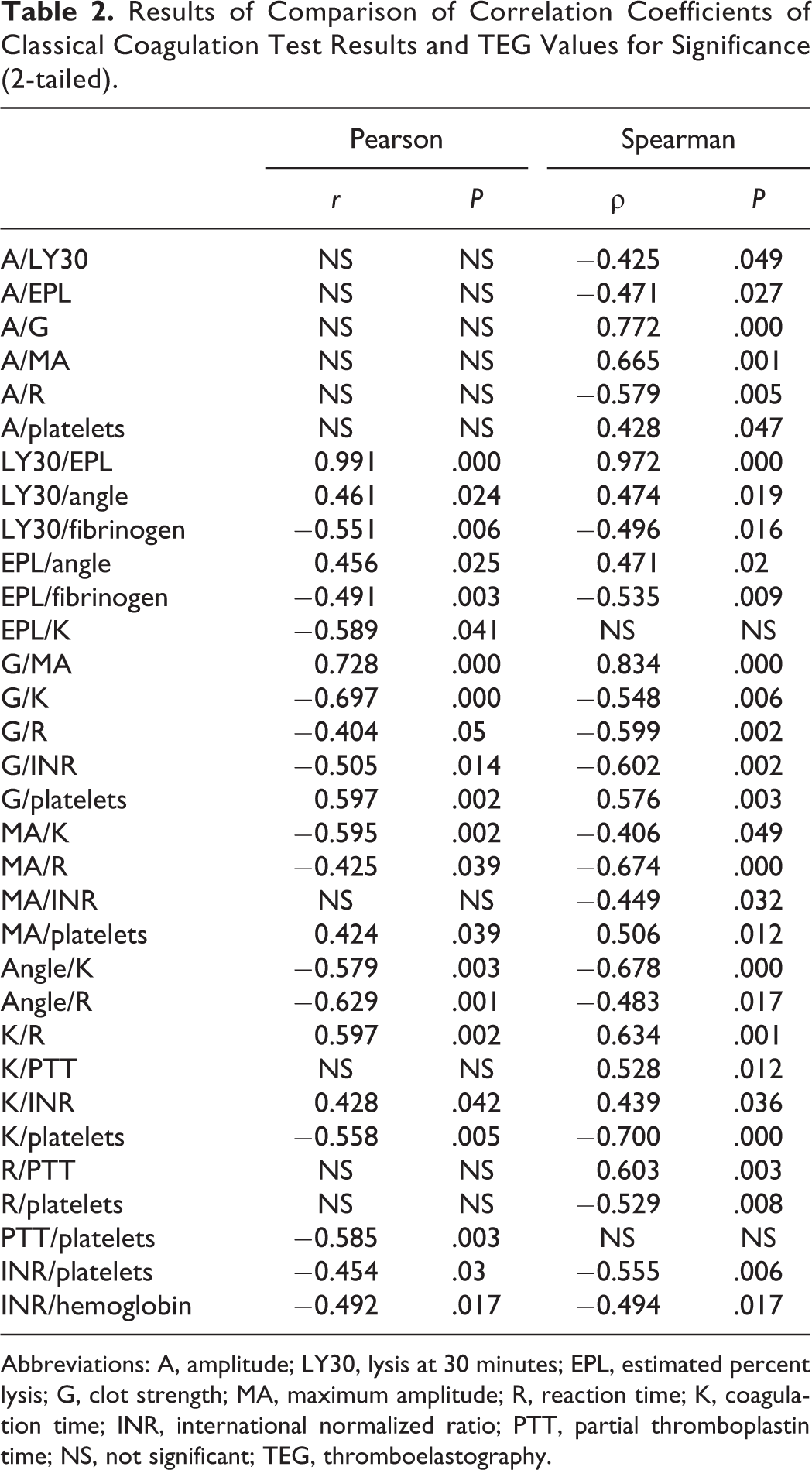
Abbreviations: A, amplitude; LY30, lysis at 30 minutes; EPL, estimated percent lysis; G, clot strength; MA, maximum amplitude; R, reaction time; K, coagulation time; INR, international normalized ratio; PTT, partial thromboplastin time; NS, not significant; TEG, thromboelastography.
Table 2 shows that in most cases (19 of 32 comparisons; 59.4%), the correlation among TEG values and between TEG values and the traditional variables was both linear (based on Pearson) and monotonic (based on Spearman); in the majority the relationship was indirect. However, all correlations with amplitude (A) and some with maximum amplitude (MA), reaction time (R), and speed of clot strength (K), were monotonic only. Among the latter were correlations with traditional coagulation tests such as INR, PTT, and platelet counts. There were only 2 comparisons (EPL/K and PTT/platelet counts) that were linear only.
Discussion
This survey is the first to provide comparisons of TEG results among patients with Gaucher disease with more traditional values of coagulation and risk of bleeding. In that the cohort is far from homogeneous in terms of age, genotype, exposure to disease-specific therapy, platelet counts, platelet function, and type of surgery, the results highlight the fact that there was only a single case of bleeding and this may not necessarily be attributed to Gaucher disease. However, the objective of this study was to underscore the utility of point-of-care use of TEG in patients with Gaucher disease comparable to its utility in otherwise healthy persons. Various features of the TEG satisfactorily described findings of the traditional tests which take longer to become available.
The rationale for the current study was the concern about unexpected bleeding during surgeries among patients with Gaucher disease. Among the established reasons for bleeding are thrombocytopenia (which may occur after long-standing splenectomy and among poor responders to disease-specific ERT) as well as because of poor platelet function and/or coagulation deficiencies.
Neither thrombocytopenia nor long-term disease-specific ERT is predictive of postpartum hemorrhaging in women with varying severity of signs of Gaucher disease. 13 Poor platelet function, that is, impaired platelet aggregation (<third percentile normal aggregate size values) was better correlated with postpartum hemorrhage in Gaucher disease. 13 Clinically significant factor deficiencies are encountered less frequently in adults with Gaucher disease but may be pervasive. 15,16 Importantly, however, with ERT, there is partial correction of some coagulopathies 14 so that thrombocytopenia may be the major risk factor for bleeding in Gaucher disease.
Recent experimental work in dogs 18 has underscored the value of TEG at point of care in identifying risk of bleeding in thrombocytopenia. Specifically, platelets have been shown to affect the strength of clot formation in TEG, particularly the MA value, as well as all other phases of coagulation. 19 Thus, should TEG implicate thrombocytopenia, this would have practical ramifications. The current study shows linear and/or monotonic relationships between platelet counts and the TEG values A, G, MA, K, and R. These relationships were significant over a range of platelet counts including severe thrombocytopenia. Moreover, it appears that the fibrinogen component, with correlation only with rate of lysis of the clot, played a less central role in risk of bleeding in these patients. Similarly, there were only 2 women with coagulation (factor XI) deficiency so that PTT was seen to describe a linear relationship with platelet counts based on the larger majority of normal range values. On the other hand, since the 1 patient to bleed was a woman with near-normal platelet counts and (marginal) factor XI deficiency, the hemorrhage may be attributable to the factor deficiency, 20 and this was not evident on TEG evaluation.
It has been the experience of an international collaborative effort that TEG and comparable technologies are not sufficiently performed in a uniform manner. 21 Bearing this in mind, it would appear that for a rapid and holistic approach to risk of bleeding in patients with Gaucher disease who may be thrombocytopenic, TEG may be a good option presurgery for management decision making regarding need for exogenous blood products. It has been the policy for the past 5 years at our Department of Anesthesiology to test for TEG presurgery and predelivery so that they have garnered experience in more than 5000 patients. In the majority, management decisions were based solely on TEG results including at delivery. Nonetheless, this exploration with a very small sample size of patients with Gaucher disease, who do not all have thrombocytopenia, and with only 1 instance of bleeding and that in a patient with a comparable previous postpartum bleed, is insufficient to draw definitive conclusions, nonetheless, the intention to treat would have been based on TEG results.
Footnotes
Author’s Note
Alexander Ioscovich and Dmitri Fadeev contributed equally to the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.