
Abstract
We studied the level of lipid peroxide, nitric oxide (NO), trace elements (TEs), and microparticles (MPs) in Gaucher disease (GD) before and after 1 year of enzyme replacement therapy (ERT). A total of 15 children with GD and 15 healthy controls were enrolled in this study. Serum level of lipid peroxide, NO, and TEs was determined. The MPs were detected by flow cytometry. The level of lipid peroxide was significantly higher in the patients than in the controls even after ERT. Although NO level was normalized in the patients after ERT, zinc and copper were still lower in the patients after ERT. The percentages of various MPs were significantly higher in the patients than in the controls both before and after ERT. There were positive correlations between chitotriosidase and both lipid peroxide and total MPs.
Conclusion:
The GD is associated with alteration in oxidant and antioxidant status and high level of circulating MPs.
Introduction
Gaucher disease (GD) is an inborn error of glycosphingolipids metabolism due to lysosomal β-glucosidase deficiency. 1 The deficiency of the enzyme leads to progressive accumulation of glucosylceramide and other glycosphingolipid and subsequent multiorgans dysfunction. 2 All forms of the disease involve some degree of hepatosplenomegly, anemia, thrombocytopenia, bone complications, and abnormal energetic metabolism. 3 Based on the neurological signs, 3 clinical phenotypes are recognized: type 1, the classic form, affects 95% of the patients and is usually defined by the absence of central nervous system impairment; types 2 and 3 are rare and severe due to neurological involvement. 4 It is a relatively rare disease with an overall incidence of approximately 1:40 000 individuals. 5
Since the 1990s, treatment of GD had included enzyme replacement therapy (ERT) using mannose-terminated recombinant human glucocerebrosidase imiglucerase. The ERT has been shown to ameliorate systemic involvement in type 1 GD and to enhance the quality of life. 6,7 Ceramide and glycosphingolipids are involved in signal transduction pathways that cause reactive oxygen species (ROS) generation. Therefore, the imbalance in glycosphingolipids pathway characterizing GD might contribute to increase in the basal ROS levels in GD cells. 2
Trace elements (TEs) are essential and very limited quantity in human. 8 The essential TEs zinc (Zn), copper (Cu), and selenium (Se) act as cofactors of key antioxidant enzymes, namely, superoxide dismutase, catalase, and glutathione peroxidase, contributing to both catalytic activity and spatial conformation. 9 The Zn may protect against cytokine-mediated activation of oxidative stress-sensitive transcription factors, upregulation of inflammatory cytokines, and endothelial cell dysfunction. 10
Cell-derived microparticles (MPs) are microvesicles of size <1.0 μm, released from parent cells during cell activation or apoptosis. Most MPs are highly procoagulant, expressing annexin V binding sites and are capable of interacting with other cells to participate in various physiologic and pathologic processes, especially thrombosis, inflammation, 11,12 and angiogenesis. 13 Recently, MPs are receiving increasing attention as sensitive biomarkers of prothrombotic and inflammatory states. 14,15 Oxidative stress is one of the risk factors involved in an increase in MPs formation. 16 Oxidative stress is also generated by MPs. 17 Little is known about the level of oxidative stress, TEs, and MPs in GD.
The aim of this study is to assess the levels of MPs, lipid peroxide, nitric oxide (NO), and TEs (Zn, Cu, and Se) in patients with Gaucher disease.
Patients and Methods
Patients
All aspects of this study were approved by the University of Assiut Institutional Review Board. The patients were enrolled in this prospective study after obtaining the informed consent from the parents. A total of 15 patients meeting the diagnostic criteria of type 1 GD 18 were recruited consecutively at the Pediatric Clinical Hematology Unit, Children Hospital of Assiut University, from June 2009 to December 2011. In all patients, diagnosis was made by bone marrow aspirate and biopsy and enzyme assay of β-glucocerebrosidase and chitotriosidase. Patients received ERT from Genzyme Company through the Project Hope after acceptance of both Gaucher committee in Cairo and Genzyme Gaucher committee group. Patients started ERT (Cerezyme) on 60 IU/kg every 2 weeks. A total of 15 healthy children of matchable age and sex selected from patients, healthy relatives, and friends were taken as controls after obtaining consent from their parents.
Inclusion Criteria
Patients with Gaucher disease not started ERT.
Clinically diagnosed patients with type 1 Gaucher disease
Exclusion Criteria
Patients with Gaucher disease on ERT.
Patients with type 2 or 3 Gaucher disease
Patients with other metabolic diseases such as Niemann Pick disease
Age > 16 years
Patients with infection or other inflammatory conditions
Methods
All patients and controls were subjected to history and physical examination in addition to the following investigations; full blood picture (Celltac E automated hematology analyzer; ihon Kohden Corporation, Tokyo, Japan), abdominal sonar, determination of serum level of Zn, Cu, Se, lipid peroxide, and NO, and flow cytometric detection of MPs. All the above investigations were done before starting ERT and after 1 year of ERT.
Determination of Serum Level of Zn, Cu, Se, Lipid Peroxide, and NO
Venous blood samples of 3 mL were collected aseptically from all the patients via venepuncture in a sterile collecting tube. These samples were centrifuged at 500g for 15 minutes. The separated sera were collected and stored at −70°C.
The levels of Zn, Cu, and Se were determined by atomic absorption/flam emission spectrophotometer (Shimadzu-model AA-630-02; Shimadzu Atomic absorption/Flame Emission Spectrophotometer, AA-630-02, SHIMADZU CORPORATION. Kyoto, Japan) GBC 906 AA. The wave length used for the measurement of these elements was 213.9, 324.7, and 196.0 nm, respectively. The lamp current used was 10, 10, and 20 mA, respectively. The results were obtained from standard curves and expressed in μg/dL. 9
Serum lipid peroxide was determined by chemical method according to the method described by Buege and Aust. 19 The NO was determined according to the method described by Van Bezooijen et al. 20
Microparticles Isolation and Characterization
Blood samples were collected into a 5-mL tube containing 3.2% citrate. In order to isolate the MPs, the cells were removed by centrifugation for 20 minutes at 1550g at 20°C within 15 minutes after the collection. Then 250 µL of plasma was centrifuged for 30 minutes at 18 800g at 20°C. After centrifugation, the supernatant was removed, and the pellet was resuspended in phosphate-buffered saline (PBS) and centrifuged for 30 minutes at 18 800g at 20°C. The supernatant was removed again, and the MPs pellet was resuspended in PBS. 21
Flow cytometric analysis was used to quantify and characterize MPs. The MP samples of 5 µL were diluted in 35 µL PBS containing 2.5 mmol/L CaCl2. The samples were then incubated for 20 minutes at room temperature in the dark with 5 µL of fluoroisothiocyanate-conjugated annexin V (IQ products, the Netherland), 5 μL of phycoerythrin conjugated, and 5 μL peridinium-chlorophyll protein cell-specific anti-human monoclonal antibody in each tube according to the following panel.
Annexin V/CD146 (Beckman coulter, France)/CD45 (Becton Dickinson [BD] Biosciences, San Jose, California).
Annexin V/CD14 (Beckman coulter)/CD33 (BD Biosciences).
Annexin V/CD235a (BD Biosciences)/CD41 (EXBIO praha, Nad safinou, Vestec, Czech Republic).
Annexin V/CD61 (BD Biosciences)/CD62P (BD Biosciences)
After incubation, PBS/calcium buffer were added, and the samples were analyzed on FACSCaliber flow cytometry with Cell Quest software (BD Biosciences). A total of 50 000 events were analyzed. Anti-human IgG was used as an isotype-matched negative control for each sample. 21,22
The MPs were identified on the basis of their forward scatter compared with that of calibrate reference beads of 1.0 µm to calibrate the size range of MPs (latex beads, amine-modified polystyrene, fluorescent red aqueous suspension, 1.0-μm mean particle size; Sigma-Aldrich Chemie Gmbh, Munich, Germany) and positivity for annexin V. The MPs express phosphatidylserine that is detected by annexin V labeling. 23 Total MPs were that events, which had the size lower than that of the reference beads and express annexin V (Figure 1). Total MPs were reported as a percentage of the total events. The MP subpopulation as platelet, endothelial, and other were expressed as percentages of total MPs.
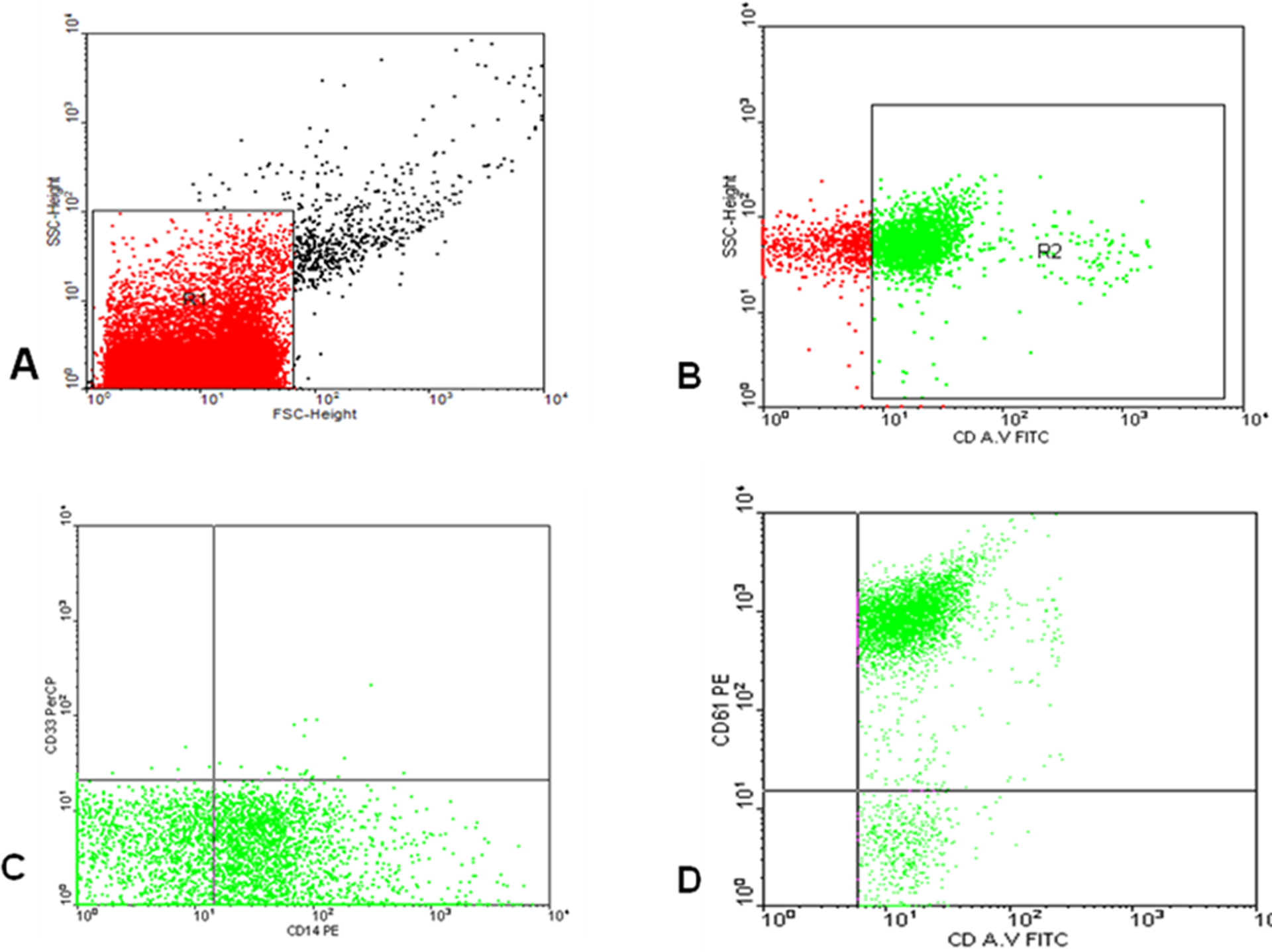
Flow cytometric analysis of microparticles. A representative set of scattergrams of a sample from patient with Gaucher disease showing microparticles (MPs) and MP subpopulations. Forward and side scatter histograms were used to define the MPs (R1) according to the size of the reference calibrate bead (A). Events defined as MPs were then selected for their annexin V binding, determined by the positivity for annexin V (R2; B). Then annexin V-positive MPs (total MPs) were further examined for the expression of cell-specific antibodies as CD61, CD14, and CD33 (C and D) compared with the negative isotype control (not shown).
Statistical Methods
Data analysis was done with SPSS, version 16. Data were expressed as the mean ± standard error of mean. Because of the small sample size and a propensity for outliers in some of the variables, all inferential analyses used 2-sided nonparametric rank-based tests. Statistical comparison using Mann-Whitney and Wilcoxon was applied to compare values of the studied groups. Spearman correlation coefficient was used to examine the correlations among different studied parameters. A statistically significant result was considered when P value ≤.05.
Results
Some baseline characteristics of the patients and controls are represented in Table 1. Before starting ERT, the current study revealed a significant increase in the mean serum level of lipid peroxide and NO in patients with GD thanin the controls. There was a significant decrease in the mean serum levels of Zn and Cu in the patients than in the controls. The mean serum level of Se was decreased in the patients than in the controls, but the difference was not statistically significant (Figure 2).
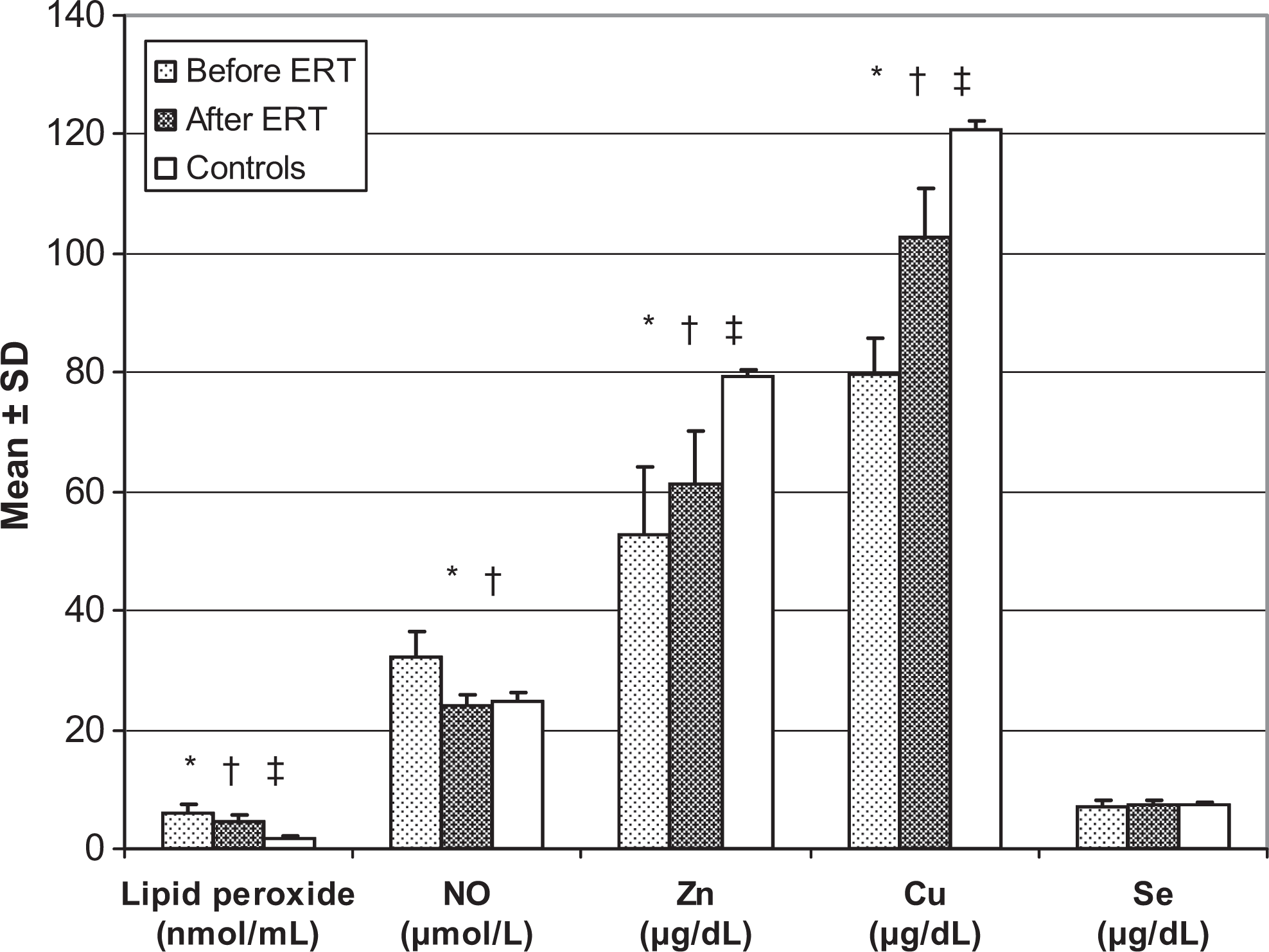
Lipid peroxide, NO, and some trace elements in patients before and after 1 year of ERT and controls. Values are represented as mean ± SEM. *Significant difference (P < .05) between patients before ERT and controls (Mann-Whitney U test). †Significant difference (P < .05) between patients before ERT and after ERT (Wilcoxon test). ‡Significant difference (P < .05) between patients after ERT and controls (Mann-Whitney U test). ERT indicates enzyme replacement therapy; NO, nitric oxide; Zn, zinc; Cu, copper; Se, selenium; SEM, standard error of mean.
Baseline Characteristics of Patients With Gaucher Disease Before and After 1 Year of Enzyme Replacement Therapy and Controls.a
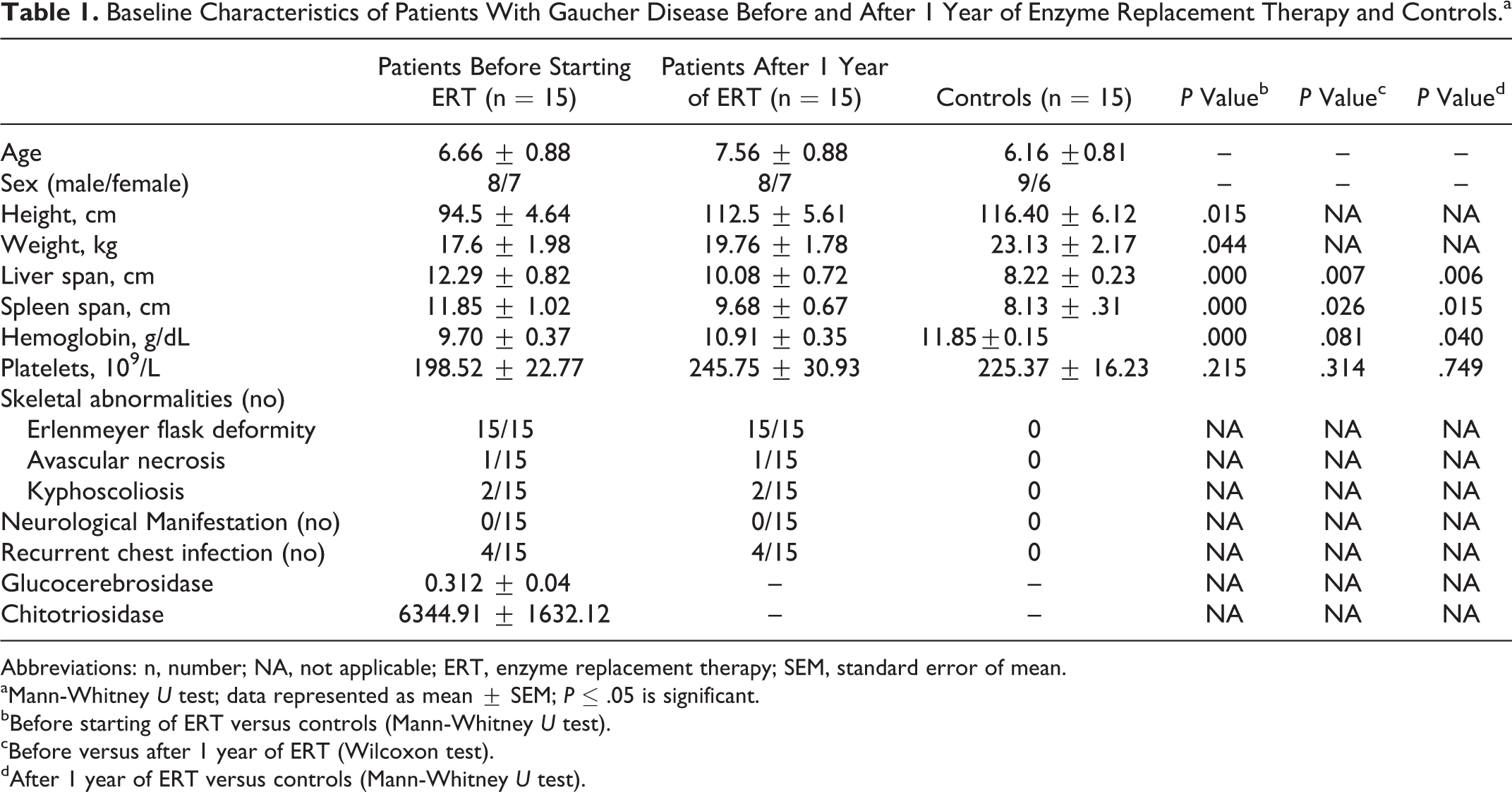
Abbreviations: n, number; NA, not applicable; ERT, enzyme replacement therapy; SEM, standard error of mean.
aMann-Whitney U test; data represented as mean ± SEM; P ≤ .05 is significant.
bBefore starting of ERT versus controls (Mann-Whitney U test).
cBefore versus after 1 year of ERT (Wilcoxon test).
dAfter 1 year of ERT versus controls (Mann-Whitney U test).
After 1 year of ERT, the mean serum level of lipid peroxide and NO was significantly decreased than that detected before starting of ERT, while the mean serum level of Zn and Cu was significantly increased. The mean serum level of Se was increased in the patients after 1 year of ERT than that detected before starting ERT, but the difference was not statistically significant (Figure 2).
When comparing patients with GD after 1 year of ERT with the controls, the mean serum level of lipid peroxide was still significantly higher in the patients than in the controls. In addition, the mean serum levels of Zn and Cu were still significantly lower in the patients than in the controls. The NO and Se showed no significant difference between the patients and the controls (Figure 2).
Before starting ERT, total MPs were significantly increased in patients with GD than in the controls. Platelet MPs (CD41+ CD235a−), activated platelet MPs (CD61+ CD62P+), and endothelial MPs (CD146+ CD45−) were significantly higher in the patients than in the controls. The MPs of other cellular origins as leukocytes (CD45+), granulocytes (CD33+, CD14−), monocytes (CD33+, CD14+), and erythrocyte (CD41− CD235a+) were not significantly different between the patients and the controls (Table 2).
Circulating Microparticles in Patients With Gaucher Disease Before and After 1 Year of Enzyme Replacement Therapy and Controls.a
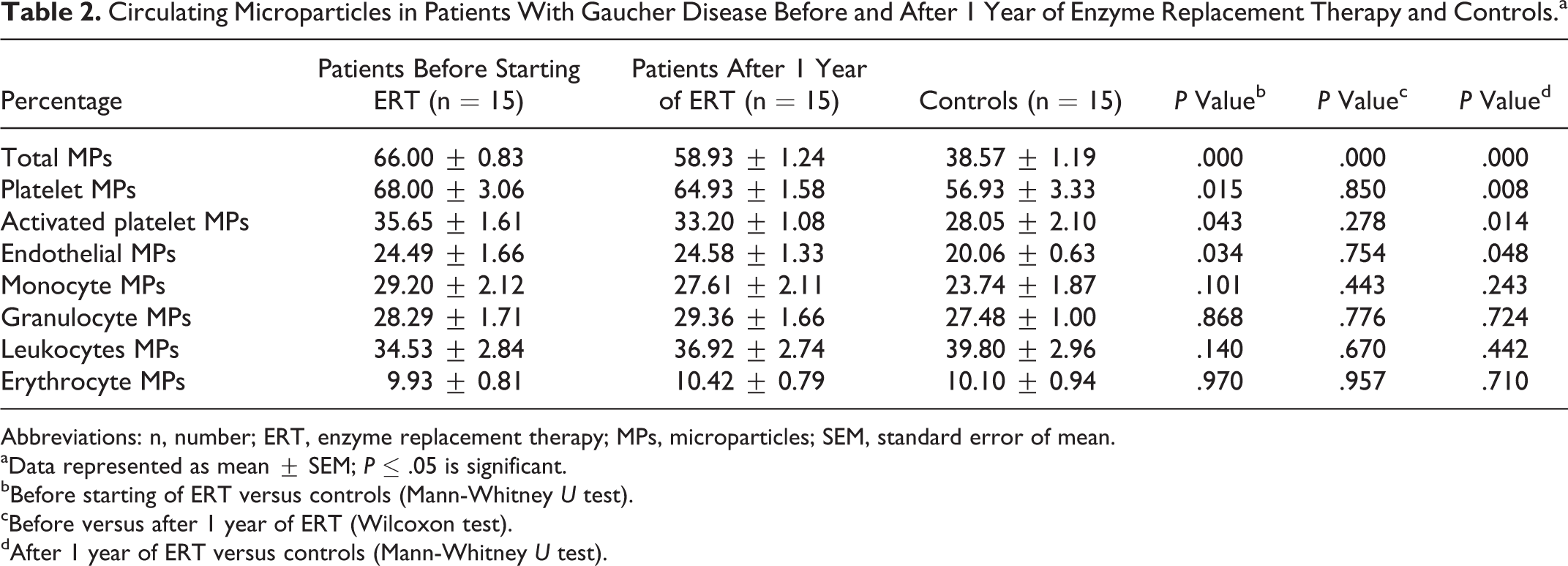
Abbreviations: n, number; ERT, enzyme replacement therapy; MPs, microparticles; SEM, standard error of mean.
aData represented as mean ± SEM; P ≤ .05 is significant.
bBefore starting of ERT versus controls (Mann-Whitney U test).
cBefore versus after 1 year of ERT (Wilcoxon test).
dAfter 1 year of ERT versus controls (Mann-Whitney U test).
Total MPs in patients with GD after 1 year of ERT were significantly decreased than the level detected before starting ERT. There was no significant difference in different types of cellular MPs in patients with GD before and after ERT. After 1 year of ERT, total MPs were still significantly higher in patients with GD than in the controls. In addition, platelet MPs, activated platelet MPs, and endothelial MPs were still significantly higher in the patients than in the controls. The MPs of other cellular origins (granulocytes, monocytes, and erythrocyte) after ERT were still not significantly different between the patients and the controls (Table 2).
Before starting ERT, there was a significant positive correlation between the mean serum level of lipid peroxide and the percentage of total MPs (r = .796; R 2 = .557; P = .000; Figure 3). There were significant positive correlations between the level of chitotriosidase and both serum level of lipid peroxide (r = .697; R 2 = .463; P = .003) and total MPs (r = .702; R 2 = .493; P = .002; Figures 4 and 5). We noted that the patients with the most severe condition (huge hepatosplenomegaly and marked delay in physical development) had higher level of lipid peroxide (7.1, 7.4, and 7.6 nmol/mL) and total number of circulating MPs (68%, 71%, and 72%). The patients with most severe skeletal abnormalities (kyphoscoliosis or avascular necrosis) had the highest level of MPs (67%, 70%, and 72%) and the lowest level of Cu (30, 32, and 38 μg/dL). The 4 patients with recurrent chest infection had the lowest levels of Se (7.2, 7.4, 8.2, and 8.5 μg/dL).
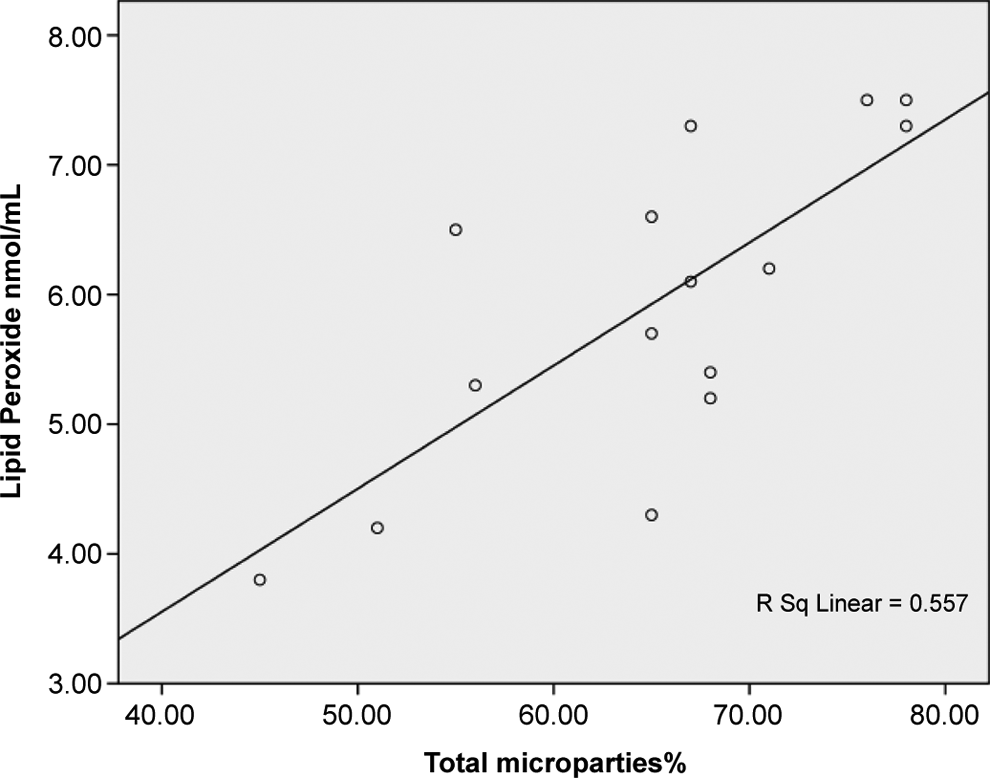
Shows positive correlation between total microparticles and lipid peroxide in patients with Gaucher disease before starting enzyme replacement therapy (ERT).
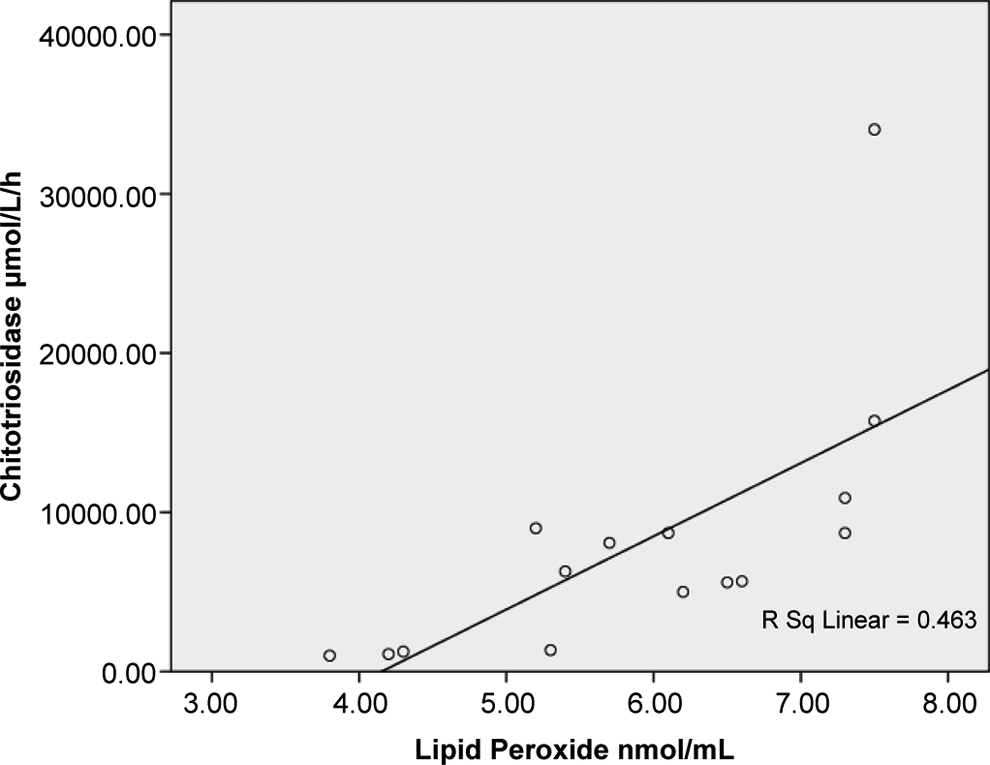
Shows positive correlation between the level of chitotriosidase and lipid peroxide in patients with Gaucher disease before starting enzyme replacement therapy (ERT).
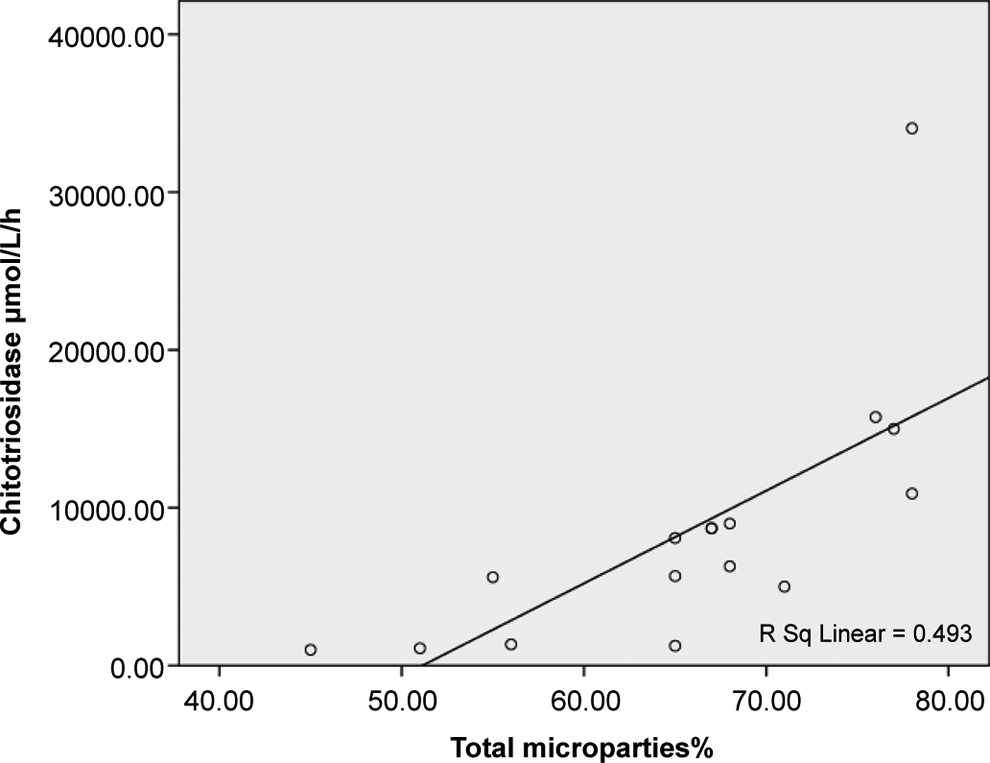
Shows positive correlation between the level of chitotriosidase and total microparticles in patients with Gaucher disease before starting enzyme replacement therapy (ERT).
Discussion
In the present study, the increased level of lipid peroxide in our patients even after 1 year of ERT indicates that they still have oxidative stress even after ERT. Lysosomes are highly susceptible to free radical oxidative stress. This is particularly important in relation to patients with GD since they have lysosomal damage. 24 Deganuto et al 2 studied the cellular behavior under acute and chronic oxidative stress conditions. They found that while the healthy cells showed an adaptive response upon oxidative stress injury, the response was completely impaired in GD cells.
Roversi et al 25 studied the lipid peroxidation in plasma of 9 patients with GD. They found no significant difference between patients and controls. The difference between our finding and their result may be due to the difference in the age and the longer duration of ERT in their patients. Kalkan et al 9 found an increase in the mean serum level of lipid peroxidation in patients with glycogen storage disease type IA and III, which is one of the lysosomal storage diseases.
In the present study, the mean serum level of NO in patients with GD before ERT was significantly higher than the controls and then returned to normal after 1 year of ERT. Our results are supported by that of Hong et al 26 who found increased level of NO from the cerebral cortex, brainstem, and cerebellum of Gaucher mice. Increased glucosylsphingosine (lysolipids) concentrations have been shown to occur in GD. 27 Lysolipids are biologically very active compounds. They are potent inhibitors of protein kinase C, interfere with the integrity of membranes, and lead to activation of inducible nitric oxide synthase (iNOS). 28,29 The NO produced by iNOS under inflammatory conditions, by itself or as a reaction product of NO with O2 − (ONOO−), is believed to be a critical factor in the pathophysiology of neurodegenerative disease. 30,31 Production of NO, which is a product of macrophages that have been activated by the cytokines and a microbial compound found in the inflammatory reaction, 32 is associated with the generation of ROS, including superoxide anions, hydroxyl radicals, lipid hydroperoxides, and hydrogen peroxide. These compounds are toxic to neurons, because they induce lipid peroxidation, DNA fragmentation, and protein oxidation. 33,34 Moreover, ROS can activate protein kinase C, mitogen-activated protein kinase, and nuclear factor κB, which regulate the expression of genes encoding a variety of proinflammatory factors. 35,36 Inflammation-mediated neurodegeneration has received considerable attention in lysosomal storage diseases. 26
After 1 year of ERT in patients with GD, the serum level of NO was returned to normal. This can be explained by a decrease in glucosylsphingosine (lysolipids) level due to the effect of the replaced enzyme, thus preventing induction of NO synthases. The mean serum levels of Zn and Cu were significantly lower in our patients than controls, both before and after 1 year of ERT. The Zn has been recognized to act as an antioxidant by replacing metals that are active in catalyzing free radical reactions, such as Fe. 37 –39 Copper is known to play an important role in the development and maintenance of the immune system. Copper deficiency leads to anemia, leucopenia and neutropenia, and osteoporosis in children. 40,41 Our patients had anemia and bone abnormalities. The lowest level of serum Cu was detected in our patients with GD who have severe skeletal manifestation (avascular necrosis or kyphoscoliosis); thus, Cu deficiency may have a role in such complications. The mean serum level of Se in the patients of the current study was lower than that in the controls both before and after ERT, but the difference was not significant. The Se is incorporated into proteins to make selenoproteins that are important antioxidant enzymes. There is also evidence that Se deficiency does not usually cause illness by itself. Rather, it can make the body more susceptible to illnesses caused by other nutritional, biochemical, or infectious stresses. 42 Four of our patients had recurrent chest infection, impaired quality of life, and lowest serum Se level among the studied patients with GD. The deficiency in the level of TEs in our patients may lead to impaired antioxidant capacity. Roversi et al 25 reported decreased antioxidants enzymes in patients with GD. Kalkan et al 9 found decreased level of Se in patients with glycogen storage disease types IA and III.
Although the total MPs were significantly decreased in patients with GD after 1 year of ERT, total MPs were significantly higher in patients with GD than in the controls both before and after 1 year of ERT. The MPs participate in hemostasis and have procoagulant potential in diseases. Microparticles contribute to inflammation via their influence on cell–cell interactions and cytokine release. The MP subpopulations are elevated in several disease states that are characterized by inflammation and vascular dysfunction. 43 In GD, glucosylceramide accumulates mainly in the cells of mononuclear phagocyte origin. Serum levels of macrophage-derived cytokines that are pro- and anti-inflammatory mediators have been variously elevated. 44 Such mediators could clearly play a role in disease progression. 45 –47 The elevated total MPs in our patients could contribute to these inflammatory process and the raised inflammatory mediators.
The elevated endothelial MPs not only constitute an emerging marker of endothelial dysfunction but also considered to play a major biological role in inflammation, vascular injury, angiogenesis, and thrombosis. Recent studies indicate that endothelial MPs are able to decrease NO-dependent vasodilatation, increase arterial stiffness, promote inflammation, and initiate thrombosis. 48 Activated platelets and circulating MPs provide a procoagulant aminophospholipid surface for the assembly of the specific enzymes of the coagulation cascade. 49
All our patients had some skeletal manifestations such as Erlenmeyer flask deformity, avascular necrosis, and kyphoscoliosis. Wenstrup et al 50 stated that skeletal manifestations of GD are associated with considerable morbidity. Patients commonly experience bone pain, and also they are at risk of pathological fractures, orthopedic interventions, and irreversible damage such as avascular necrosis. Avascular necrosis is probably the most clinically significant and disabling skeletal manifestation in GD. 51,52 Avascular necrosis occurs secondary to ischemia due to chronic infarction, and once the necrotic process starts, it cannot be reversed. 52 We believe that the increase in the procoagulant MPs, endothelial MPs, platelet MPs, and activated platelet MPs may contribute to these skeletal manifestations, especially that of avascular necrosis. After 1 year of ERT, the avascular necrosis of the head of the femur and the pain resulting from it seems to be constant and not progressive. The associated decrease in total MPs after ERT has a role in the reduction of the disease progression.
The level of chitotriosidase, which reflects the disease burden, was positively correlated with both lipid peroxide and total MPs, which means that modulation of these makers may have positive effect in decreasing complications that occurs in these patients.
Both ROS and MPs were increased in our patients. Furthermore, there was a positive correlation between the mean serum level of lipid peroxide and the percentage of total MPs. It has been stated that oxidative stress is one of the risk factors involved in increased MPs formation. 16 In addition, oxidative stress may be generated by MPs. 17
Conclusion
The GD is associated with alteration of oxidant and antioxidant status and high level of circulating MPs. The relation between oxidative stress, MPs, and inflammatory markers and their relation to various complications in GD should be explored in further study.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.