
Abstract
Background and Aims
Thromboelastography (TEG) is a non-invasive, readily available quantitative test used to assess the clotting ability of whole blood. In this study, we aim to explore the indications for utilizing TEG during the peripartum period.
Methods
A single-center, retrospective study was conducted, analyzing the electronic medical records of 288 women admitted to the labor and delivery unit, all of whom underwent TEG testing. The study period was five years. Data collected encompassed various hematological parameters; and TEG parameters with a focus on maximum amplitude (MA) were recorded. Furthermore, the diagnoses prompting TEG referral were documented for each participant.
Results
All participants were categorized into one of the following six groups: gestational thrombocytopenia (n = 41, 14.24%), immune thrombocytopenic purpura (ITP) (n = 33, 11.46%), preeclampsia (n = 27, 9.38%), preexisting coagulopathy (n = 14, 4.86%), suspected coagulopathy (n = 26, 9.03%), and massive bleeding (n = 147, 51.04%). TEG results indicated that MA values were within the normal range for the majority of participants in each category. Regional anesthesia was performed across all groups, with the following distribution: gestational thrombocytopenia (73.17%), ITP (36.36%), preeclampsia (62.96%), preexisting coagulopathy (64.29%), suspected coagulopathy (53.85%), and massive bleeding (65.46%).
Conclusions
We identified two primary reasons for performing TEG during the peripartum period: low platelet count and massive bleeding. TEG, particularly the MA parameter, plays a valuable role in peripartum management, particularly in guiding decisions regarding the suitability of neuraxial anesthesia in the presence of a low platelet count and in directing the administration of blood products in cases of massive bleeding.
Introduction
The utilization of thromboelastography (TEG) is increasing globally. TEG, first described in 1948 by Hertert, initially found its primary application in liver transplantation but has since become more widespread. This diagnostic test assesses the viscoelastic properties of clot formation in whole blood, now utilized across various surgical specialties, including cardiac surgery, trauma cases with significant bleeding potentially complicated by Trauma Induced Coagulopathy (TIC), and in determining appropriate blood product transfusion to enhance patient survival rates. TEG also holds significant importance in obstetric anesthesia. 1
TEG testing aids in identifying patients at high risk for massive bleeding and assists in selecting the most suitable anesthesia modality. 2 It serves as a crucial tool in guiding the management of massive bleeding in parturients.
Pregnancy presents a hypercoagulable state, with an increased risk of venous thrombosis, particularly in the first trimester. 3 Standard coagulation tests like prothrombin time (PT) and activated partial thromboplastin time (aPTT) may not offer sufficient information, necessitating more sensitive tests to identify high-risk groups. 4 Pregnancy is also associated with complications such as bleeding, preeclampsia, and thrombocytopenia.
For the past five years, the Department of Obstetrics and Gynecology has employed TEG. The indications for TEG testing may vary and include assessing coagulation function in parturients with low platelet counts, diagnosing platelet dysfunction, and identifying coagulation disorders. TEG results play a significant role in determining appropriate blood product administration and aiding anesthesiologists in deciding the safety of proceeding with neuraxial anesthesia.
Methods
This retrospective study aimed to explore the indications for thromboelastography testing at a university medical center between 2015 and 2020, with an average number of births of 16,000 per year. The TEG 5000 Hemostasis Analyzer System was used in this study. The range of normal TEG parameters was determined according to the manufacturer's guidelines for the TEG device.
Approval from the Institutional Review Board (Helsinki number - 0362-19, approval date 02/02/2020) was obtained prior to data collection with the need for written informed consent waived.
In this study, the Maximum Amplitude (MA) parameter from the thromboelastography (TEG) test was selected as the primary variable of interest due to its established role in reflecting the final strength of a blood clot, which is predominantly determined by platelet function and fibrinogen interaction. MA provides a direct measurement of the clot's structural integrity, which is especially critical in the obstetric population, where thrombocytopenia or coagulopathies may pose significant risks when planning neuraxial anesthesia.
Data was collected from computer records and institutional database. The study sought to answer questions regarding the reasons for TEG utilization and whether TEG testing influenced anesthetic decisions, such as the choice of anesthesia type and necessity of additional tests. Patient data from both the maternity departments and postnatal departments were entered into a table anonymously to ensure privacy.
Information for this study was sourced from the laboratories of the Department of Obstetrics and Gynecology. The data was anonymized, processed, and stored in a password-protected computer using Excel. Patient data was encoded based on the last four digits of an identification number, and the encoded data was stored securely for one year.
Data collection involved retrieving electronic patient files from databases of the medical center. Information gathered included reasons for TEG testing, demographic characteristics of each woman (such as age, gestational week, parity, and gravidity), laboratory test results (hemoglobin levels, platelet count, fibrinogen levels, and INR), details from the initial TEG test, and information regarding the type of anesthesia and type of delivery.
For the purpose of this study, thrombocytopenia was defined as a platelet count of less than 90,000; preeclampsia with severe features was defined according to American College of Obstetricians and Gynecologists (ACOG) criteria 5 ; and massive bleeding was defined as severe postpartum hemorrhage (PPH) with blood loss exceeding 2 liters according to the Royal College of Obstetricians and Gynaecologists (RCOG). 6 Suspected coagulopathy was defined as a history of bleeding in previous deliveries without laboratory confirmation of a coagulation factor deficiency. Patients with overlapping conditions were assigned to a group based on their primary diagnosis.
Statistical Analysis
Descriptive statistics are shown as mean (±SD) and as number (percentage) for categorical variables. Continuous variables were compared across groups using one-way ANOVA (using Tukey's for ANOVA) for normally distributed data followed by post hoc pairwise comparisons to identify specific intergroup differences. Normality was assessed via the Kolmogorov-Smirnov test. A P value <0.05 was considered statistically significant. Statistical analyses were carried out with the SPSS software version 30.0.0.0 (172) (IBM SPSS Statistics).
Results
The study included a total of 288 pregnant women and parturients, who were categorized into six distinct groups: gestational thrombocytopenia (41, 14.24%), immune thrombocytopenic purpura (ITP) (33, 11.46%), preeclampsia (27, 9.38%), congenital coagulopathy (14, 4.86%), suspected coagulopathy (26, 9.03%), and massive bleeding (147, 51.04%). Details regarding demographic information and laboratory test results are presented in Table 1.
Patient Characteristics.
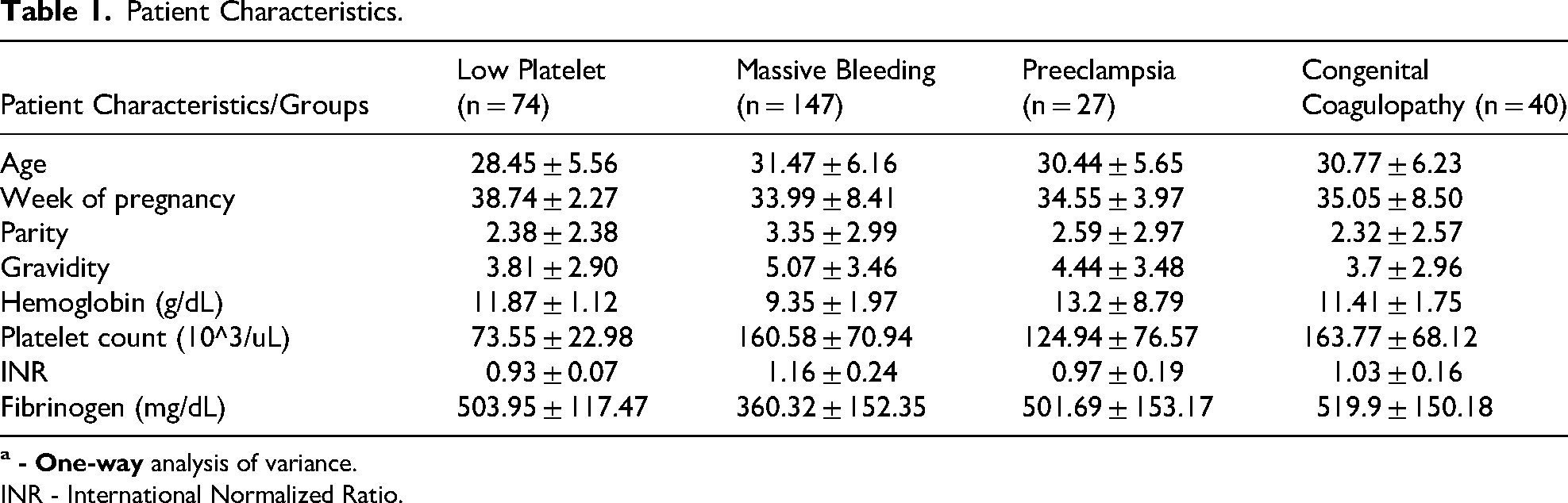
INR - International Normalized Ratio.
There were no significant differences observed across all groups in terms of demographic data, including age, pregnancy week, parity, and gravidity. However, laboratory test data revealed variations in the low platelet count within the “low platelet groups”, which comprises gestational thrombocytopenia and ITP. Additionally, lower levels of fibrinogen and higher levels of INR were noted in the severe postpartum hemorrhage (PPH) group, categorized under massive bleeding, in comparison to the other groups. When using pairwise comparison method, it was found that the levels of hemoglobin, INR, and fibrinogen in the PPH group were statistically different from all other groups (p < 0.001). The platelet count in the preeclampsia group was statistically significantly different from that in the PPH group (p < 0.001).
Details regarding TEG parameters, such as Maximum Amplitude (MA) and reaction time (R), are outlined in Table 2.
Maximum Amplitude (MA) and Reaction Time (R) Parameters.

ITP - Immune thrombocytopenic purpura.
The MA index was within normal range for the majority of parturients, indicating preserved platelet function. Even in groups with initially lower platelet counts, such as ITP and gestational thrombocytopenia, platelet function remained intact in most cases.
Table 3 illustrates that nearly all groups, particularly those with low platelet counts, proceeded with neuraxial anesthesia following the TEG test. No neurological complications following neuraxial anesthesia were reported. However, in the “massive bleeding” group, 56% of cases did not receive epidural or spinal anesthesia.
Regional Anesthesia According to Diagnosis to Proceeding with TEG.

ITP - Immune thrombocytopenic purpura.
A final table (Table 4) summarizes how parturients proceeded with labor according to groups of primary reasons for performing TEG. The four main groups include: congenital coagulopathy, preeclampsia, low platelets, and massive bleeding. From these groups, we can observe how parturients delivered: vaginal delivery, elective cesarean section, or emergent cesarean section.
Type of Delivery According to Reasons for Proceeding with TEG.

Discussion
There were 288 parturients who underwent the TEG test in our study. This test was conducted during labor due to various pregnancy complications and disorders. The significance of TEG testing in all types of pregnancy complications was discussed in reports by Butwick A. et al 7 Shreeve et al, 8 and Liew-Spilger et al 9 Among all parameters of the TEG test, only MA was discussed in our study. This parameter is crucial for assessing blood clot strength, that is mainly affected by platelet function in conditions of maternal thrombocytopenia.
In this study, we delineate the primary reasons for performing a TEG test, with one of the predominant reasons being massive bleeding and thrombocytopenia. There are no similar reports in the literature that describe reasons for TEG testing in obstetric anesthesia, and our study represents one of the largest datasets available in obstetric anesthesia for addressing this question.
We examined the platelet counts in four main groups: low platelets, massive bleeding, preeclampsia, and congenital coagulopathy. We found that low platelet levels (less than 90 (10^3/uL)) were primarily observed in the “low platelets” group (ITP and gestational thrombocytopenia) and the “preeclampsia” group. The findings of this study were consistent with those in works by Kim et al 10 and Parnas et al, 11 as well as Bernstein, 12 where similar groups with low platelet counts were identified.
In the study by Xie X. et al, 13 involving 70 parturients diagnosed with preeclampsia, the results of the MA parameter were predominantly within the normal range (MA = 55–70) in almost all cases. This aligns closely with the findings of our research. Specifically, in 24 out of 27 participants (88.88%), the MA parameter fell within the normal range (MA = 55–70), with only 2 women (7.4%) exhibiting an MA result less than 55, and one parturient (3.7%) showing an MA result exceeding 73. Similar findings were reported in a study by Wang et al, 14 further supporting the notion that preeclampsia is often associated with MA results within the normal range.
In the study conducted by Hendrickx et al 15 involving 20 patients diagnosed with preeclampsia, the results revealed no significant differences in demographic parameters, hemoglobin levels, normal clotting capabilities, and fibrinogen levels across all groups. However, they did observe MA levels within the range of 52 ± 3 across the board. In our own report, while we also found no discrepancies in demographic parameters, blood count results, or normal coagulation capabilities, there was a notable difference in the TEG results regarding the MA parameter. Specifically, we found that the MA parameter was within the normal range (between 55–70) in 24 out of the 27 (88.9%) parturient women included in our study.
In the study conducted by Snegovskikh et al, 16 which included 28 patients diagnosed with PPH, a TEG test was performed, influencing the decision regarding neuraxial anesthesia. The majority of women received neuraxial anesthesia, with 15 (53.6%) patients undergoing spinal anesthesia, 5 (17.9%) patients receiving epidural anesthesia, and 8 (28.6%) patients undergoing general anesthesia. However, our results differed from theirs. In our study, which included 147 patients with massive bleeding, after performing TEG, it was decided to proceed with neuraxial anesthesia in 64 (43.54%) patients, with 27 (18.37%) undergoing spinal anesthesia and 37 (25.17%) receiving epidural anesthesia. General anesthesia was administered to 83 (56.46%) parturient women. It is worth noting that some patients had received epidural anesthesia prior to the onset of PPH. In our study, the majority of patients in the massive bleeding group received general anesthesia.
In the report conducted by Ramanujam et al, 17 a parturient woman with severe preeclampsia experienced an acute decrease in platelet levels from 124,000 to 97,000 over 3 hours, along with a decrease in prothrombin time (PT). However, other coagulation parameters remained within the normal range. A TEG test was performed, and the results indicated normal MA levels (66.2), along with normal values for all other TEG parameters. Consequently, it was decided to proceed with spinal anesthesia. In our study, which included 27 parturient women with preeclampsia, the majority received neuraxial anesthesia. Specifically, 17 (62.96%) patients underwent neuraxial anesthesia, with 4 (14.18%) patients receiving epidural anesthesia and 13 (48.15%) patients undergoing spinal anesthesia. Additionally, 10 (37.04%) patients received general anesthesia.
In the study conducted by Roberts et al, 18 which included 372 patients diagnosed with PPH, the delivery method was examined after performing a TEG test. It was observed that 123 (33%) participants underwent vaginal delivery, instrumental vaginal delivery was performed in 87 (23%) patients, elective cesarean section took place in 64 (17%) participants, and emergency cesarean section was performed in 98 (26%) patients. In our study, which examined 147 patients with PPH, the distribution of delivery method was as follows: 40 (27.21%) patients underwent vaginal delivery, instrumental vaginal birth was performed in 5 (3.4%) patients, elective cesarean section was accomplished in 21 (14.29%) patients, and emergency cesarean section was carried out in 65 (44.22%) patients. Additionally, in the report of Rigouzzo et al, 19 which included 98 PPH patients, it was found that 52 (53.6%) women underwent a vaginal delivery, and 45 (46.4%) parturients underwent a cesarean section. These results were similar to the findings in our report.
In the Murray et al 20 report which focused on a group of 31 parturient women diagnosed with preeclampsia, standard tests including blood count and coagulation studies, as well as TEG results, were examined. The study revealed no significant difference in demographic parameters, hemoglobin levels, or normal coagulation testing results. However, the MA levels obtained in the entire group were within the range of 59 ± 4. Similarly, in our report, there were no differences observed in demographic parameters, blood count results, or normal coagulation mechanisms within this group. Additionally, there was no disparity in the TEG results for the MA parameter, which fell within the normal range (55–70) in 24 (88.88%) of parturients.
In a report by Tharp et al 21 regarding a parturient with Gaucher disease, a TEG test supported the decision to perform neuraxial anesthesia. The MA result of 59.6 indicated normal platelet function, which aligned with the findings in our report. Among the 14 patients in the “congenital coagulopathy” group, which included Gaucher disease, we found that 11 (78.57%) had MA values within the normal range, while only 3 (21.43%) had lowerthannormal results.
One important limitation of our study is the primary reliance on the MA parameter, without comprehensive analysis of other TEG variables (eg, R time, K time, and alpha angle), which also contribute to a full assessment of coagulation status. While MA is valuable for evaluating clot strength, a more complete interpretation of coagulation dynamics may have provided a deeper insight, particularly in complex or overlapping coagulation disorders.
Currently, there is insufficient evidence to confirm that a normal MA value with a platelet count below 50,000 is a safe criterion for performing neuraxial anesthesia. However, further studies are required to investigate this, and we do not rule out the possibility that regional anesthesia may be feasible even with normal or slightly lower MA values.
Conclusion
In summary, our study involved the analysis of 288 patients who underwent TEG testing due to bleeding disorders and pregnancy-related complications, including gestational thrombocytopenia, ITP, preeclampsia, congenital coagulopathy, suspected coagulopathy, and massive bleeding. The primary motivation for conducting a TEG test was one, to aid in decision-making regarding neuraxial anesthesia administration, and second, to manage circumstances involving massive bleeding.
A critical TEG parameter assessed in this study was the MA. Our findings consistently showed that MA values were within the normal range across almost all pregnancy complications evaluated. This normal MA, combined with other TEG parameters within normal limits, provided valuable guidance for safely proceeding with neuraxial anesthesia in these cases.
Footnotes
ORCID iDs
Ethical Approval and Informed Consent Statements
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Shaare Zedek Medical Center (no. 0362-19) on February 2, 2020, with the need for written informed consent waived.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used or analysed during the current study are available from the corresponding author on reasonable request.