
Abstract
The association between hereditary thrombophilia and venous thrombosis is well established but controversial data exist with respect to arterial thrombosis. We performed a pilot study on 31 patients with acute myocardial infarction (AMI), 21 patients with unstable angina (UA), and 20 healthy volunteers to investigate the role of various hemostatic gene polymorphisms in young Egyptian patients, who survived their first ischemic heart disease (IHD). Thrombophilic gene polymorphisms were tested using multiplex polymerase chain reaction and reverse-hybridization technique. We showed an increased risk of AMI with factor V (FV) Leiden and prothrombin G20210A heterozygosity. The increased risks of UA was associated with GA and A allele of fibrinogen β-455G→A polymorphism. Conversely, factor XIII (FXIII) Val34Leu GT and T allele were protective in the UA group. Nevertheless, the prevalence of FV H1299R, plasminogen activator inhibitor 1 4G/5G, glycoprotein IIIa C1565T, 5,10-methylenetetrahydrofolate reductase C677T, and A1298C mutations did not differ between patients with IHD and controls. The data have clinical implications regarding screening and thromboprophylaxis in high-risk individuals younger than 40 years.
Keywords
Introduction
Despite the continued efforts to control cardiovascular risk factors, ischemic heart disease (IHD) remains the leading cause of death worldwide, in both developed and developing countries. 1 The IHD is considered as a multifactorial disease with a complex pathophysiology generated by the combined effects of genes and the environment. Environmental influences have been widely investigated, but genetic markers have not been fully understood. 2,3
Acute coronary syndrome (ACS) is the acute manifestation of IHD that results from the formation of a platelet-rich thrombus over an atherosclerotic plaque within a coronary artery and/or a plaque rupture. The symptoms and severity of ACSs (unstable angina [UA] and myocardial infarction) vary depending on the degree to which thrombi occlude the coronary arteries. 4
Although IHD occurs usually in patients older than 45 years, younger patients having IHD have also been reported. Premature IHD is a growing entity that carries a significant morbidity, psychological effects, and financial constraints for both patients and the families. In young people, the role of genetic risk factors is expected to be even more important than that of environmental factors. 5,6 Among the genetic factors, genes involved in hemostasis may be excellent candidate risk factors for coronary artery disease (CAD). 7 Of particular importance to thrombotic complications are thrombophilia genes. 8
Although the association between inherited thrombophilia and venous thrombotic diseases is well known, 8 controversial data were reported with respect to its association with arterial thrombotic diseases such as the early-onset IHD. 9 –11 Moreover, while several studies have reported the frequency of selected thrombophilic gene polymorphisms in the Egyptian populations 12 –17 so far, no studies have investigated simultaneously the association of a wide variety of these genes with arterial thrombotic diseases or focused on younger age-group. In addition, contradiction was observed with respect to the outcomes in some of these studies at least in relation to some of these genes. This pilot study, therefore, was designed to investigate the presence of a variety of thrombophilia gene polymorphisms in association with IHD in Egyptian patients who survived their first IHD before the age of 40 years.
Materials and Methods
Patients’ Recruitment
This case–control pilot study was conducted on 52 patients admitted to Cardiac Intensive Care Unit, Cardiology Department, Specialized Medical Hospital, Mansoura University and diagnosed for the first time with IHD. We investigated 31 patients with acute myocardial infarction (AMI) and 21 patients with UA. Twenty healthy unrelated volunteers (blood donors) of matched age and sex were recruited as a control group and were clinically proven free from IHD. The study was conducted in the period from July 2010 to February 2012, and written informed consent was obtained from all patients in this study. The patients fulfilled the following criteria: (1) age: less than 40 years, (2) nondiabetic, (3) with no history of acquired causes of thrombophilia, such as antiphospholipid antibody syndrome, recent surgery procedure or trauma, and malignancy, (4) with no history of previous myocardial infarction, congestive heart failure, prosthetic heart valves, or pacemaker, and (5) with no history of drug abuse.
Clinical and Laboratory Assessment and Risk Factors
All patients and controls were subjected to full clinical assessment, electrocardiography, and laboratory testing of fasting and postprandial glucose level, lipid profile, creatine kinase (CK) and CK-MB, and antiphospholipid antibodies and lupus anticoagulant.
Diagnosis of AMI was based on:
Detection of rise and fall of cardiac biomarker with at least 1 value above the 99th percentile of the upper reference limit together with,
evidence of myocardial ischemia with at least one of the following: Symptoms of ischemia; electrocardiogram (ECG) changes indicative of new ischemia; development of pathological Q waves.
Diagnosis of UA was based on
New cardiac symptoms and positive ECG findings with normal biomarkers.
Changing symptom pattern and positive ECG findings with normal biomarkers.
Common risk factors including hypertension, smoking, obesity, and elevated cholesterol, triglyceride, or low-density lipoprotein were also examined in each of the 2 patients’ group as well as the control.
Blood Collection and DNA Analysis
Venous blood samples from all patients and the control group were drawn from the antecubital vein into EDTA-containing tubes for genetic analysis. DNA was extracted from white blood cells using QIAamp DNA Blood Mini Kit (Qiagen, Hilden, Germany) and stored at −80°C for later use. The following polymorphisms of genes encoding proteins involved in thrombophilia were analyzed: (1) factor V (FV) Leiden, (2) FV H1299R, (3) prothrombin (PTH) G20210A, (4) factor XIII (FXIII) Val34Leu, (5) fibrinogen β (FGB)-455G→A, (6) plasminogen activator inhibitor 1 (PAI-1) 4G/5G, (7) platelet glycoprotein IIIa (GPIIIa) C1565T, (8) 5,10-methylenetetrahydrofolate reductase (MTHFR) C677T, and (9) MTHFR A1298C.
Multiplex Polymerase Chain Reaction and Reverse Hybridization
The CVD Strip Assay (Vienna Lab, Austria) was used to detect the previously mentioned 9 polymorphisms of genes encoding proteins involved in blood coagulation as per manufacturer’s instructions. In summary, the procedure included 3 steps: (1) DNA isolation, (2) polymerase chain reaction amplification, and (3) hybridization of amplified products to a test strip which contains allele-specific oligonucleotide probes immobilized as an array of parallel lines. Bound biotinylated sequences were detected using a streptavidin–alkaline phosphatase conjugate and color substrates.
Statistical Analysis
Individual data were collected, and differences between numeric variables were analyzed using student t test, whereas differences between nominal and categorical variables were assessed using chi-square and Fisher exact test. To assess the association between genotype and IHD, odds ratio (OR) with 95% confidence interval (CI) was calculated. Statistical significance was defined by P value <.05. All statistical analysis was performed with SPSS for windows (version 15.0, Chicago, Illinois).
Results
The basic demographic, clinical, and laboratory data of traditional risk factors in the studied groups are illustrated in Table 1. In this study, over 50% of patients diagnosed with IHD were younger than 35 years and the male/female ratios in AMI and US were 9.3 and 6.0, respectively. The coronary angiographic data of the patients are demonstrated in Table 2.
Clinical Characteristics and Risk Factors for the Studied Groups.
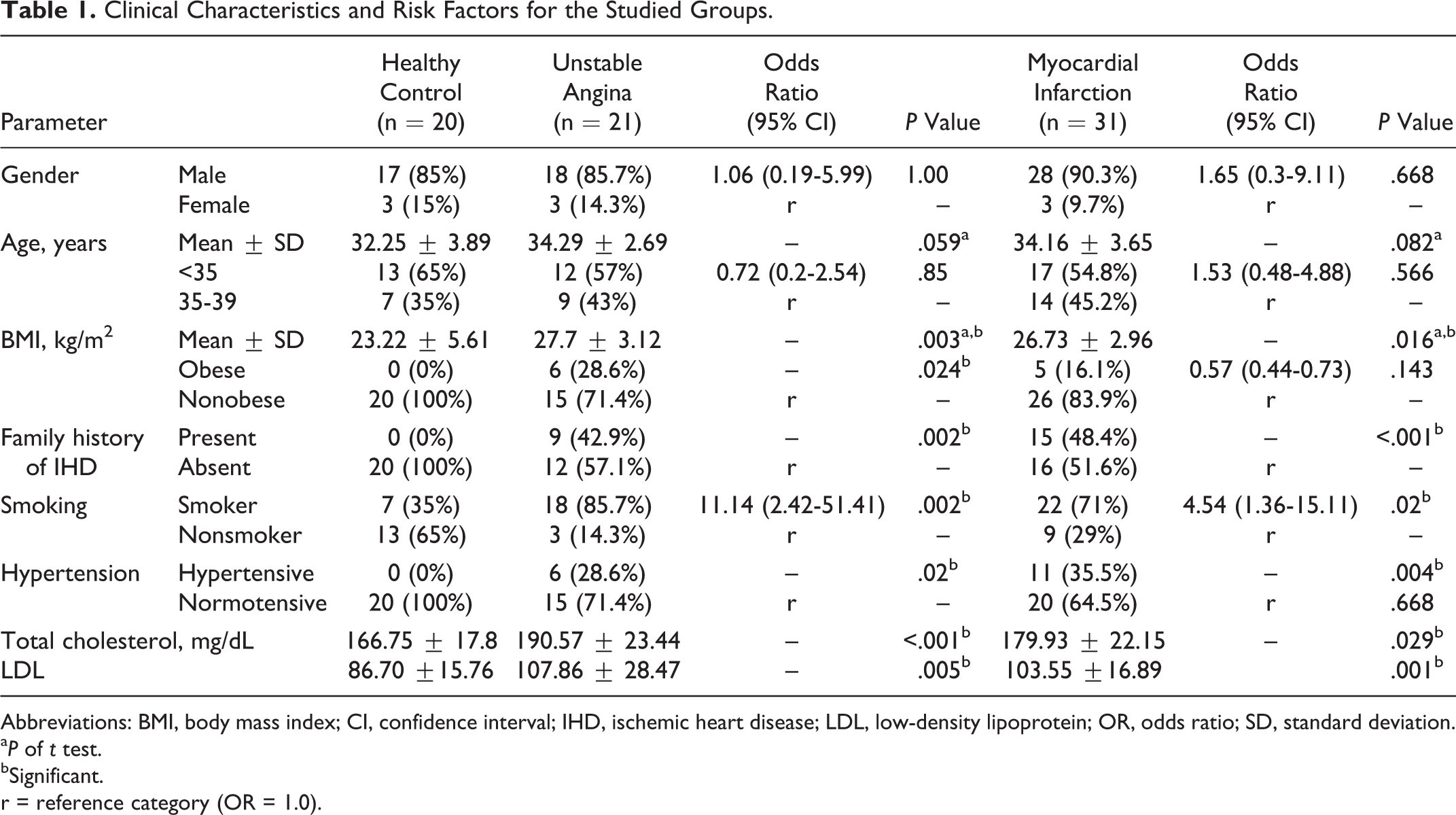
Abbreviations: BMI, body mass index; CI, confidence interval; IHD, ischemic heart disease; LDL, low-density lipoprotein; OR, odds ratio; SD, standard deviation.
a P of t test.
bSignificant. r = reference category (OR = 1.0).
Coronary Angiographic Findings in Relation to Subtypes of IHD Presentations.
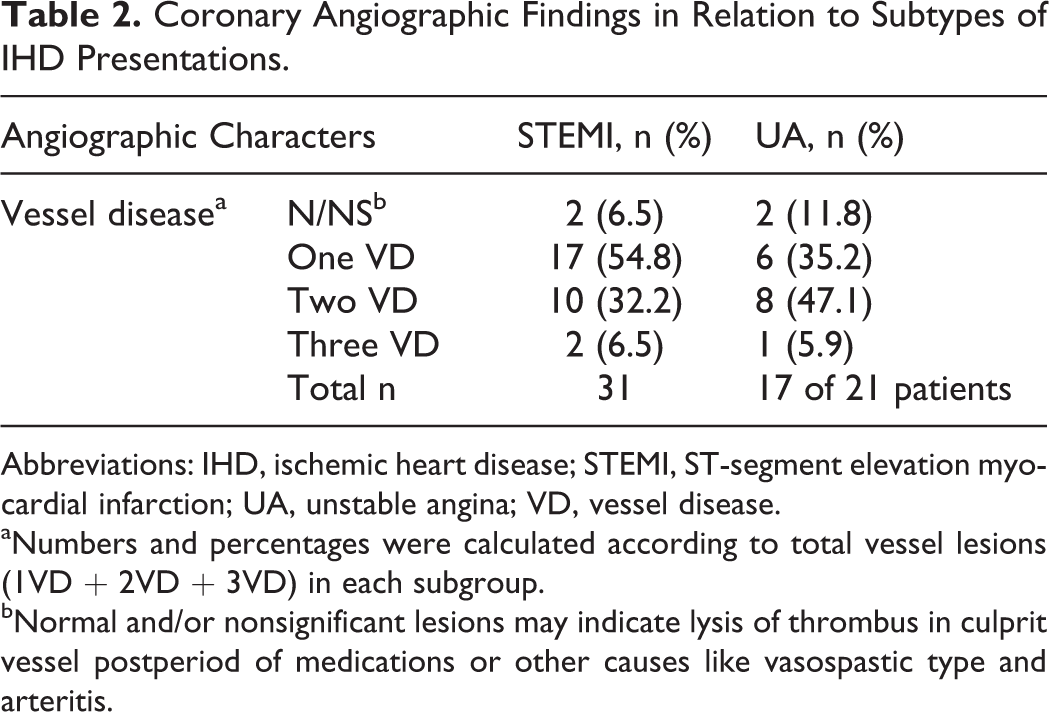
Abbreviations: IHD, ischemic heart disease; STEMI, ST-segment elevation myocardial infarction; UA, unstable angina; VD, vessel disease.
aNumbers and percentages were calculated according to total vessel lesions (1VD + 2VD + 3VD) in each subgroup.
b
cNormal and/or nonsignificant lesions may indicate lysis of thrombus in culprit vessel postperiod of medications or other causes like vasospastic type and arteritis.
Genotype and Allele Frequencies of the Studied Thrombophilia Gene Polymorphisms in Early-Onset IHD
In patients with AMI, heterozygous FV Leiden (GA) genotype showed higher prevalence (51.6%) compared to the control (15%; OR = 6.48; 95% CI: 1.56-26.84; P = .008) with (A) allele being more frequent. Similarly, heterozygous PTH 20210 (GA) genotype showed higher prevalence (45.2%) compared to the control (15%; OR = 4.67; 95% CI: 1.13-19.24; P = .035; Table 3). There was also a significant increase in the combined FV Leiden and PTH 20210A polymorphisms compared to the control group (P = .034; Table 3). Neither PTH 20210 nor FV Leiden polymorphisms were prevalent in patients with UA. Other thrombophilia gene polymorphisms did not show significance in patients with AMI compared to the control (Table 3). In patients with UA, there were a significant increase in the frequencies of heterozygous (GA) and A allele of FGB-455G→A polymorphism compared to the control group (OR = 9.0; 95% CI: 1.98-40.93; P = .004 and OR = 3.0; 95% CI: 1.12-8.05; P = .034, respectively). On the other hand, the FXIII Val34Leu polymorphism appeared to have a significant protective effect (0%) compared with the control group (20%; P = .042; Table 3). Also, there was a significant increase in the combined polymorphisms; FGB-455A and PAI 4G (OR = 9.0; 95% CI: 1.98-40.93; P = .004) compared to the control group (Table 4).
Genotype and Allele Frequencies of the Thrombophilia Gene Polymorphisms in Patients With IHD Compared With Control Group.a
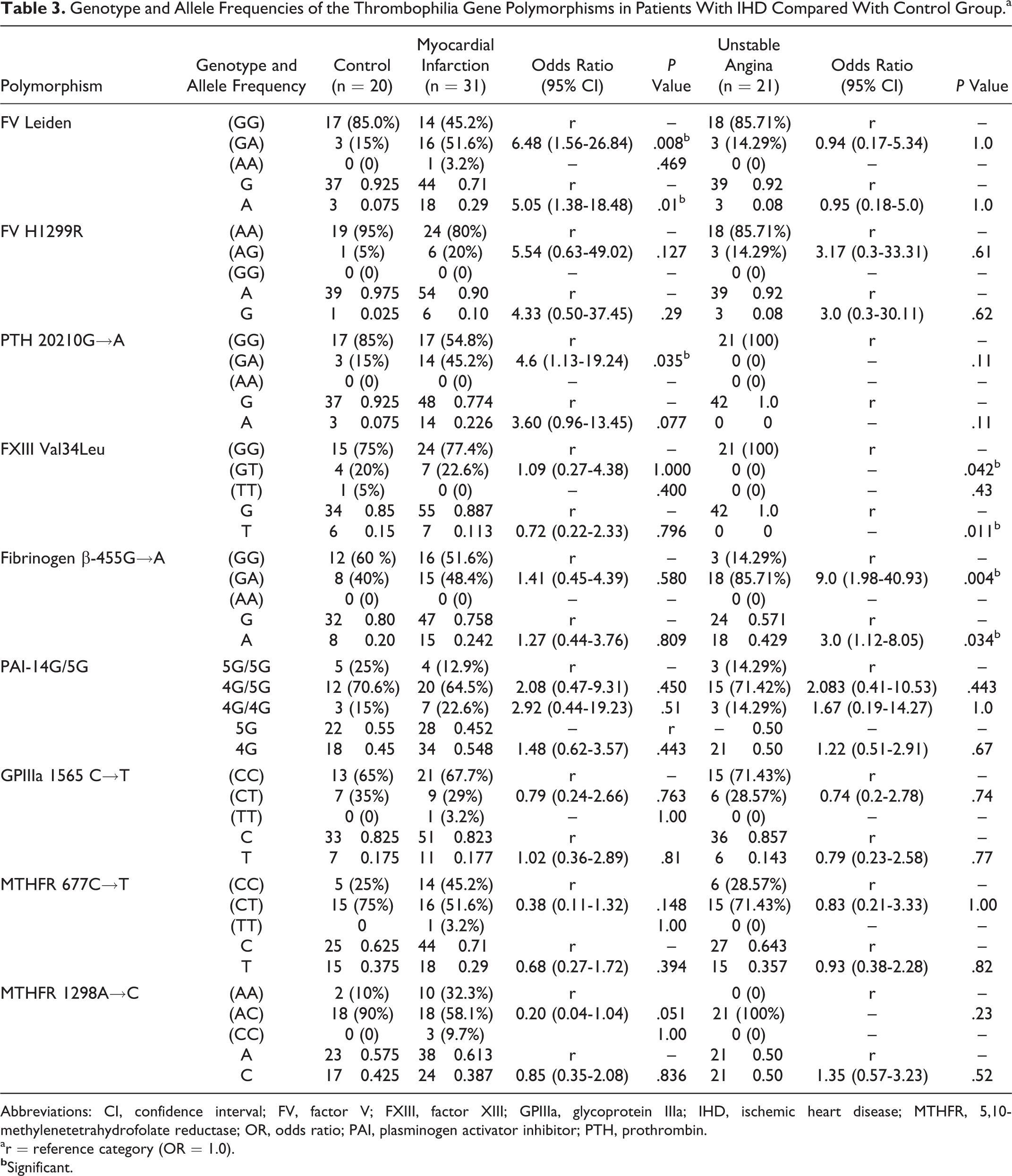
Abbreviations: CI, confidence interval; FV, factor V; FXIII, factor XIII; GPIIIa, glycoprotein IIIa; IHD, ischemic heart disease; MTHFR, 5,10-methylenetetrahydrofolate reductase; OR, odds ratio; PAI, plasminogen activator inhibitor; PTH, prothrombin.
ar = reference category (OR = 1.0).
Frequencies of Combined Thrombophilia Gene Polymorphisms in Patients With IHD Compared to Control Group.
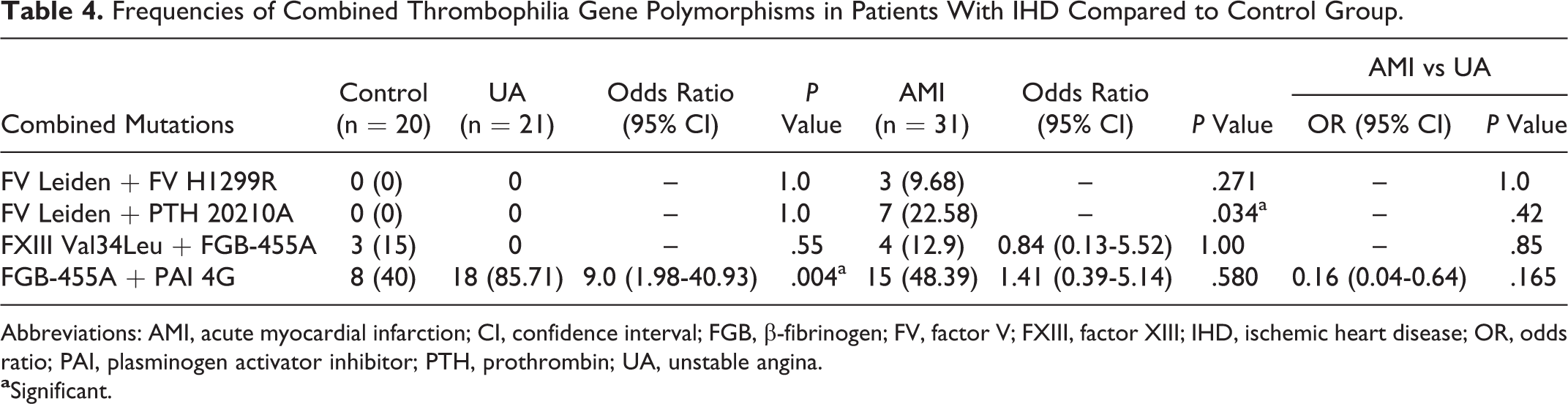
Abbreviations: AMI, acute myocardial infarction; CI, confidence interval; FGB, β-fibrinogen; FV, factor V; FXIII, factor XIII; IHD, ischemic heart disease; OR, odds ratio; PAI, plasminogen activator inhibitor; PTH, prothrombin; UA, unstable angina.
Allelic Frequencies of the Thrombophilia Gene Polymorphisms in Egyptians Compared to Other Ethnic Origins
The allelic frequencies of the studied polymorphisms in healthy Egyptians (control group in this study) compared to European, Middle Eastern, Chinese, and African healthy populations were demonstrated in Table 5. The prevalence of FV Leiden in Egypt is high and is close to Turkey and Greece, whereas that of FV H1299R is the lowest. The prevalence of PTH 20210A is among the highest prevalence among these countries, close to Turkey and Cyprus. The prevalence of FXIII Leu allele is low, same as Lebanon and close to Spain, Turkey, and Cyprus. The prevalence of FGB-455A allele in healthy Egyptians is near to other mentioned countries except China. The prevalence of PAI-1-675 4G is high near to all except Africa (low). The prevalence of GPIIIa 1565T allele in Egypt is near to Lebanon and Greece. The prevalence of MTHFR 677T allele is high, near to that of Greece and Cyprus, and the prevalence of MTHFR 1298C is near to that of other mentioned countries.
Allele Frequencies of the Thrombophilia Gene Polymorphisms in Healthy Egyptians Compared to Other Ethnic Origins.a
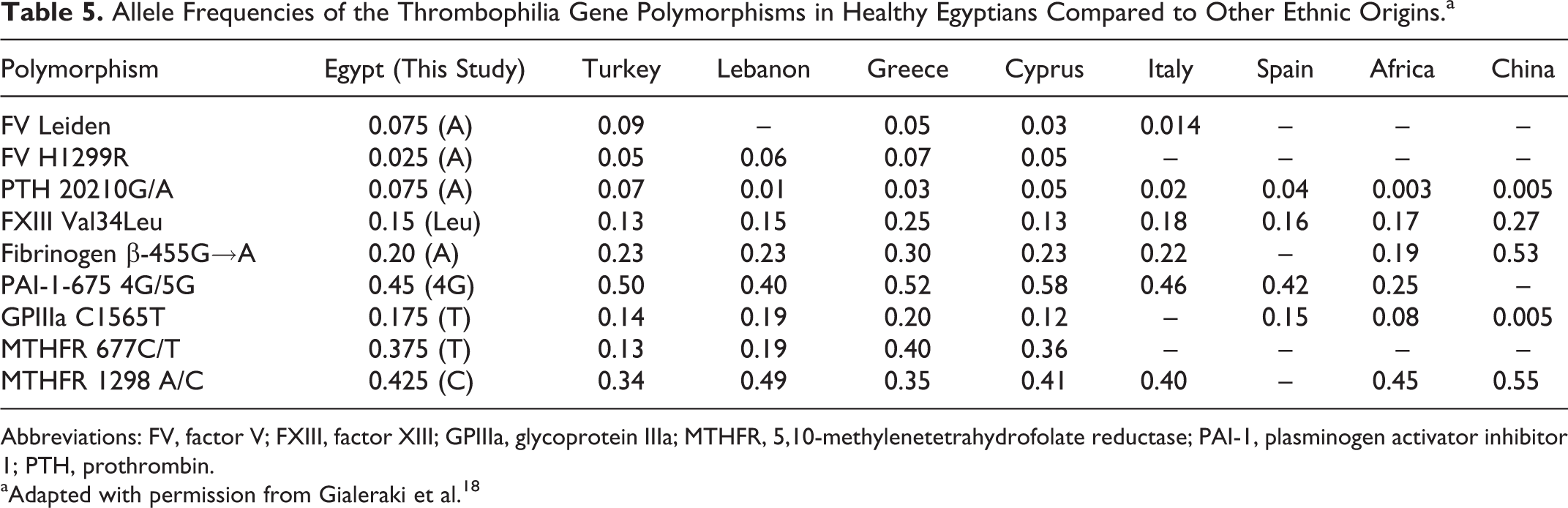
Abbreviations: FV, factor V; FXIII, factor XIII; GPIIIa, glycoprotein IIIa; MTHFR, 5,10-methylenetetrahydrofolate reductase; PAI-1, plasminogen activator inhibitor 1; PTH, prothrombin.
aAdapted with permission from Gialeraki et al. 18
Discussion
In this study, we have identified a positive association between FV Leiden and PTH G20210A heterozygosity and premature AMI development and between FGB-455G→A polymorphism and UA. Conversely, a negative association (protective role) for FXIII Val34Leu in patients with UA was observed. This indicates a potential role for hereditary thrombophilia in the development of early IHD in this population. However, the prevalence of FV H1299R, PAI-1 4G/5G, HPA1 (GPIIIa C1565T), MTHF C677, and MTHFR A1298C mutations did not differ between patients with IHD and control participants. Moreover, combined carriers of the FV Leiden and prothrombin G20210A and FGB-455-A and PAI-1 4G alleles were at high risk of AMI and UA, respectively.
Factor V Leiden, a common cause for activated protein C (APC) resistance, increases the activated form of FV leading to thrombosis. 19 In this study, there was a significant association between FV Leiden (GA) genotype and the (A) allele in patients with the AMI group compared with the control group, leading to ∼6.5-fold and ∼5-fold AMI risk, respectively. Consistent with our results, some studies have suggested that FV Leiden may be associated with early-onset AMI, 20 –22 on the other side, some studies have failed to show an association between FV Leiden and AMI. 23 –25 Our data suggested a possible thrombotic predisposition of FV Leiden for early onset of MI by causing APC resistance either by reducing the susceptibility of FVa to APC-mediated inactivation or by interfering with the APC cofactor activity of FV in FVIIIa inactivation, which ultimately facilitates the generation of more thrombin. 26 –29
The frequency of prothrombin (PTH) 20210 (G→A) gene polymorphism showed significant 3-fold increase in the heterozygous (GA) genotype in patients with AMI having premature onset compared with the control group. This may suggest that PTH 20210A allele is important for early age of onset of MI and it is agreed with a recent meta-analysis with a total of 42 case–control studies, a significantly increased risk was found during analysis of 13 studies of the subgroup of premature CAD. 30 On the other side, heterozygosity of PTH 20210G→A polymorphism was not significant risk factors for the development of AMI in patients <55 years old in many studies. 23 –25 The PTH G20210A mutation leads to increased messenger RNA and protein expression. 31 High prothrombin plasma levels may act through an increase in endogenous thrombin potential, a key step in hemostasis and thrombosis. 32 In addition, increased prothrombin levels may lead to an increase in the inhibitor of fibrinolysis, thrombin-activatable fibrinolysis inhibitor that disturbs the fibrinolysis process and therefore may add to the hypercoagulable status in these patients. 33,34
The protective role of FXIII 34Leu allele observed in our study appears to be protective in the milder IHD (UA) but not in AMI with more severe and complex pathogenicity. In addition, the smaller sample size of the UA group may statistically obviate this protective role in those patients. Although this protective role was previously shown in many studies, 35 –37 the mechanisms behind this observation are not well understood and remain to be elucidated. Possible explanations have been reported. An increased FXIII activity has been reported in carriers of the Leu allele, with Leu homozygotes having higher but Leu heterozygotes having intermediate activities compared with Val homozygotes. 38 –40 Higher FXIII activity would therefore be expected to be associated with a higher resistance of fibrin clot to fibrinolysis. Kohler et al hypothesized that increased rates of FXIII activation could lead to ineffective cross-linking or that the kinetics of the cross-linking reactions might be considerably disrupted as a result of the effects of FXIIIa on other proteins. 39
In patients with AMI of the present study, FGB-455G→A showed nonsignificant increase in the frequencies of heterozygous (GA) genotype (P = .580) and mutated allele frequencies (A) when compared to their corresponding control values. On the other side, there were significant increase in the frequencies of heterozygous (GA) and the mutated (A) allele in patients with UA compared with the control group. Consistent with our results, meta-analysis in the Chinese population found that the combined OR on the susceptibility to IHD in FGB-455A allele was 1.75. 40 Additionally, an association between this polymorphism and adverse myocardial perfusion was found. 22 In contrast, a protective effect of the mutated A allele against the development of AMI was found, with a higher prevalence of carriers of the mutated A allele in controls than in patients. 41
The Effect of This Polymorphism May Appear in the Mild Disease, UA Not in the Severe IHD, and AMI
Combined thrombophilia markers were observed in our study. Concomitant heterozygous PTH G20210A and FV Leiden genotypes comprised 22.6% of our patients with AMI compared to controls (P = .034). Individuals who are carriers of double combined heterozygous FV Leiden and PTH G20210A mutations may be particularly susceptible to increased risk of IHD compared to single FV Leiden or PTH G20210A carriers. 42 –44 It has been suggested that PTH G20210A and FV Leiden may operate partly through a common biological pathway; APC resistance, and both of which increase circulating thrombin generation. 45 Also, in patients with UA, there was a significant increase in the coincidence of FGB-455A and PAI 4G compared to controls, which results in a synergistic enhancement of prothrombotic tendency through interaction of the 2 gene products with impaired fibrinolysis. This enhanced prothrombotic tendency could result in a greater risk of UA in persons carrying both variants.
The pattern of geographical distribution of genetic risk markers is a valuable tool for population genetics and also provides data for introducing screening protocols in specific populations. The results of our study are in accordance with findings already reported in other Caucasian populations and suggest a similar distribution. Moreover, the allelic frequencies of prothrombotic polymorphisms in Egyptian controls are comparable to those observed in healthy controls in Greece, Lebanon, Cyprus, and Turkey, and populations living in the same geographic region of Eastern Mediterranean Basin. Discrepancies in results might be partly explained by the small size of the group studied or by possible genetic mixing with different populations.
Conclusions
This study is the first—to the best of our knowledge—to evaluate the role of several hemostatic gene polymorphisms in young Egyptians with IHD. Although we recognize that the small number of patients is a limitation for this study, we believe the data presented may have important clinical implications because it alerts to the potential need for (1) screening high-risk individuals younger than 40 years, (2) use specific thromboprophylaxis in well-defined groups to prevent thrombotic diseases, and (3) family studies as well as genetic counseling for those identified with high risk of inherited prothrombotic conditions. A larger study is required in order to further support their potential recommendations.
Footnotes
Authors’ Note
The project received internal support from the Department of Clinical Pathology, Mansoura University, Egypt.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.