
Abstract
Acute myocardial infarction (MI) is still a large source of morbidity and mortality worldwide. Although early reperfusion therapy has been prioritized in the modern era of percutaneous coronary intervention and thrombolysis, attempts at incremental improvements in clinical outcomes by reducing MI size have not been successful so far. Herein, we review the studies that have evaluated immediate-onset antiplatelet therapy as attempts to improve meaningful clinical outcomes in ST-segment elevation MI (STEMI). Unfortunately, many of the adjunctive pharmacotherapies have proven to be disappointing. Recent studies performed in the background of routine oral administration of P2Y12 adenosine receptor inhibitors, which may take several hours to take full effect, and aspirin have largely shown no improvement in outcomes, despite an earlier onset of antiplatelet activity of the investigative agents. Further progress in improving outcomes during STEMI may depend on exploring therapeutics that modulate the pathophysiology of microvascular damage during ischemia–reperfusion injury, a phenomenon whose effects evolve over hours to days. We speculate that the dynamic nature of the no-reflow phenomenon may be an explanation for these disappointing results with the intravenous antiplatelet agents. We hope that appreciation for what has not worked in this domain may direct future research efforts to focus on novel pathways. Myocardial ischemia and reperfusion injury are very much still a lingering issue. Despite significant improvements in door-to-balloon times, rates of in-hospital mortality for STEMI remain unchanged. Outcomes following successfully reperfused STEMI are likely determined by the initial size of myocardial necrosis (ie, cardiomyocyte death during the period of ongoing ischemia), patency of the infarct-related epicardial coronary artery, possible reperfusion injury, the microvascular no-reflow phenomenon, and adverse remodeling after infarction.
Maintaining Myocardial Perfusion During ST-Segment Elevation Myocardial Infarction
Achieving myocardial perfusion after the initial reperfusion (by thrombolysis or primary percutaneous coronary intervention [PCI]) is crucial. It is well established that platelets play a major role in initiating thrombotic (re-)occlusion of the culprit atherosclerotic lesion, stent thrombosis, and reduction of flow in the microcirculation. Therefore, aspirin and other oral antiplatelet agents are routinely used in patients presenting with ST-segment elevation myocardial infarction (STEMI). The perception is that we need additional immediate potent antiplatelet therapy before or immediately after reperfusion.
Antiplatelet therapy aims to limit platelet adhesion and aggregation, the crucial steps in thrombotic coronary occlusion. Aspirin loading (chewable or intravenous) is recommended as soon as possible after the initial encounter with any patient with suspected STEMI, per the most recent STEMI guidelines by the American College of Cardiology/American Heart Association (ACC/AHA) and the European Society of Cardiology (ESC). 1,2,3 Aspirin blocks cyclooxygenase, a mediator of the synthesis of thromboxanes and prostaglandins. Thirty years ago, the Second International Study of Infarct Survival study found that aspirin therapy within the first 24 hours after STEMI onset significantly reduced 5-week vascular and all-cause mortality. 4 After the initial loading dose, subsequent administration of low-dose aspirin (ie, 81 mg daily) is associated with lower gastrointestinal bleeding with the same cardiovascular benefit as higher daily doses. 5,6 Per the 2013 ACC/AHA STEMI guidelines, after an initial aspirin loading dose of 162 to 325 mg, a daily dose of 81 mg is often continued indefinitely for secondary prevention. 7 Likewise, the 2017 ESC STEMI guidelines recommend aspirin administration for all patients without contraindications (class I recommendation). 3
P2Y12 adenosine receptor inhibitors (eg, clopidogrel, prasugrel, ticagrelor) hinder platelet aggregation by blocking adenosine phosphate binding to the platelet receptor P2Y12. This inhibits glycoprotein (GP) IIb/IIIA complex activation, which normally assists in cross-linking of fibrin molecules. An oral loading dose of P2Y12 receptor inhibitor is to be administered at the time of primary PCI or as early as possible (eg, clopidogrel 600 mg, or preferentially prasugrel 60 mg or ticagrelor 180 mg), with daily therapy to be given for 1 year subsequently in those patients receiving a stent (ie, clopidogrel 75 mg, prasugrel 10 mg, or ticagrelor 90 mg 2 times a day). According to the 2016 ACC/AHA-focused update on dual antiplatelet therapy in patients with coronary artery disease, in patients with non-STEMI (NSTEMI) or STEMI, it is reasonable to use ticagrelor in preference to clopidogrel for maintenance P2Y12 inhibitor therapy following PCI; prasugrel may be preferred over clopidogrel for the patient without history of stroke/transient ischemic attack or increased risk of bleeding complications (both class IIa recommendations) 8 ; recent guidance from the ESC notes a preference for ticagrelor and prasugrel as well. 3,9
Other pharmacotherapeutics are used as immediate adjunctive therapy to attenuate thrombosis. The rationale behind intravenous anticoagulation is to prevent extension of the intraluminal thrombosis, which results from atherosclerotic plaque rupture. Anticoagulation is an attempt to mitigate the constant process of thrombus formation. Unfractionated heparin (UFH), with additional bolus as needed, to maintain therapeutic activated clotting time for patients with STEMI undergoing primary PCI, is a class I recommendation by the ACC/AHA task force. 7
Bivalirudin may also be used in those with or without prior treatment with UFH. No explicit recommendations were given regarding enoxaparin, given its less extensive use in this setting; use of fondaparinux as an anticoagulant by itself is advised against given the risk of catheter thrombosis. The ESC guidelines 3 recommend parenteral anticoagulation for all patients in addition to antiplatelet therapy during primary PCI, with routine use of UFH (class I recommendation) or bivalirudin in patients with heparin-induced thrombocytopenia (class I recommendation).
Oral anticoagulation has also shown promise in long-term clinical outcomes after acute coronary syndrome (ACS). In the phase 3 study of patients with recent ACS, anti-Xa Therapy to Lower Cardiovascular Events in Addition to Standard Therapy in Subjects with Acute Coronary Syndrome–Thrombolysis in Myocardial Infarction (ATLAS ACS 2-TIMI 51), 10 twice-daily 2.5 mg doses of rivaroxaban led to reduced rates of death from myocardial infarction (MI), stroke, or cardiovascular causes compared to placebo. Among patients with stable atherosclerotic vascular disease, the recent Cardiovascular Outcomes for People Using Anticoagulation Strategies trial, 11 2.5 mg rivaroxaban twice daily plus aspirin led to a reduced composite end point of cardiovascular death, MI, and stroke with more major bleeding events compared to aspirin alone. The use of rivaroxaban in this setting has been approved by European Medicines Agency but has not yet been approved by the Food and Drug Administration (FDA).
Lack of Adjunctive Benefit With Immediate Antiplatelet Therapy
The importance of long-term dual-antiplatelet therapy (DAPT) after primary PCI for STEMI has been well established. In addition to coronary stent undersizing and active malignancy, the strongest predictor of early and late stent thrombosis is discontinuation of P2Y12 adenosine receptor inhibitors at the time of the event (hazard ratio 36.5). 12 Nonresponsiveness to clopidogrel has been linked to a greater risk of subsequent adverse cardiac events. 13,14 Herein, we focus on the failure of immediate, intravenous potent antiplatelet therapy to modify clinical outcomes in the setting of STEMI. In the modern era of routine oral aspirin and P2Y12 adenosine receptor inhibitor administration, prioritizing immediate antiplatelet effect seems unlikely to lead to additional, meaningful clinical benefit in patients with STEMI as has been demonstrated in a number of clinical trials (Table 1). Table 2 describes landmark studies involving early antiplatelet therapy without the concurrent use of dual antiplatelet therapy.
Key Studies Involving Early Antiplatelet Therapy in Patients With STEMI, With the Routine Use of Dual Antiplatelet Therapy.

Abbreviations: CHF, congestive heart failure; GPIIb/IIIA, glycoprotein IIb/IIIa; IC, intracoronary; IV, intravenous; LV, left ventricle; MACE, major adverse cardiac events; MI, myocardial infarction; MVO, microvascular obstruction; PCI, percutaneous coronary intervention; STEMI, ST-elevation myocardial infarction.
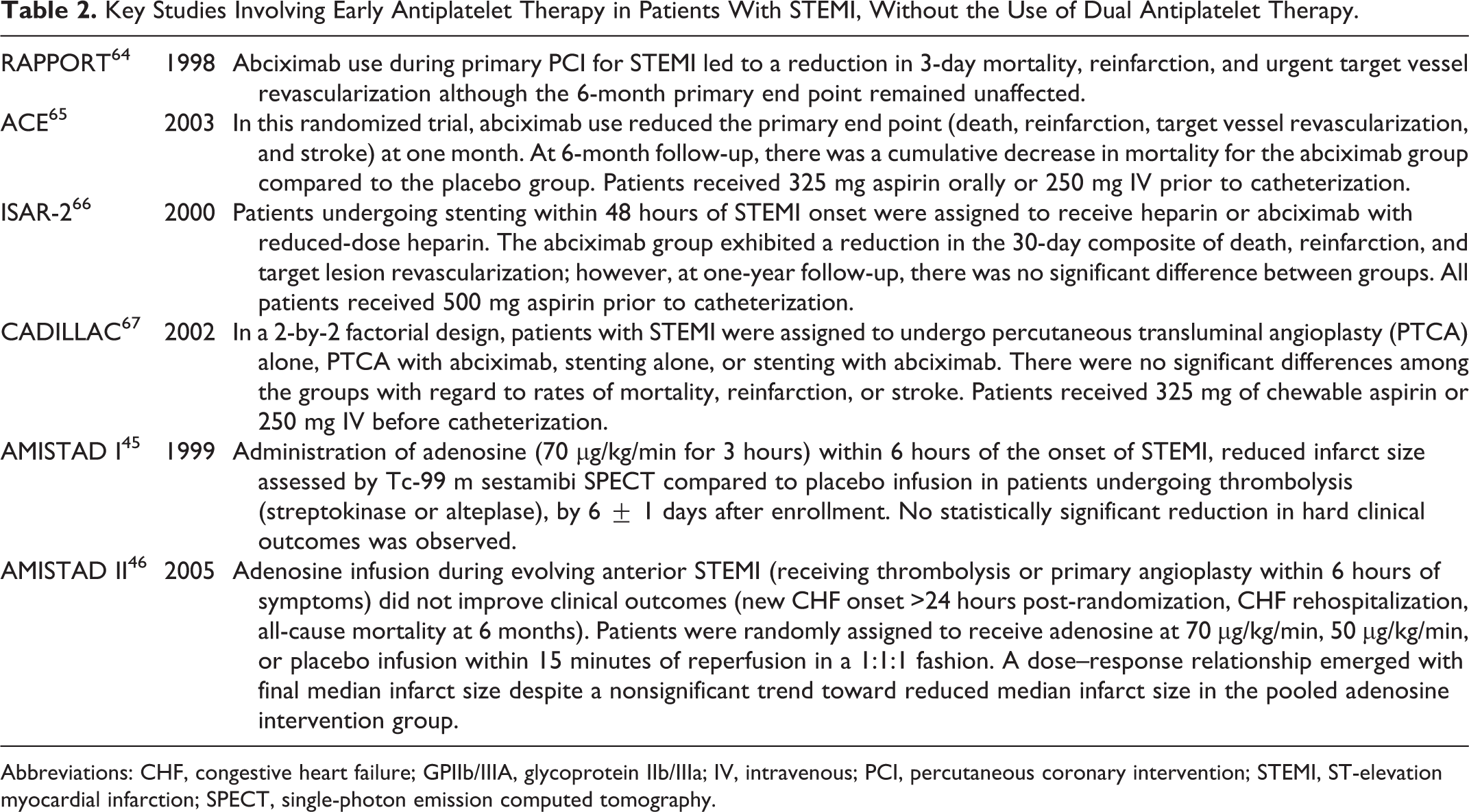
Key Studies Involving Early Antiplatelet Therapy in Patients With STEMI, Without the Use of Dual Antiplatelet Therapy.
Abbreviations: CHF, congestive heart failure; GPIIb/IIIA, glycoprotein IIb/IIIa; IV, intravenous; PCI, percutaneous coronary intervention; STEMI, ST-elevation myocardial infarction; SPECT, single-photon emission computed tomography.
Glycoprotein IIb/IIIA Inhibitors
GPIIb/IIIa inhibitor administration in isolation (eg, tirofiban) appeared to have salutary effects on the no-reflow area assessed pathologically or by myocardial contrast echocardiography in canine, 25,26 rat, 27 and porcine 28 models; however, the reperfusion times studied were only 1, 27 2, 28 or 3 hours, 25,26 which would have precluded a robust assessment of the extent of the fully developed no-reflow zone. There have been many attempts over the years to improve clinical outcomes (potentially by mitigating no-reflow and maintaining patency of the infarct related artery) with intravenous antiplatelet and anticoagulation therapies, such as the GPIIb/IIIa inhibitor class. Initial results were quite promising. 29,30 Key results of the trials investigating the use of GPIIb/IIIa inhibitors in patients with STEMI undergoing PCI are summarized in Table 1.
Although these trials, showing improvement in clinical events, illustrate the importance of antiplatelet therapy, the majority were conducted before the introduction of oral P2Y12 receptor inhibitors into the routine management of ACSs. More recent trials have not shown much benefit from routine intravenous GPIIb/IIIa inhibitor use in patients receiving aspirin and oral P2Y12 receptor inhibitors such as clopidogrel, prasugrel, and ticagrelor.
With clopidogrel loading done before catheterization in all Harmonizing Outcomes with Revascularization and Stents in Acute Myocardial Infarction study trial patients, heparin and GPIIb/IIIa inhibitor therapy (abciximab, eptifibatide, or tirofiban at operator discretion) underperformed bivalirudin anticoagulation with respect to 30-day cardiac mortality in patients undergoing primary PCI. 19 Similarly, the European Ambulance Acute Coronary Syndrome Angiography trial compared heparin and GPIIb/IIIA inhibitor (bailout use allowed with large thrombus burden or angiographically visualizing no-reflow) to bivalirudin anticoagulation started en route to the catheterization laboratory. The heparin and GPIIb/IIIa inhibitor arm underperformed with respect to 30-day major bleeding and stent thrombosis rates in patients with STEMI undergoing primary PCI. 20 A trial of acute patients with STEMI undergoing primary PCI showed no significant differences in major adverse cardiac or cerebral events in groups receiving either bivalirudin anticoagulation with a median 3-hour post-PCI infusion, heparin alone, or heparin plus tirofiban. 17 In a placebo-controlled, double-blinded randomized controlled trial in patients with STEMI with failed thrombolysis undergoing rescue PCI, the EASY RESCUE investigators found that neither intracoronary (IC) nor intravenous abciximab had significant impact on clinical outcomes (death, MI) or secondary measures compared to placebo. All patients received 325 mg aspirin and at least 300 mg of loading dose clopidogrel prior to PCI. 15 The 2017 ESC task force on the management of STEMI offers only a class IIb recommendation for GPIIb/IIIA receptor inhibitor use as bailout therapy in cases of angiographic evidence of massive thrombus burden, thrombotic complication, or no reflow. 3 Likewise, the 2013 ACC/AHA task force gives a class IIa recommendation for GPIIb/IIIA receptor inhibitors in conjunction with UFH or bivalirudin in select patients at the time of PCI (with or without stenting or prior clopidogrel loading). 7
In ACS, routine upstream initiation of GPIIb/IIIa inhibitors, compared to the deferred selective use of the drugs, did not demonstrate a statistically significant difference in composite ischemia although there was a significant increase in major bleeding. Furthermore, GPIIb/IIa inhibitor therapy and anterior wall MI have been linked to the occurrence of intramyocardial hemorrhage, which is associated with larger infarctions with poor left ventricle (LV) functional recovery compared to those with microvascular obstruction (MVO) alone. 31 Microvascular obstruction is an independent predictor of cardiac death and major adverse cardiac events (MACE). 32
P2Y12 Adenosine Receptor Inhibitors
Oral administration of P2Y12 inhibitor is standard of care in the modern era of ACS management. The efficacy of oral P2Y12 inhibition has been demonstrated in multiple key clinical trials.
A 600-mg loading dose of clopidogrel brings about adequate inhibition of platelet function after approximately 6 hours. 33 The Clopidogrel as Adjunctive Reperfusion Therapy—TIMI 28 group studied 3491 patients (18-75 years of age) presenting within 12 hours of STEMI onset. 34 Participants were assigned to either placebo or clopidogrel (300 mg loading dose with 75 mg daily thereafter); they received fibrinolytic therapy, aspirin and heparin (when appropriate). 35 The rates of the primary end point (composite of angiographic occlusion of the infarct-related artery or death or recurrent MI preceding angiography) were reduced to 15.0% in the clopidogrel group compared to 21.7% in the placebo group (P < .001). At 30 days, clopidogrel therapy was associated with reduced composite end point of cardiovascular death, recurrent ischemia necessitating urgent revascularization, or recurrent MI (11.6% vs 14.1%; P = .03).
More potent oral antiplatelet agents have also been evaluated. In the study of Platelet Inhibition and Patient Outcomes (PLATO) trial, 36 18 624 patients admitted with suspected ACS (37.5% with persistent ST Segment Elevation [STE]) were studied with treatment with ticagrelor (180 mg loading dose, 90 mg twice daily thereafter) and clopidogrel (300-600 mg loading dose, 75 mg daily thereafter). At 12 months posttreatment, the composite of death from vascular causes, MI, or stroke occurred in 9.8% of patients in the ticagrelor arm compared with 11.7% of in the clopidogrel arm (P < .001). Results of a substudy of patients with STE or left bundle branch block were similar to those of the overall trial. 37
Similarly, the TRial to assess Improvement in Therapeutic Outcomes by optimizing platelet inhibitioN with prasugrel—TIMI 38 (TRITON-TIMI) 38 demonstrated the benefits of prasugrel compared to clopidogrel in patients with STEMI. The larger effect size (3.0%) observed in the TRITON-TIMI study is likely given that PCI was carried out several days after the sentinel event and much of benefit would be observed in the first 24 hours of presentation; however, in the PLATO trial, it is difficult to distinguish between the sentinel MI and periprocedural MI as patients presented with evolving MI.
Cangrelor, an IV inhibitor of the P2Y12 adenosine receptor, was evaluated with the expectation of improved clinical outcomes, given its rapid onset compared to clopidogrel, but trial results appear to be another failure of adjunctive pharmacological therapies to improve ischemic cardiovascular disease outcomes.
The Cangrelor versus Standard Therapy to Achieve Optimal Management of Platelet Inhibition (CHAMPION) PLATFORM 39 and CHAMPION PCI 40 trials did not demonstrate clinical superiority of intravenous cangrelor over oral clopidogrel in patients with NSTEMI, STEMI, or stable angina pectoris undergoing PCI. In both randomized controlled trials, cangrelor was infused intravenously throughout PCI or for 2 hours, whichever period was longer. In the later CHAMPION PHOENIX study (stable angina 57.0%, NSTEMI 25.4%, STEMI 17.6% of the patients), 41 cangrelor reduced the rate of ischemic events compared to clopidogrel alone in patients undergoing urgent or elective PCI. However, the effect size was small: the absolute risk reduction of the primary end point, a composite of death, MI, ischemic-driven revascularization, and stent thrombosis at 48 hours post-randomization, was 1.2% in the cangrelor arm compared to the control arm. There was a 0.1% absolute risk reduction (P = .02) in MI at 48 hours postrandomization. All-cause mortality and cardiovascular mortality were not statistically different between both arms.
Nevertheless, the United States FDA approved cangrelor in June 2015 as adjunctive therapy to PCI in patients with inadequate prior treatment with a P2Y12 receptor inhibitors and who were not to receive GPIIb/IIIa/inhibitors in the planned clinical course (GPIIb/IIIa). The 2017 ESC STEMI guidelines suggest cangrelor may be considered in patients not receiving pretreatment with oral P2Y12 receptor inhibitors at the time of PCI or those who are considered unable to absorb oral agents. 3
In the CHAMPION PLATFORM trial, over 5000 patients (NSTEMI, 59.4% unstable angina 35.4%, stable angina 5.2% of the patients) were assigned randomly to receive either placebo or cangrelor infusion 30 minutes prior to PCI. A loading dose of 600 mg of clopidogrel was administered to both study arms following the procedure. The study failed to show a significant difference in the primary composite end point (death, MI, or ischemia-drive revascularization). 39 In the CHAMPION PCI trial, over 8000 patients (11% STEMI, 49.2% NSTEMI, 24.7% unstable angina, 15.1% stable angina) were randomly assigned to receive either 600 mg clopidogrel or IV cangrelor infusion 30 minutes before PCI. The same primary composite end point (death, MI, ischemia-drive revascularization) was measured and found to not significantly differ between the 2 intervention arms. 40
Notably, the ATLANTIC trial demonstrated that prehospital oral loading with ticagrelor in patients with STEMI did not improve pre-PCI coronary reperfusion compared to loading in the catheterization laboratory. However, the median time difference in administration between the prehospital and the control arm was only 31 minutes. 18
The ACC/AHA Task Force recommend the administration of a loading dose of a P2Y12 inhibitor (ie, clopidogrel 600 mg, prasugrel 60 mg, or ticagrelor 180 mg) in addition to aspirin 162 to 325 mg in the setting of STEMI 7 ; a recent guideline-focused update reveals a preference for prasugrel or ticagrelor for maintenance DAPT therapy. Similarly, European guidelines advise administration of a potent P2Y12 inhibitor (ticagrelor or prasugrel) or clopidogrel, if these are unavailable, before (or at least at the time of) PCI, in the absence of contraindications. Of note, the Task Force did not insist on P2Y12 inhibitor loading prior to PCI. The risk of bleeding relating to coronary artery bypass graft surgery has been described in loading with clopidogrel, 42 prasugrel, 43 and ticagrelor. 36 Withholding P2Y12 inhibition may be desired if surgery is anticipated, as in cases of previously discerned coronary anatomy, clinically significant valvular disease, or those suffering mechanical complications of MI.
Adenosine
Adenosine, a purine nucleoside, primarily elicits smooth muscle relaxation in the coronary microcirculation, but it also exerts antiplatelet effects. The binding of this metabolite to G-protein-coupled adenosine receptors leads to increased intracellular cyclic adenosine monophosphate, a potent platelet activity inhibitor. 44
The administration of adenosine as adjunctive therapy to reperfusion during STEMI was first evaluated in the Acute Myocardial Infarction STudy of ADenosine (AMISTAD) trials (Table 1). In the AMISTAD I trial, 45 administration of adenosine (70 μg/kg/min for 3 hours) within 6 hours of the onset of STEMI reduced infarct size assessed by Tc-99 m sestamibi single-photon emission computed tomography compared to placebo infusion in patients undergoing thrombolysis (streptokinase or alteplase), by 6 ± 1 days after enrollment. A 33% relative reduction in infarct size was seen with adenosine (P = .03), although no statistically significant reduction in hard clinical outcomes was observed.
In the AMISTAD II trial, 46 adenosine IV infusion during evolving anterior STEMI (thrombolysis or primary angioplasty within 6 hours of symptoms) did not improve clinical outcomes (new congestive heart failure [CHF] onset >24 hours postrandomization, CHF rehospitalization, all-cause mortality at 6 months). Patients were randomly assigned to receive adenosine infusion at 70 μg/kg/min, 50μg/kg/min, or placebo infusion within 15 minutes of reperfusion in a 1:1:1 fashion. A dose–response relationship emerged with final median infarct size: 27% (of left ventricle) in the placebo group, 23% with the low-dose group (P = nonsignificant vs placebo) and 11% with the high-dose group (P = .023 vs placebo infusion), despite a nonsignificant trend toward reduced median infarct size in the pooled adenosine intervention group. Post hoc analysis of the AMISTAD II data revealed that 3-hour adenosine infusion given when reperfusion was performed within approximately 3 hours of onset of ongoing anterior STEMI improved survival at 1 month and 6 months in addition to heart failure occurrence and heart failure rehospitalization at 6 months. 47
In the modern era, the use of adenosine as an agent to mitigate no-reflow during STEMI was examined in the Intracoronary Nitroprusside Versus Adenosine in Acute Myocardial Infarction (REOPEN-AMI) trial 23 (Table 1), which sought to determine whether IC adenosine or sodium nitroprusside after thrombus aspiration improve outcomes over thrombus aspiration alone. A total of 240 patients with STEMI having TIMI 0/1 flow grade were given adenosine, nitroprusside, or saline infusion. Aspirin and clopidogrel (600 mg) were given in the emergency department with IV abciximab (0.25 mg/kg bolus, 12-hour infusion thereafter) and heparin (5000 IU) bolus given prior to PCI. The primary end point measured was ST-segment resolution on the electrocardiogram at 90 minutes post-PCI. Adenosine, but not nitroprusside, improved ST-segment resolution, although angiographic MVO (TIMI flow grade <2 or 3 and myocardial blush grade <2) and MACE at 30 days were not significantly different among the groups. Follow-up up at 1 year of the REOPEN-AMI data 24 demonstrated lower incidence of heart failure, MI, and death with adenosine. Improved remodeling of the LV (assessed by echocardiography) was observed with the adenosine arm but not the nitroprusside arm.
In a study of 90 patients with STEMI, 3-hour continuous infusion of adenosine (70 μg/kg/min) reduced the rate of no-reflow compared to a lower adenosine dose (50 μg/kg/min) and control arms. No reflow was assessed by the ratio of the sum of ST-segment elevation in all 12 surface leads pre-PCI to the same sum counted post-PCI. 48 Left Ventricular Ejection Fraction (LVEF), assessed by echocardiography, was improved while clinical outcomes (heart failure occurrence, nonfatal MI, noncardiac death) were not impacted at 6 months postintervention. One caveat is that the permitted use of nitroprusside and verapamil in study patients clouds the isolation of the effect adenosine on its own.
Direct evidence of the effect of adenosine on delayed no-reflow, as assessed by cardiac magnetic resonance, has been scarce. In a recent trial, 16 patients with STEMI undergoing primary PCI with observed TIMI grade 0/1 flow received bivalirudin anticoagulation and were randomized to (1) primary PCI with IC adenosine 1 to 2 mg, (2) PCI with IC sodium nitroprusside 250 µg, or (3) standard PCI alone. Loading doses of aspirin as well as prasugrel or ticagrelor were given pre-PCI. However, infarct size and MVO assessed at 48 to 96 hours post-PCI by cardiac magnetic resonance were not decreased by adenosine or nitroprusside. In fact, MACEs were increased at 30 days and 6 months in the adenosine arm. If adenosine is working primarily through an antiplatelet mechanism, it is possible that its effects are masked in a background of aspirin and P2Y12 receptor inhibitor loading.
Adenosine seems to be one of few intravenous therapies to attenuate final infarct size in humans; the mechanism behind this observation—whether related to antiplatelet properties or direct cardioprotective effects has not been clarified. Although meta-analyses of adenosine therapy in the setting of STEMI have offered conflicting results on hard clinical outcomes, all analyses suggest possible improvement in surrogate measures of microvascular dysfunction (ie, TIMI grade flow and ST-segment resolution). 49 -51
Oral and Intravenous Antiplatelet Agents
Full-dose aspirin therapy on its own does not seem to prevent the no-reflow phenomenon given that most patients undergoing reperfusion in the setting of STEMI have received aspirin yet still evidence a high rate of no-reflow, 52 an outcome that we hypothesize is due to the underlying importance of delayed no-reflow during the postinfarct period. In the canine model of coronary artery occlusion, tissue plasminogen activator, 53 streptokinase, 54 and dabigatran, 55 have all failed to improve no-reflow when assessed by the thioflavin S fluorescent dye technique and the microspheres technique in the laboratory. In humans, the narrow set of pharmacological and nonpharmacological interventions that potentially attenuate no-reflow and microvascular disease have been detailed before. 56
Immediately after restoration of coronary flow, hyperemic myocardial blood flow occurs. Imaging performed soon after restoration of coronary blood flow likely underestimates the size of the no-reflow zone, 57 -59 as the area changes dynamically due to myocardial edema and vasospasm during the first 3 hours. The no-reflow zone may be fully developed as late as 48 hours postreperfusion as active changes in resting myocardial perfusion will have abated, so this may be a more ideal time to assess its extent. 58 By the time that delayed no-reflow develops and effective platelet inhibition are probably needed, blood concentrations of the oral antiplatelet agents are sufficient to exert therapeutic effects. Alternatively, the effects of the antiplatelet therapy is not on the no-reflow phenomenon. These agents may affect epicardial artery patency. Again, with the background of anticoagulation and aspirin, full effect might be needed only a few hours after reperfusion and can safely and effectively be achieved by oral therapy. It is unclear whether IV antiplatelet agents (eg, GPIIb/IIIa inhibitors and cangrelor), on top of aspirin loading and anticoagulation therapy, are truly effective against distal embolization of plaque debris.
Notably, the fact that the immediate IV agents do not have dramatic clinical effect in a background of aspirin and P2Y12 receptor inhibition may indicate that they are not effective, or that the issue of provoked thromboembolization (ie, “immediate” no-reflow), per se, is not as important as commonly believed. If indeed the full antiplatelet effect is needed only a few hours after restoration of macrovascular coronary flow and not immediately after reperfusion, oral agents administered at the time of PCI likely suffice.
Future Directions
Experimental models have failed to show a benefit to thrombolytic therapy or anticoagulation after reperfusion in reduction of the no-reflow zone. 55 Vasodilators (adenosine, nitroprusside, nitroglycerin, calcium channel blockers) have shown different degrees of mitigating clinical no-reflow. 56 Adenosine, which also demonstrates antiplatelet activity, seems to have had some benefit in mitigating no-reflow, but aggregated data are conflicting and less ideal markers of the phenomenon (ie, ST-segment resolution) were used in its assessment during key studies. 49 -51 Mechanical methods directed at thrombi have been met with disappointment, underlining the lower impact that immediate no-reflow plays in the perireperfusion period. Distal protection devices (ie, filters and balloons) have not shown any clinical benefit in mitigating no-reflow during STEMI. 60 Rheolytic thrombectomy may actually potentiate no-reflow in some patients. 61 Although aspiration thrombectomy is widely used, its use does not seem to reduce post-STEMI clinical measures (30-day post-MI mortality, reinfarction, and stroke) despite improved early markers of reperfusion (ST-segment resolution and angiographic outcome). 62 A more recent meta-analysis of long-term outcomes reported similar findings, with an actual increased stroke risk in patients undergoing the procedure. 63
We believe that the failure of early, full-dose intravenous antiplatelet therapies to demonstrate strong superiority over slower onset oral agents underlines the importance of delayed microvascular damage, which evolves over several hours after coronary reperfusion. Early spontaneous or provoked thromboembolization of plaques does not seem to drive as much of the microvascular damage and myocardial perfusion deficits in the postinfarct period, and oral antithrombotic therapy (namely, aspirin and P2Y12 inhibitor) is likely sufficient, as inhibition of platelet aggregation takes place within a couple of hours.
Thomas Edison, on inventing the light bulb, is believed to have said, “I have not failed. I’ve just found 10,000 ways that won’t work.” In examining what has not worked, we may find an avenue to approach future therapeutics in this domain.
Footnotes
Author Contributions
All the authors contributed to conception, design, acquisition, analysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Authors’ Note
The guest editor of this paper was Dr. Christopher Cannon.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.