
Abstract
We sought to determine the prognostic value of neutrophil to lymphocyte ratio (NLR) in non-ST elevation myocardial infarction (NSTEMI) and unstable angina pectoris (UAP). A total of 308 (mean age 59.22 ± 11.93) patients with NSTEMI and UAP were prospectively evaluated. The study population was divided into tertiles based on admission NLR values. The patients were followed for clinical outcomes for up to 3 years after discharge. In the Kaplan-Meier survival analysis, 3-year mortality was 21.6% in patients with high NLR versus 3% in the low-NLR group (P < .001). In a receiver–operating characteristic curve analysis, an NLR value of 3.04 was identified as an effective cut point in NSTEMI and UAP of a 3-year cardiovascular mortality (area under curve [AUC] = 0.86, 95% confidence interval [CI] 0.8-0.92). An NLR value >3.04 yielded a sensitivity of 79% and specificity of 71%. Admission NLR is the strong and independent predictor of a 3-year cardiovascular mortality in patients with NSTEMI and UAP.
Keywords
Introduction
The important role of inflammation in cardiovascular disorders is well established. 1 The presence of systemic atherosclerosis is associated with low-grade systemic inflammatory response in which leucocytes play a key role. 2 The neutrophil to lymphocyte ratio (NLR) was introduced as a potential marker to determine inflammation in cardiac and noncardiac disorders. Kaya et al found that NLR was associated with severity of coronary artery disease (CAD) 3 . The NLR is the strongest white blood cell (WBC) predictor of adverse outcomes for stable CAD, 4 long-term mortality in ST-segment elevation myocardial infarction (STEMI), and in-hospital and 6-month mortalities in acute coronary syndromes (ACS). 5,6 Despite the diversity of NLR research, no prospective study has yet been addressed evaluating the relationship between NLR and long-term adverse outcomes in populations who have non-STEMI (NSTEMI) and unstable angina pectoris (UAP). We sought to determine the prognostic value of NLR in NSTEMI and UAP.
Materials and Methods
This prospective study population consisted of 308 patients (234 men and 74 women; range 30- 80 years) who were admitted to the emergency department of Siyami Ersek Thoracic and Cardiovascular Surgery Center from January 2008 to December 2008 because of NSTEMI and UAP. All patients presented to the emergency department with acute chest pain. Initially, 386 patients were screened, but 326 patients were found to be eligible according to the inclusion criteria. Finally, 18 patients were excluded due to loss of follow-up, and the study was completed with 308 patients. Exclusion criteria included age >80 years, clinical evidence of active infection, malignant neoplasia, hematologic proliferative diseases, active or chronic inflammatory or autoimmune diseases, steroid therapy or chemotherapy, concomitant STEMI, and unavailable complete blood cell count (CBC). All women were postmenopausal, and none were receiving hormone-replacement therapy. Patients who were lost to the 3-year follow-up were also excluded. The local ethics committee gave approval for the study.
The study population was divided into tertiles based on the admission NLR values. First tertile (n = 104) NLR ≤ 1.8, second tertile (n = 102) NLR ≤3.04, and third tertile (n = 102) NLR > 3.04. A high NLR (n = 102) was defined as a value in the third tertile (>3.04), and a low NLR (n = 206) was defined as a value in the lower 2 tertiles (≤3.04).
The UA/NSTEMI is defined by electrocardiographic (ECG) prominent T-wave inversion or ST-segment depression and/or positive biomarkers of necrosis (eg, troponin, creatine kinase-MB [CK-MB]) in the absence of ST-segment elevation and in an appropriate clinical setting (anginal equivalent or chest discomfort). The basic drug treatment for UAP/NSTEMI included antiplatelet agents, beta-blockers, angiotensin-converting enzyme inhibitor (ACE-I)/ angiotensin receptor blocker (ARB), and statins. The thrombolysis in myocardial infarction (TIMI) risk score was calculated from the initial clinical history, ECG, and laboratory values collected on admission. Calculation of the Global Registry of Acute Coronary Events (GRACE) risk score was based on the clinical history, ECG, and laboratory values at the first arrival to the coronary care unit (CCU) or the acute medical admissions unit. 7
At admission, medical history and a special questionnaire on lifestyle and risk factors were obtained from each patient. Hypertension (HT) was defined as the previous use of antihypertensive medications, a systolic pressure more than 140 mm Hg, or a diastolic pressure more than 90 mm Hg for at least 2 separate measurements. Diabetes mellitus (DM) was defined as a previous diagnosis, use of diet or antidiabetic medicines, or fasting venous blood glucose level of 126 mg/dL on 2 occasions in previously untreated patients. Hypercholesterolemia was defined as total cholesterol ≥ 200 mg/dL. Smoking was defined as the current regular use of cigarettes. Body mass index (BMI) was calculated as the weight in kilograms divided by the square of the height in meters. Quantitative assessment of left ventricular systolic function was performed using the modified biplane Simpson’s method to calculate a left ventricular ejection fraction (LVEF). 8 Contrast-induced nephropathy (CIN) was defined as an increase in serum creatinine level ≥0.5 mg/dL or ≥25% from the baseline (admission) within 72 hours of radiocontrast administration. Anemia was defined as a baseline hemoglobin concentration < 13 mg/dL in men and < 12 mg/dL in women. Patients were also evaluated according to Killip clinical examination classification. 9 Admission glomerular filtration rate (GFR) was estimated by the simplified Modification of Diet in Renal Disease (MDRD) equation. 10 For the diagnosis of metabolic syndrome at the baseline we followed the National Cholesterol Education Program Adult Treatment Panel III criteria. 11
Blood Samples and Laboratory Assay
On admission, venous blood was obtained from all the patients. Neutrophils, lymphocytes, hemoglobin, NLR, hematocrit, and WBC were measured as part of the automated CBC using a Coulter LH 780 Hematology Analyzer (Beckman Coulter Ireland Inc, Mervue, Galway, Ireland). The NLR was calculated as the ratio of the neutrophils and lymphocytes, both obtained from the same automated blood sample at admission of the study. Troponin I, CK-MB, and other biochemistry measurements were carried out by our biochemistry department using the standard methods. Within 72 hours after admission CK-MB was measured daily and the maximum was recorded. The 12-hour fasting serum levels of total cholesterol, triglyceride, and low-density lipoprotein (LDL) and high-density lipoprotein (HDL) cholesterol were measured by standard enzymatic methods.
Assessment of Cardiovascular Events
All patients were followed up for up to 3 years after discharge using a standardized protocol that included telephone contacts and outpatient visits, and recurrent cardiac events were recorded at 30 days, 6 months, and 3 years. The primary end point was cardiac death. A death was classified as cardiac if the primary cause was related to myocardial infarction (MI), arrhythmia, refractory congestive heart failure, or sudden death. The secondary end point of the study was reinfarction, stroke, and heart failure. Hospitalization for heart failure was defined by the presence of new symptoms of dyspnea with pulmonary venous congestion on x-ray with interstitial or alveolar edema requiring hospitalization. Reinfarction was defined as an elevation in serum CK-MB levels twice the upper limit of normal and ST-segment reelevations.
Statistical Analysis
Qualitative variables were expressed as percentages (%), and quantitative variables were expressed as mean value ± standard deviation (SD). Comparison of parametric values between the 2 groups was performed by means of 2-tailed Student t test. Categorical variables were compared by the likelihood ratio Chi-square or Fisher exact test. Correlations between the NLR and the other parameters were assessed using Spearman rank correlations test.
The variables were selected using backward stepwise logistic regression analysis, entering all those with a significant or borderline (P < .1) association with NLR. A backward stepwise multivariate Cox regression analysis, which included variables with P <.1 was performed to identify independent predictors of cardiovascular mortality, including DM, HT, smoking habit, peripheral arterial disease, age ≥75, admission anemia, GRACE risk score, TIMI risk score, GFR < 60, Killip class > 1, LVEF < 40%, treatment (percutaneous coronary intervention [PCI]/coronary artery bypass grafting [CABG]), ST-segment depression > 1 mm, troponin I, peak CK-MB, and NLR. The cumulative survival curves for cardiovascular mortality and reinfarction were constructed using the Kaplan-Meier method with differences assessed using the log rank test. A P < .05 was considered statistically significant. All statistical studies were carried out with the program SPSS (version 15.0, SPSS, Chicago, Illinois).
Results
Baseline Characteristics
Demographic and clinical characteristics of individual groups are listed in Table 1. The patients of high-NLR group were older and had class Killip >1 at admission when compared to the patients of the low-NLR group. The TIMI and GRACE risk scores were significantly higher in the high-NLR group than the low-NLR group. Smoking was higher in the low-NLR group than the high-NLR group. The incidence of CIN was higher in the high-NLR group than the low-NLR group. Mean LVEF was less in the high-NLR group. The low-NLR group showed higher treatment rates with PCI and CABG. Other baseline characteristics were not statistically different between the 2 groups (Table 1).
Baseline Characteristics of Study Patients.a
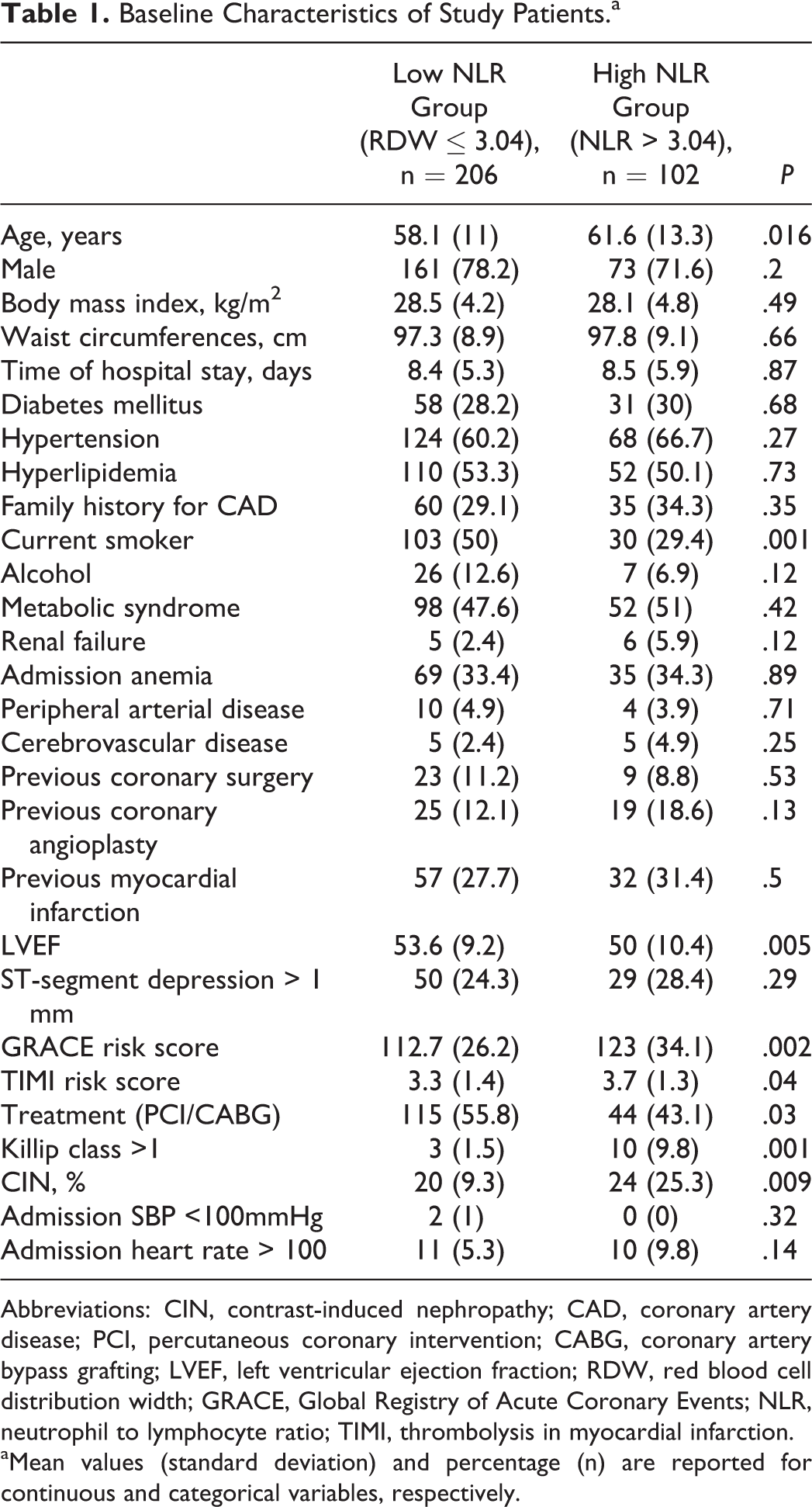
Abbreviations: CIN, contrast-induced nephropathy; CAD, coronary artery disease; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting; LVEF, left ventricular ejection fraction; RDW, red blood cell distribution width; GRACE, Global Registry of Acute Coronary Events; NLR, neutrophil to lymphocyte ratio; TIMI, thrombolysis in myocardial infarction. aMean values (standard deviation) and percentage (n) are reported for continuous and categorical variables, respectively.
Table 2 lists the laboratory data. There were significant higher levels of troponin-I and peak CK-MB in the higher NLR group. A lower TG level and higher high-density lipoprotein (HDL) level were found in the higher NLR group. Unsurprisingly, the WBC value was higher in the high-NLR group than the low-NLR group. Other laboratory characteristics were not statistically different between the 2 groups (Table 2).
Laboratory Findings of Patients.a
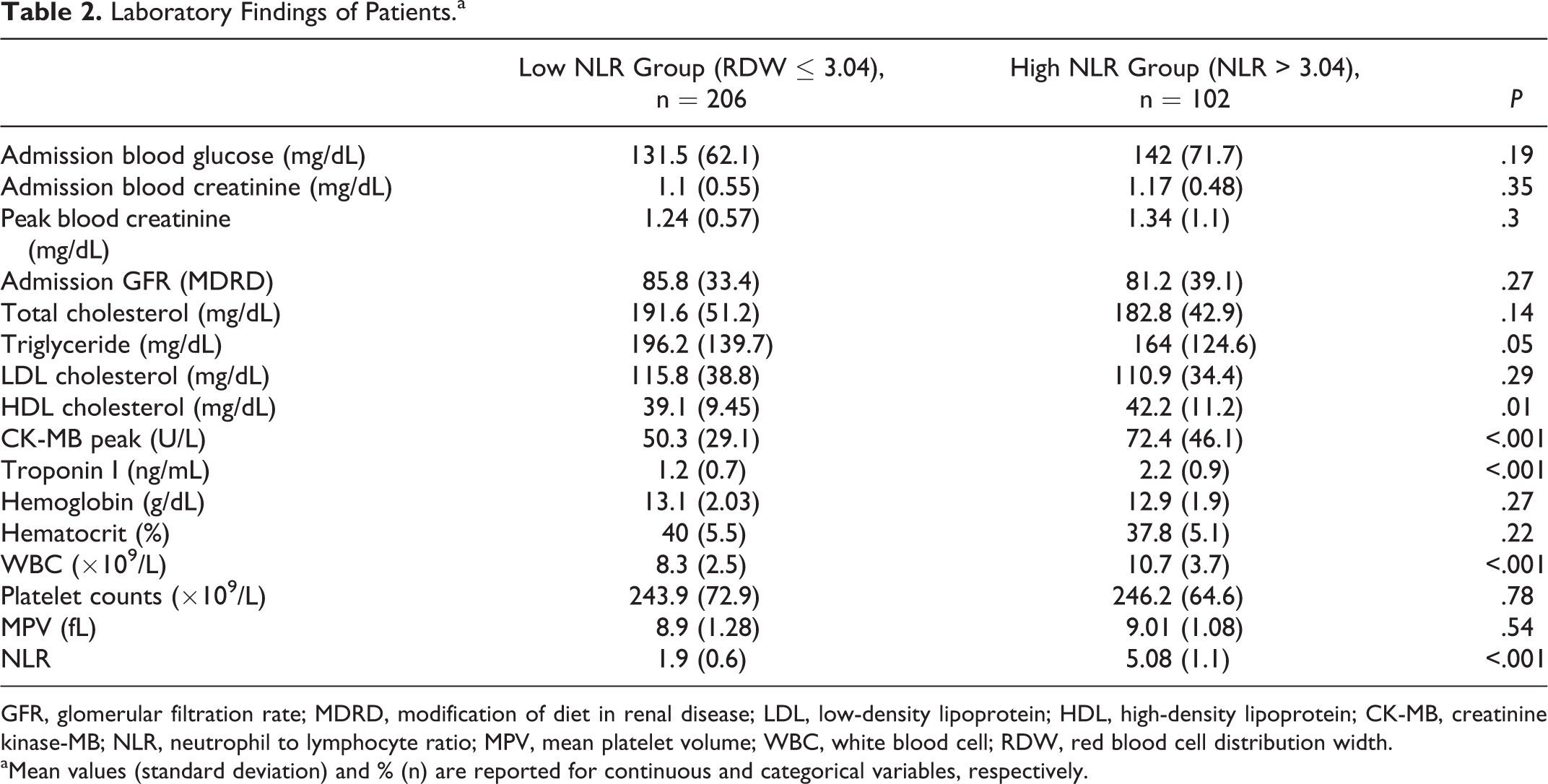
GFR, glomerular filtration rate; MDRD, modification of diet in renal disease; LDL, low-density lipoprotein; HDL, high-density lipoprotein; CK-MB, creatinine kinase-MB; NLR, neutrophil to lymphocyte ratio; MPV, mean platelet volume; WBC, white blood cell; RDW, red blood cell distribution width.
aMean values (standard deviation) and % (n) are reported for continuous and categorical variables, respectively.
Table 3 presents the in-hospital adverse outcomes. Cardiopulmonary resuscitation, advanced heart failure, and cardiogenic shock were noted more often in the high-NLR group than the low-NLR group. Other complications were not statistically different between the 2 groups (Table 3).
In-Hospital Cardiac Events and Complications.a
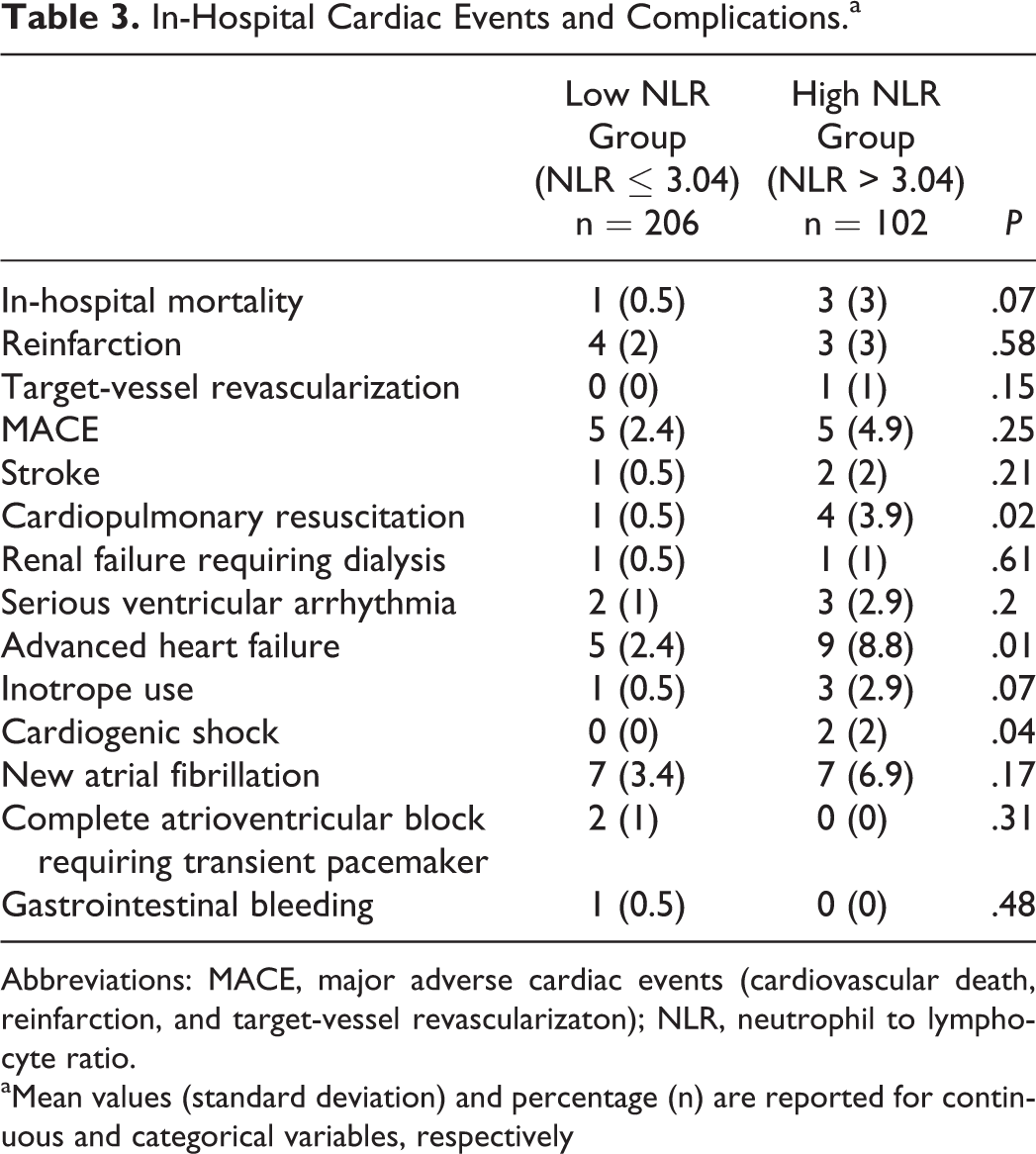
Abbreviations: MACE, major adverse cardiac events (cardiovascular death, reinfarction, and target-vessel revascularizaton); NLR, neutrophil to lymphocyte ratio.
aMean values (standard deviation) and percentage (n) are reported for continuous and categorical variables, respectively
Correlation of NLR With Other Parameters
There was a good positive correlation between the NLR levels and the age, TIMI risk score, GRACE risk score, WBC, CK-MB peak, troponin I, and admission glucose. There was a negative correlation between the NLR and the GFR and LVEF. We did not observe any significant correlation between NLR and other parameters (Table 4).
Spearman Correlations Analysis Between Neutrophil to Lymphocyte Ratio and Other Parameters.
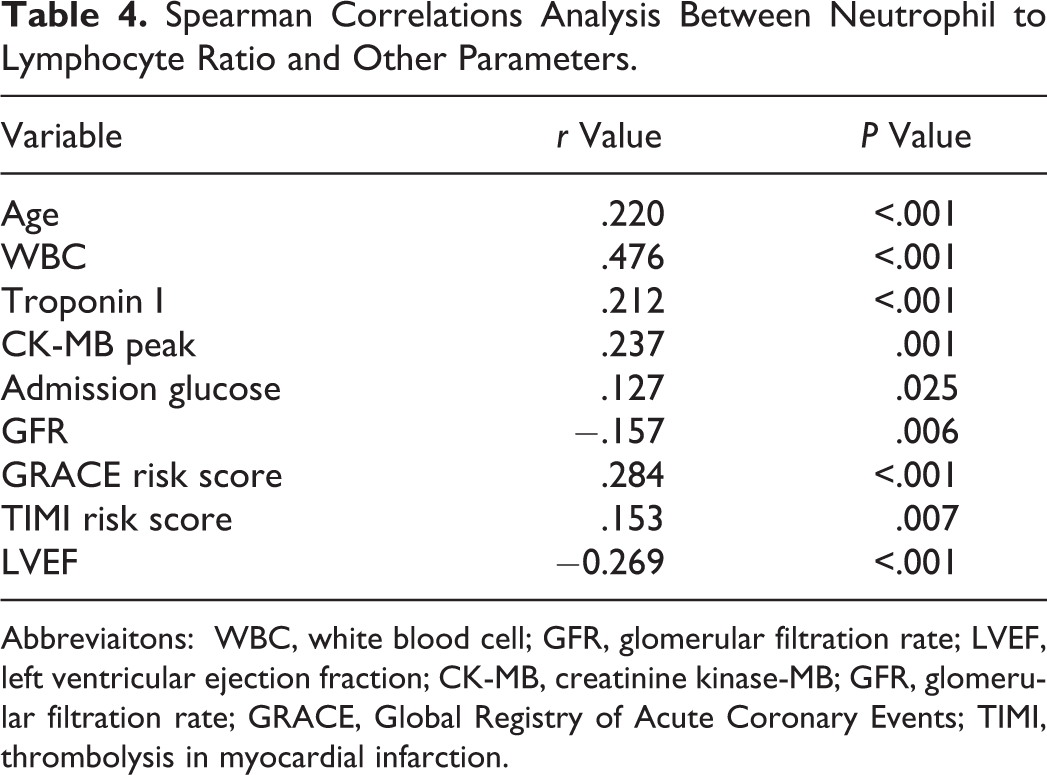
Abbreviaitons: WBC, white blood cell; GFR, glomerular filtration rate; LVEF, left ventricular ejection fraction; CK-MB, creatinine kinase-MB; GFR, glomerular filtration rate; GRACE, Global Registry of Acute Coronary Events; TIMI, thrombolysis in myocardial infarction.
Neutrophil to Lymphocyte Ratio and Follow-up
Table 5 presents adverse outcomes at 30 days, 6 months, and 3 years. A total of 30 deaths, 2 noncardiac and 28 cardiovascular deaths (6 in the low-NLR group and 22 in the high-NLR group), occurred in the 3-year follow-up. The incidence of the primary end point, 3-year cardiovascular mortality, was higher in the high-NLR group (P < .001). Mortality was significantly higher at 30 days and at 6 months in the high-NLR group compared to the low-NLR group (P:.03 and P < .001, respectively). There was significantly higher 3-year reinfaction (24.5%) in the high-NLR group compared to the low-NLR group (11.2%). Hospitalization for heart failure was higher at 3 years in high-NLR group. Other complications were not statistically different between the 2 groups (Table 5).
Follow-Up Cardiaovascular Events.a
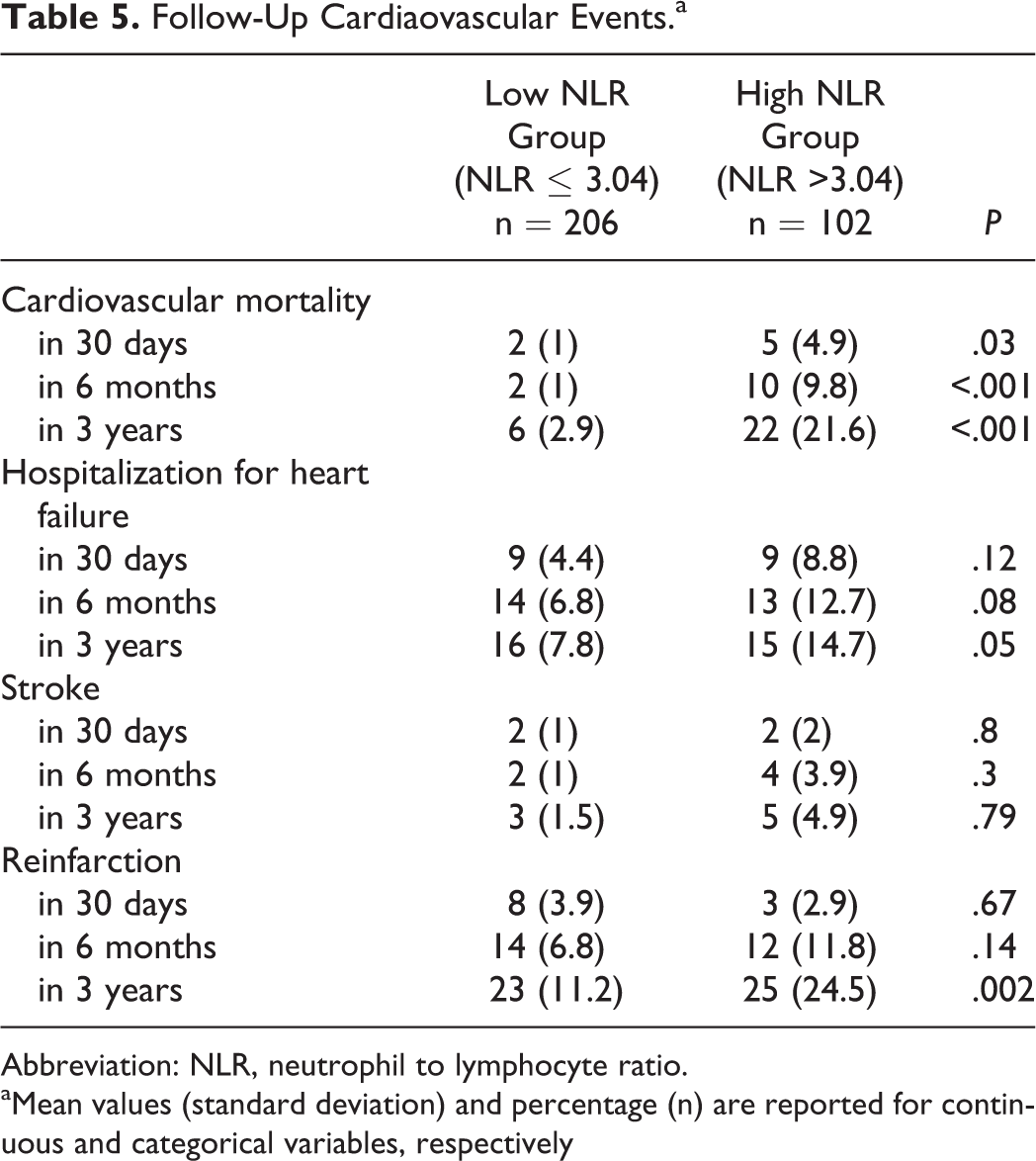
Abbreviation: NLR, neutrophil to lymphocyte ratio.
aMean values (standard deviation) and percentage (n) are reported for continuous and categorical variables, respectively
In Kaplan-Meier survival analysis, the 3-year mortality rate was 21.6% in the high-NLR group versus 3% in the low-NLR group (P < .001; Figure 1). In a receiver–operating characteristic (ROC) curve analysis, an NLR value of 3.04 identified as an effective cut point in NSTEMI and UAP of the 3-year cardiovascular mortality (AUC = 0.86, 95% confidence interval [CI] 0.8-0.92). An NLR value of >3.04 yielded a sensitivity of 79% and specificity of 71% (Figure 2).
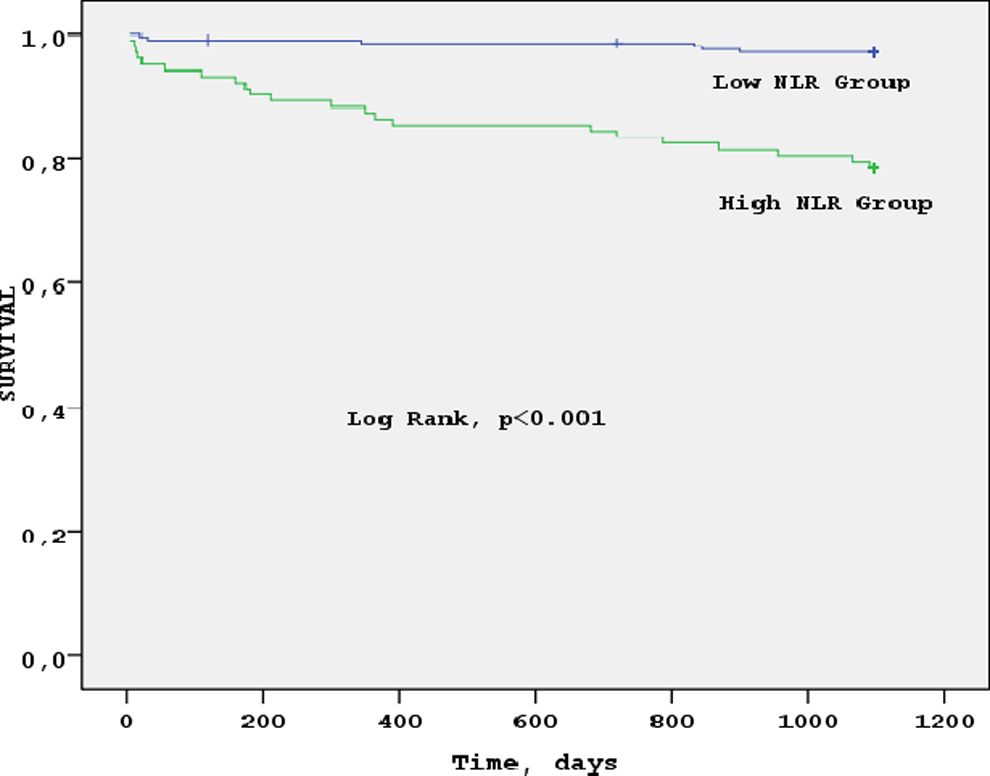
Kaplan-Meier curves for 3-year survival according to neutrophil to lymphocyte ratio. The 3-year cardiovascular mortality was 21.6% in the high neutrophil to lymphocyte ratio versus 2.9% in the low neutrophil to lymphocyte ratio.
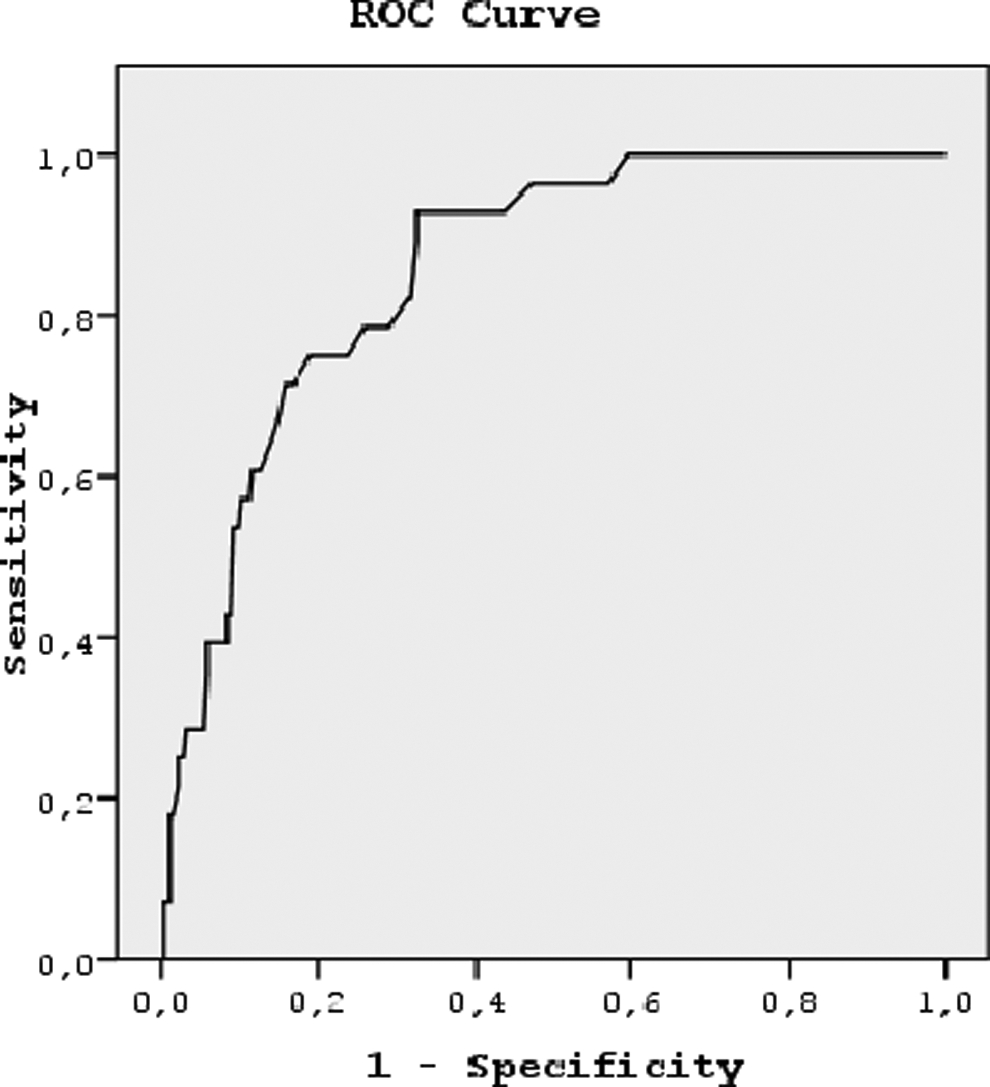
The receive–operating characteristic curve for neutrophil to lymphocyte ratio for predicting cardiovascular mortality (area under curve = 0.86, 95% confidence interval 0.80-0.92, P < .001). An neutrophil to lymphocyte ratio value of more than 3.04 demonstrated a sensitivity of 79% and a specificity of 71%.
We used Cox proportional hazard models to examine the association between NLR and adverse clinical outcomes. A significant association was noted between the high admission NLR level and the adjusted risk of cardiovascular mortality (hazard ratio [HR]: 6.3, 95% CI: 1.6-24.3, P = .008). Other independent predictors of cardiovascular mortality were determined by Cox proportional hazards analysis (Table 6).
Multivariate Predictors of Long-term Cardiovascular Mortality.a
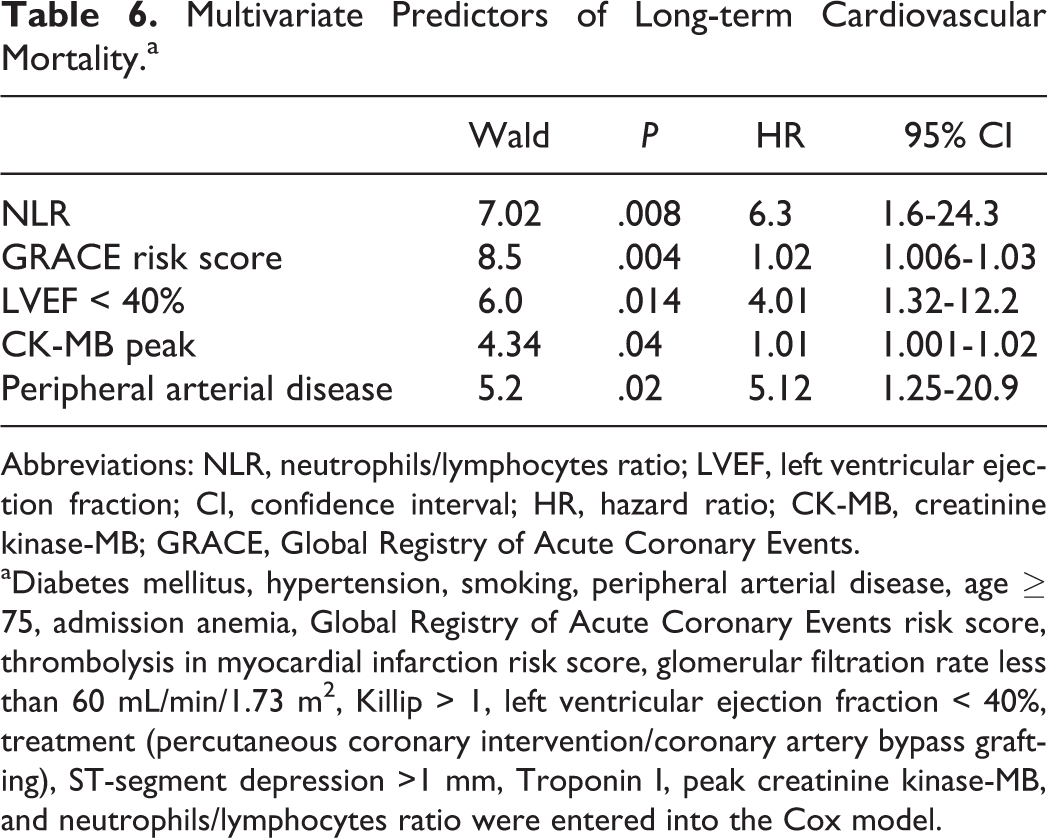
Abbreviations: NLR, neutrophils/lymphocytes ratio; LVEF, left ventricular ejection fraction; CI, confidence interval; HR, hazard ratio; CK-MB, creatinine kinase-MB; GRACE, Global Registry of Acute Coronary Events. aDiabetes mellitus, hypertension, smoking, peripheral arterial disease, age ≥ 75, admission anemia, Global Registry of Acute Coronary Events risk score, thrombolysis in myocardial infarction risk score, glomerular filtration rate less than 60 mL/min/1.73 m2, Killip > 1, left ventricular ejection fraction < 40%, treatment (percutaneous coronary intervention/coronary artery bypass grafting), ST-segment depression >1 mm, Troponin I, peak creatinine kinase-MB, and neutrophils/lymphocytes ratio were entered into the Cox model.
Discussion
The primary finding of this study is that higher NLR value is associated with increased risk for 3-year mortality in patients with NSTEMI and UAP. Additional analysis revealed that higher NLR value was associated with increased risk for a 3-year reinfarction and hospitalization for heart failure in patients with NSTEMI and UAP.
Previous studies showed that increased WBC counts were associated with short-term mortality in patients with acute MIs and increased incidence of heart failure hospitalization and mortality. 12,13 Giugliano et al showed that elevated total leukocyte count and neutrophil count predicted major cardiovascular events in peripheral arterial disease. 14 Recently, the NLR has emerged as a potent composite inflammatory marker. Duffy et al demonstrated that elevated NLR predicted long-term mortality after percutaneous coronary intervention. 15 Turak et al demonstrated that high preprocedural NLR is a powerful and independent predictor of bare-metal stent restenosis in patients with stable angina pectoris and UAP. 16 Another study with 418 patients by Akpek et al demonstrated that the NLR was independently associated with the development of no reflow and in-hospital major adverse cardiac events (MACEs) in patients with STEMI undergoing primary PCI. 17 Similarly, Nunez et al also showed NLR to be the predictor of long-term mortality in STEMI. 5 Additionally, higher NLR was shown to be the predictor of long-term mortality in patients admitted with acute decompensated heart failure. 18 Azab et al demonstrated that NLR is a predictor of short-term and long-term mortality in patients with NSTEMI. 19 Their study was a retrospective study contrary to our study and they only presented all-cause mortality rate with no secondary end point results.
The WBC count and its subtypes are classic markers of inflammation in cardiovascular diseases. 20 Activated neutrophils release a variety of proteolytic enzymes such as myeloperoxidase, elastase, acid phosphatase, and oxygen free radicals that can facilitate plaque disruption. 21 –23 Increased neutrophil count predicts adverse angiographic outcomes in patients with STEMI. In addition, neutrophils may be involved in a maladaptive process that includes vascular plugging leading to enlargement of the infarct. 24 On the other hand, low lymphocytes represent depressed immune response that is also associated with adverse outcomes in patients with acute MI and advanced heart failure. 25,26 Elevated NLR integrated the predictive risk of both increased neutrophil and decreased lymphocyte; therefore, it should be more predictive than either parameter alone.
Increased circulating levels of inflammatory markers have been observed in patients with heart failure of varying causes, suggesting that inflammatory activation is potentially linked to the pathogenesis of heart failure. 27 In our study, there was a negative correlation between the NLR and the LVEF. In addition, hospitalization for heart failure was higher at 3 years in the high-NLR group. Turkmen et al showed the relationship between NLR and inflammation patients with end stage renal disease. 30 In the present study, we noted a significant association between the lower level of GFR and the higher NLR groups. Incidence of CIN was higher in the high-NLR group compared to the low-NLR group.
Smoking may produce systemic inflammatory condition with deceptively low NLR due to increased migration of neutrophils from the intravascular compartment to the peripheral tissues due to an increase in chemotactic and adhesion molecule activities that lead to a decrease in intravascular neutrophils and lowering of NLR. 28 Similar to the previous studies, 18 we observed that smoking was higher in the low-NLR group than the high-NLR group.
In the same group of patients, we found that red cell distribution width (RDW) was associated with long-term mortality. 29 Neutrophil to lymphocyte ratio can be easily calculated from the differential WBC count. Compared to many other inflammatory markers, NLR is inexpensive and is routinely performed on admission; therefore adds no further cost. Previous studies have demonstrated the usefulness of NLR in predicting adverse outcomes in CAD; however, the NLR was not included in any risk scoring. There was a good positive correlation between the NLR levels and the TIMI risk score, GRACE risk score, CK-MB peak, troponin I, and admission glucose. Risk stratification is essential in managing the ACS, and the TIMI and GRACE risk scores are valuable tools in ACS. According to the previous studies, there was a statistical difference in mortality once NLR was >4.5-5. 4,5,15,17 In our study, in a ROC curve analysis, an NLR value of 3.04 was identified as an effective cut point in NSTEMI and UAP of 3-year cardiovascular mortality (AUC = 0.86, 95% CI 0.8-0.92). An NLR value >3.04 yielded a sensitivity of 79% and a specificity of 71%. The NLR cutoff point derived from randomized multicenter trials may be used as a prognostic indicator.
Study Limitation
Same limitations should be considered for this study. Our study is a single-center study and patients had different treatment modalities (CABG/PCI vs medical treatment). However, the NLR was significantly associated with cardiovascular mortality independent of the treatment modality. Inflammatory markers such as C-reactive protein, myeloperoxidase, tumor necrosis factor-α, and interleukin (IL)-6 were not analyzed and are not compared to NLR. However, such inflammatory biomarkers are expensive and are not immediately available in everyday practice.
Conclusion
Admission NLR is the strong and independent predictor of a 3-year cardiovascular mortality in patients with NSTEMI and UAP. Consequently, given the advantages of NLR, it may be the ideal marker for risk stratification in patients with NSTEMI and UAP.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.