
Abstract
Background/Aim:
To evaluate the value of
Methods:
A total of 137 patients with cirrhotic PHT who undergone devascularization from January 2012 to April 2014 were retrospectively reviewed, all of them were divided into 2 groups (PVT group and non-PVT group) by Doppler ultrasonography (DU) examination. The level of
Results:
In all, 38 (27.7%) patients were found to have PVT by DU examination postoperatively. In contrast to the non-PVT group, the level of
Conclusion:
The level of
Introduction
Portal vein thrombosis (PVT) includes thrombosis in the portal vein, splenic vein, and superior mesenteric vein or intrahepatic portal vein branches as they form an interactive vascular system without valves. Portal vein thrombosis following devascularization occurs in 6.3% to 39.0% of patients and is mostly an unpredictable event. 1,2 Complete or partial occlusion of the portal venous system in patients with cirrhotic portal hypertension (PHT) may determine liver ischemia, with consequent deterioration of liver function, and a sudden increase in portal pressure. Some complications of liver cirrhosis such as variceal hemorrhage may develop and death eventually may occur. 3 –5 It is therefore important to identify markers that can predict the PVT and be used to guide prevention.
Platelet count had been used to evaluate the possibility of thrombosis and make prophylactic treatment, but some studies showed that patients with increased levels of platelet count were not accompanied with thrombosis.
6
Methods
Patients and Study Design
Two hundred and sixty-seven consecutive patients who were diagnosed with hepatitis virus-related cirrhosis PHT between January 2012 and April 2014 at the 81st Hospital of P.L.A. in Nanjing, China, were included. The diagnoses of these patients were all confirmed by endoscopy, Doppler ultrasonography (DU), virological examination, biochemistry tests, and biopsy specimen of liver during the operation. All of them underwent the surgery procedure. The indications for operation were reported in our previous study.
11
All of the patients accompanied with no serious cardiopulmonary diseases and concomitant chronic duodenal ulcers. Patients whose serum levels of
Preoperative Clinical Characteristics of Patients With Cirrhosis.
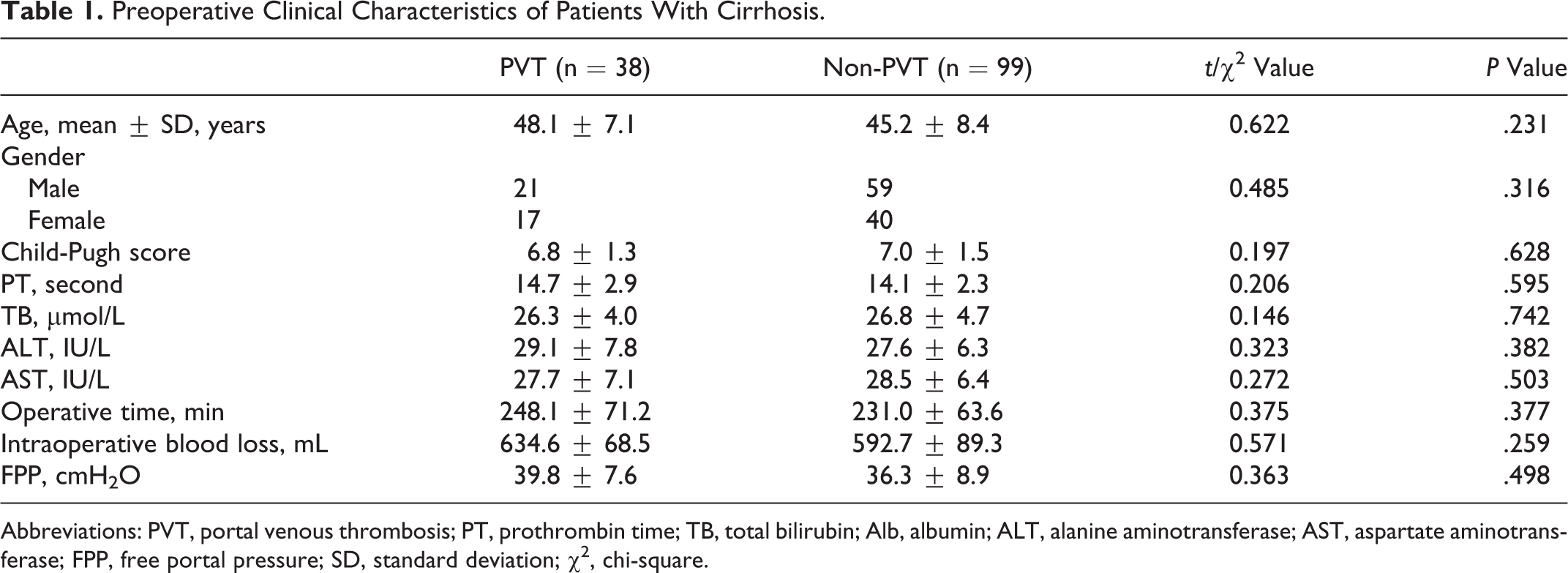
Abbreviations: PVT, portal venous thrombosis; PT, prothrombin time; TB, total bilirubin; Alb, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; FPP, free portal pressure; SD, standard deviation; χ2, chi-square.
The study protocol conformed to the guidelines by the institutional ethical committee. All patients gave their informed consent to be included in the study. The research was carried out according to the principles of The Declaration of Helsinki.
Portal Vein Thrombosis Diagnosis
The DU (ACUSON Sequoia 512, Color Doppler equipment, Germany) examination of the portal vein was performed pre-/postoperationally. 12 The study was performed in all cases by the same examiner to avoid interobserver variables. Spectral waveforms were obtained at measured angles of insonation of <60°. The preoperational examination was performed at 3 days before the surgery. The postoperational examination was performed at 2, 5, 7, 15, 22, and 30 days following the surgery. Portal vein thrombosis was defined as the obstruction of more than 50% of the vascular lumen by a thrombus in the main portal vein, its large branches, or in the splenic vein. No patient had a diagnosed PVT prior to the operation. Then the samples were divided into 2 groups, including PVT group and non-PVT group.
d -Dimer and P-Selectin Determinations
Peripheral venous blood sample (15 mL) was collected from each patient who had fasted for at least 12 hours and mixed with 3.8% sodium citrate (ratio 9:1). Sample was centrifuged for 10 minutes at 2000g, and the supernatant was stored at −80°C until use.
Surgical Technique
The surgical technique was applied as described by Zong et al. 11 The same operative setup and standardized technique were applied for all patients. Procedures were performed by the same team of specialists in gastrointestinal and hepatobiliary surgery.
Statistics Analysis
All statistical analyses were performed using SPSS15.0 software (SPSS, Chicago, Illinois). Continuous data were expressed as mean values ± standard deviations. Significant differences between groups were determined by chi-square analysis and unpaired Student t test. Dichotomous variables were created out of continuous variables by using clinically important cutoff points. Receiver–operating characteristic (ROC) curves, sensitivity (Sen), specificity (Spe), and positive and negative predictive values (PPV and NPV) were determined to assess the diagnostic value of
Results
Baseline Characteristics
The DU examination showed 38 patients developed PVT postoperatively (38 of 137, 27.7%), the occurrence of PVT was 5.72 ± 1.73 days after devascularization, and 86.8% of PVT (33 of 38) occurred between days 3 and 7.
There were no significant difference between the PVT group and the non-PVT group of the preoperative database including age, gender, Child-Pugh score, blood routine tests, biochemical tests, the level of D-dimer and P-selectin, mean operative time, intraoperative blood loss, and intraoperative freedom portal vein pressure (P > .05; Table 2). The 2 groups were well balanced in the distribution of pre- and intraoperational characteristics.
The Level of
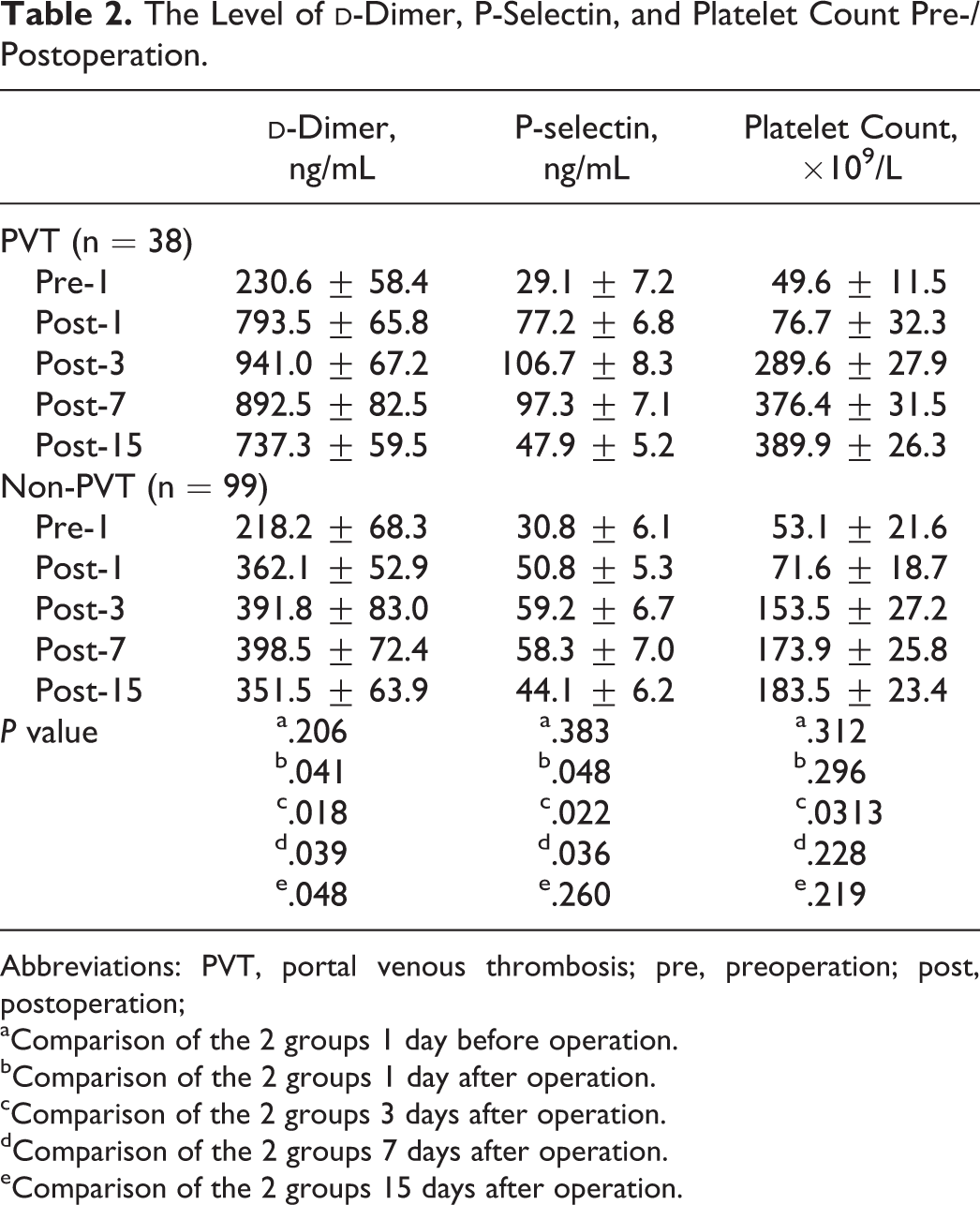
Abbreviations: PVT, portal venous thrombosis; pre, preoperation; post, postoperation;
aComparison of the 2 groups 1 day before operation.
bComparison of the 2 groups 1 day after operation.
cComparison of the 2 groups 3 days after operation.
dComparison of the 2 groups 7 days after operation.
eComparison of the 2 groups 15 days after operation.
The Level of d -Dimer, P-Selectin, and Platelet Count
As shown in Table 2 and Figures 1
to 3, in contrast to the non-PVT group, the level of
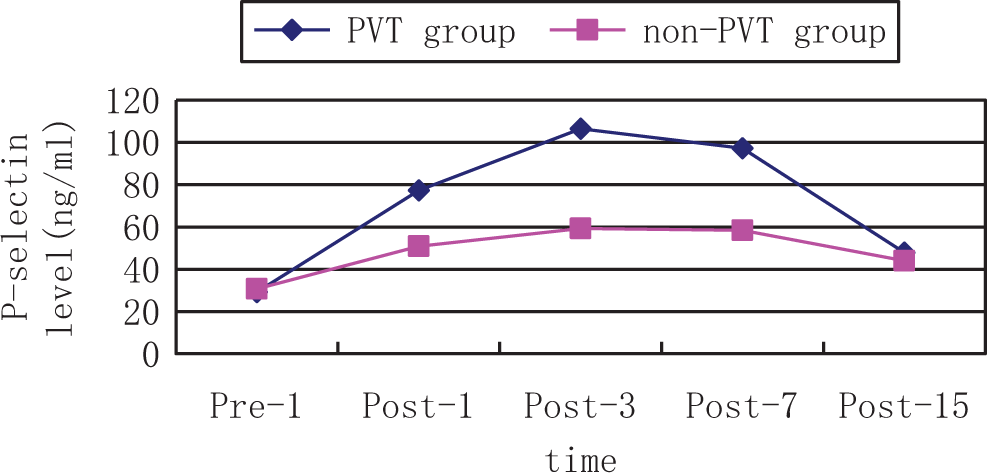
The change in P-selectin level perioperatively. PVT indicates portal venous thrombosis; Pre, preoperation; Post, postoperation.
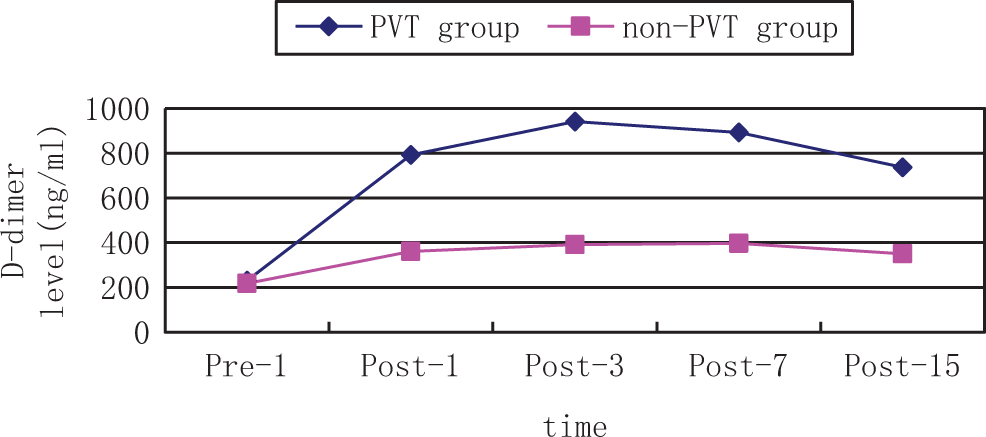
The change in
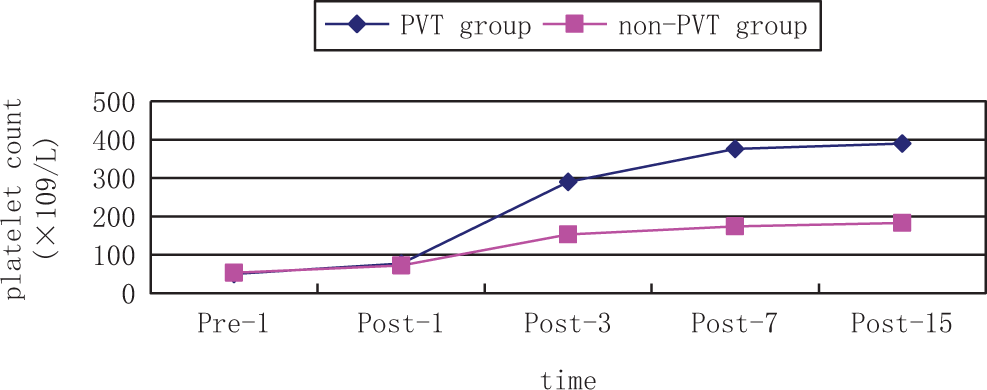
The change in platelet count perioperatively. PVT indicates portal venous thrombosis; Pre, preoperation; Post, postoperation.
Value of d -Dimer, P-Selectin, and Platelet Count on PVT
By using the change in
Evaluation of the value of
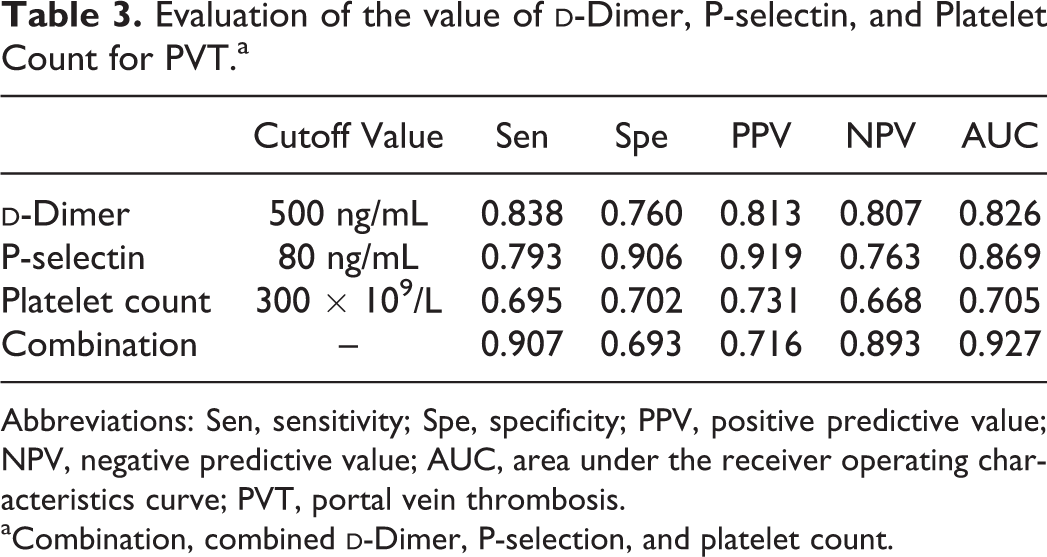
Abbreviations: Sen, sensitivity; Spe, specificity; PPV, positive predictive value; NPV, negative predictive value; AUC, area under the receiver operating characteristics curve; PVT, portal vein thrombosis.
aCombination, combined
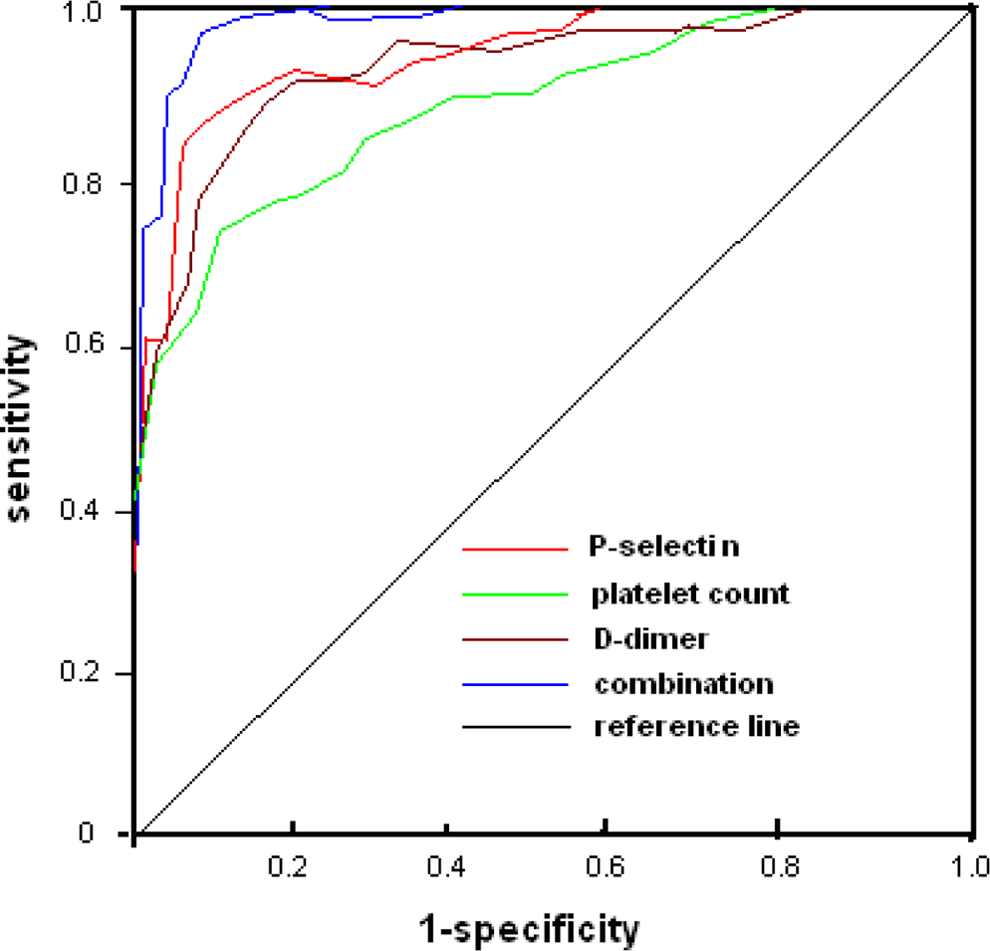
The receiver–operating characteristic (ROC) curve for diagnosis of portal venous thrombosis (PVT) by
Discussion
The prevalence of PVT in cirrhotic PHT had been reported as values ranging from 0.6% to 2.1% 13 However, PVT has been recognized as a potential complication following devascularization for PHT, some literature showed a frequency from 6.3% to 39.0% for postoperation of PVT. 1,2 In our study, the incidence of PVT after devascularization was 8.6%. Portal vein thrombosis is often an occasional diagnosis in asymptomatic patients, but it may rapidly progress leading to massive thrombosis of intestinal veins, even fatal consequences. 14 Therefore, early diagnosis of PVT may be useful to prevent uneventful outcome. The early predictive indicator of postoperative PVT may be the most focus.
At present, some methods were performed to prevent the occurrence of PVT: (1) systemic or topical injection heparin for prophylaxis intraoperatively or immediate postoperatively. 15 But not all patients may have PVT or accept the treatment of injection heparin; (2) anticoagulant therapy base on the testing platelet count, since this method reflects only the number of platelets and ignores the function of platelet count. Some reports showed that the level of platelet count was not more than the level of 500 × 109/L until PVT formation 16 ; and (3) imaging examination especially DU can provide information on the thromboses via echo analysis, detect the presence of poststenotic dilatation, as well as flow defects and turbulence. Although PVT can be accurately diagnosed by DU, the formation of thrombosis was a dynamic process, only when the appearance of PVT, the ultrasound can play a valuable role, so it can’t predict thrombosis.
The study on deep venous thrombosis showed that P-selectin involved in platelet/endothelial cell adhesion and inflammation in vascular wall, which may lead to a new pathogenesis of venous thrombosis. 21 Blenn et al found that soluble P-selectin level in patients with deep vein thrombosis was significantly higher, which may be related to excessive platelet activation. 22 Myers experiment showed that P-selectin could enlarge the effect of vein wall inflammation caused by thrombotic stimuli and promoting venous thrombosis. The higher level P-selectin, the more inflammatory cells in vein wall, the bigger intravenous clot generated simultaneously in model mice. 23 Therefore, as an indicator of the degree or function of platelet activation, P-selectin can be regarded as a marker to evaluate the prothrombotic state, coagulation tendency, and formation of thrombosis in vivo. Our study showed that compared with non-PVT group, the level of P-selectin was higher in the PVT group postoperationally, especially in 3 days after surgery. When 80 ng/mL was set as a cutoff point, P-selectin had an 87% sensitivity and specificity for PVT.
As a dynamic process, the formation of thrombosis was monitored by our DU continuously. And the 3 indicators including
Conclusion
The level of
Footnotes
Authors’ Note
Yang Fei and Guang-quan Zong are co-first author. They are equal contributors to this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.