
Abstract
Elevated lipoprotein (a) [Lp(a)] is related to the incidence of lower limb deep vein thrombosis and pulmonary embolism. Its role in portal and/or splenic vein thrombosis (PSVT) is not established. A total of 77 consecutive patients who underwent splenectomy for cirrhotic portal hypertension were prospectively studied between 2014 and 2017. The impact of Lp(a) on preoperative day 1 and postoperative days (PODs) 1, 3, 5, 7, and 14 was analyzed. Color Doppler ultrasound examination was performed for the diagnosis of PSVT. The median interval between surgery and postoperative PSVT was 6 days (range: 2-13 days). The levels of Lp(a) were highly increased in patients with PSVT and significant intergroup differences (vs non-PSVT) were found until day 3 and day 5 after operation, respectively. On POD 3, at a threshold of 309.06 mg/L, Lp(a) was a better predictor of PSVT (area under the curve [AUC] = 0.872) compared to the levels on PODs 1, 5, and 7 (AUC = 0.775, 0.796, and 0.791, respectively). The median Lp(a) values peaked at 382.5 mg/L on POD 5 for patients without PSVT. After POD 5, the Lp(a) decreased with values at 347.4 mg/L on POD 7 and 150.7 mg/L on POD 14. For the first time, Lp(a) was shown to be abnormal in patients with PSVT following splenectomy. Monitoring of serum Lp(a) levels on POD 3 might represent a valuable tool to predict early PSVT after splenectomy in cirrhotic patients.
Keywords
Introduction
Portal and/or splenic vein thrombosis (PSVT) is a common and potentially lethal complication following splenectomy.
1,2
The incidence of PSVT detected by imaging methods was 12.3% and ranged from 4.8% to 51.5%,
3,4
which was much higher in patients after splenectomy for cirrhotic portal hypertension (PHT).
5
This outcome may be due to the special pathophysiological features of cirrhotic PHT and disturbances in postoperative hemodynamics.
6
Portal and/or splenic vein thrombosis leads to liver dysfunction, increases the risk of ischemic intestinal necrosis and variceal bleeding, and even influences liver transplantation in patients with cirrhosis.
7
–9
However, the identification serum markers for PSVT prediction in patients undergoing splenectomy for cirrhotic PHT remains elusive.
Lipoprotein (a) [Lp(a)] is a circulating macromolecule consisting of a low-density lipoprotein particle that is covalently linked to apolipoprotein (a). 13 As Lp(a) has strong structural homology to plasminogen and thus possibly inhibits fibrinolysis, high concentrations of Lp(a) may promote thrombosis. 14,15 Numerous case–control and prospective studies indicated that there was an apparent association between circulating Lp(a) levels and thrombotic events. 16 –18 Marcucci et al 19 found that Lp(a) was independently associated with occurrence of venous thromboembolism (VTE) in adult patients, suggesting the importance of serum Lp(a) in idiopathic and recurrent VTE. An Lp(a) level greater than 300 mg/L was correlated with a more than 10-fold increased risk of VTE in patients with spinal cord injury. 20 Although most evidence suggests that Lp(a) is an independent risk factor of VTE, 21,22 little is known about the role of Lp(a) in PSVT after splenectomy, which was a very strong risk factor for the development of portal venous system thrombosis in cirrhotic patients. 23 We aimed to investigate the changes of serum Lp(a) in cirrhotic patients with splenectomy and explore its value in PSVT prediction.
Methods
Study Population
The present study was performed at the Shanxi Bethune Hospital (a tertiary hospital), Shanxi Province, China, and approved by the local medical ethical committee. Between December 2013 and December 2017, we recruited patients diagnosed with cirrhotic PHT who underwent either splenectomy alone or in combination with devascularization. The primary indications for splenectomy included endoscopic treatment-resistant esophageal varices with or without variceal hemorrhage, a tendency to bleeding and infection due to hypersplenism and general conditions satisfying the needs for operation. All participants gave informed consent before entering this study. Exclusion criteria were as follows: (1) age of >75 years or <18 years; (2) any baseline prothrombotic risk factors, such as severe coagulation disorders, congenital thrombotic disease, or preoperative PSVT and deep vein thrombosis; (3) a lack of typical manifestations of PHT; and (4) the presence of other chronic illnesses, such as cardiovascular, respiratory, or renal diseases. Patients were withdrawn from this study if diagnosed with PSVT (Figure 1A).
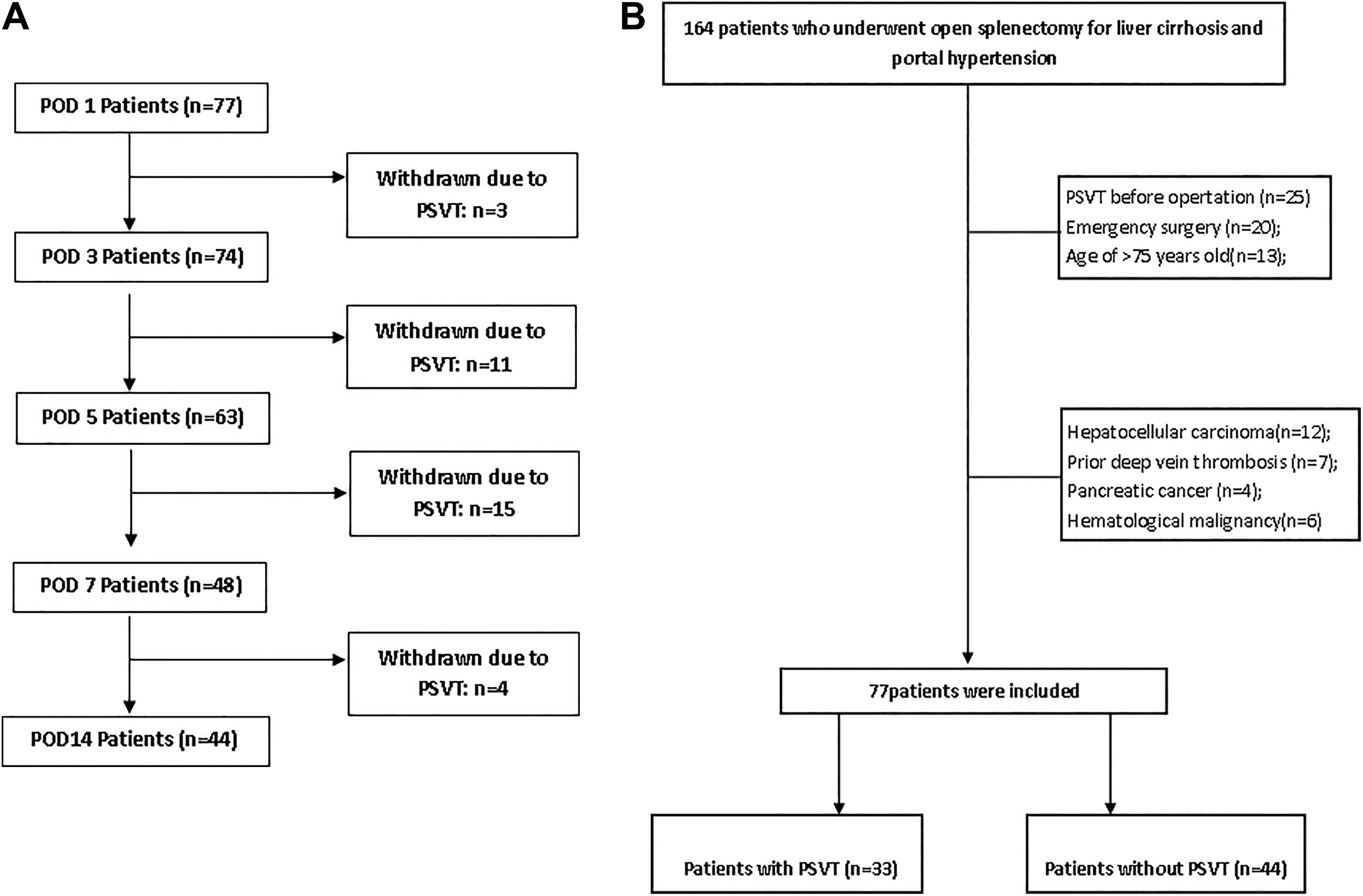
Flowchart of (A) withdrawal and (B) recruitment. POD indicates postoperative day.
Surgical methods
All patients underwent conventional open splenectomy and all operations were elective. After general anesthesia, all patients were placed in a supine position and an L-shaped incision of the upper left abdomen was made. The devascularization was implemented after the splenectomy. All procedures were performed by the same surgical team.
Diagnosis of PSVT
Color Doppler (Mylab70, Esaote, Maastricht, the Netherlands) examination was performed to detect portal diameter, blood flow, and PSVT formation at 11
Lipoprotein (a) Assays
Venous blood was sampled on preoperative day 1 and postoperative days (PODs) 1, 3, 5, 7, and 14 for the measurement of Lp(a). All venipunctures were performed at 8
Statistical Analyses
Data were analyzed using the SPSS software package, versions 22.0 (SPSS Inc, Chicago, Illinois) and GraphPad Prism, version 6.0 (GraphPad Software Inc, La Jolla, California). Student t test, χ2 test, nonparametric Mann-Whitney U test, and Spearman test were applied as appropriate. Because Lp(a) values are skewed, we used logarithmic transformation to obtain a normal distribution and more reliable estimates for comparative analysis among groups and regression analyses. Areas under the curve (AUCs) of receiver operating characteristic were determined and optimal cutoff values for serum Lp(a) levels for predicting PSVT were evaluated. The optimal serum Lp(a) cutoff values were defined as the value that provided the highest sensitivity and specificity for predicting PSVT. To determine the risk of postoperative PSVT, odds ratios were calculated by logistic regression analysis with 95% confidence intervals. A value of P < .05 was considered statistically significant.
Results
Baseline Characteristics
A total of 77 eligible patients were recruited and the demographic characteristics of all patients are listed in Table 1 and Figure 1B. Thirty-three (42.9%) patients were diagnosed with PSVT, and the median interval between surgery and postoperative PSVT was 6 days (range: 2-13 days). There were 6 patients with symptomatic PSVT in our study and all symptomatic patients were present with fever or/and abdominal pain. Indications for operation included endoscopic treatment-resistant esophageal varices (n = 26), bleeding tendency (n = 21), infection tendency (n = 19), and other conditions (n = 11). The mean postoperative hospital stay was 21.7 ± 6.9 days and no patient died after the operation. There were no significant differences between the patients with PSVT and those without PSVT of the preoperative data, including age, sex, body mass index, surgical procedures, Child-Pugh score, 24 and hematologic findings (P > .05; Table 1). Simple splenectomy was conducted in 30 patients, and splenectomy plus devascularization was performed in 47 patients. Moreover, the incidence rate of PSVT was higher in patients with splenectomy and devascularization than those with splenectomy alone, although this did not reach statistical significance.
Baseline Characteristics of Patients.a

Abbreviations: HDL, high-density lipoprotein; IQR, interquartile range; LDL, low-density lipoprotein; PLT, platelet counts; PVST, portal and/or splenic vein thrombosis; S+D, splenectomy + devascularization; TC, total cholesterol; TG, triglyceride; WBC, white blood cell.
a Values are expressed as mean ± standard deviation unless otherwise indicated.
Lipoprotein (a) Levels
The levels of Lp(a) are presented in Table 2 and the time course of postoperative Lp(a) levels are illustrated graphically in Figure 2. The levels of Lp(a) increased in patients with PSVT and significant intergroup differences (vs non-PSVT) were found until day 3 and day 5 after operation, respectively. Although the difference between the 2 groups on POD 7 was also statistically significant, due to the large difference in sample size between the 2 groups, the test efficiency may be reduced, so we should be careful when interpreting the results on POD 7. The median Lp(a) values peaked at 382.5 mg/L on POD 5 for patients without PSVT. After day 5, the Lp(a) decreased with values at 347.4 mg/L on POD 7 and 150.7 mg/L on POD14.
Comparison of Lp(a) Between Patients With and Without PSVT at Different Time Points.a

Abbreviations: Lp(a), lipoprotein (a); IQR, interquartile range; POD, postoperative day; PSVT, portal and/or splenic vein thrombosis.
a Results are expressed as median (interquartile range).

The kinetics of pre- and postoperative lipoprotein (a) values. The median values are plotted over time for patients without portal and/or splenic vein thrombosis after surgery (n = 44). −1 indicates preoperative day 1; 1, postoperative day 1; 3, postoperative day 3; 5, postoperative day 5; 7, postoperative day 7; and 14, postoperative day 14.
Value of Lp(a) Level on PSVT Prediction
A logistic regression analysis was performed to assess the association of factors and PSVT adjusted for main confounding variables such as the patients’ backgrounds and types of splenectomy. The Lp(a) level on POD 3 was included in a multivariate logistic regression model with other variables. As presented in Table 3, the POD 3 Lp(a) level was the only independent risk factor for postoperative PSVT after splenectomy (P < .0001; odds ratio, 10.35 [95% confidence interval, 3.19-50.95]; Table 4).
Areas Under the Curve Based on Every-Other-Day Values of Lipoprotein (a).
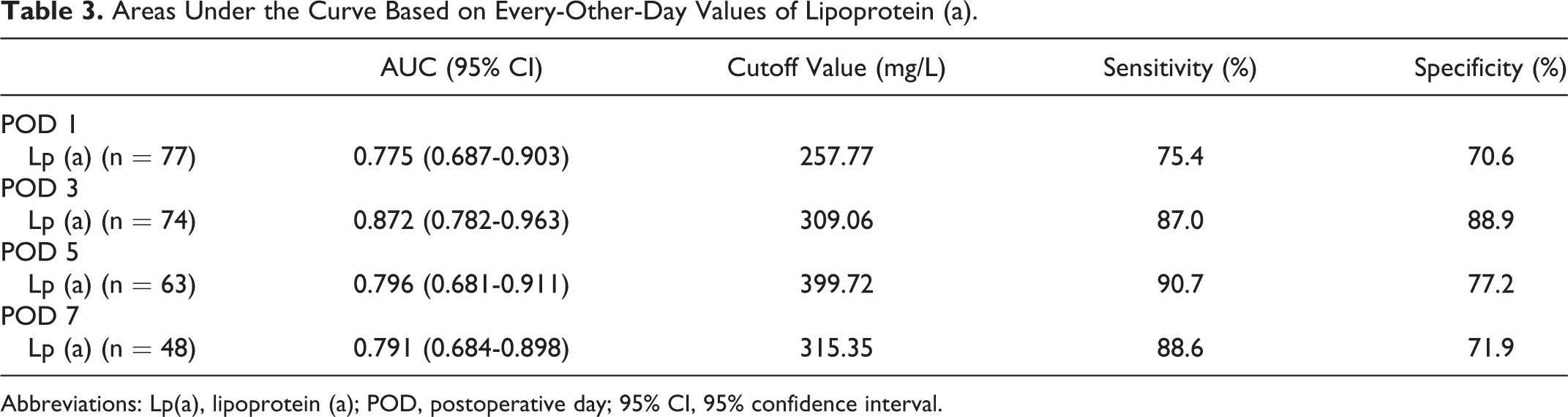
Abbreviations: Lp(a), lipoprotein (a); POD, postoperative day; 95% CI, 95% confidence interval.
Predictive Factors of PSVT After Splenectomy.
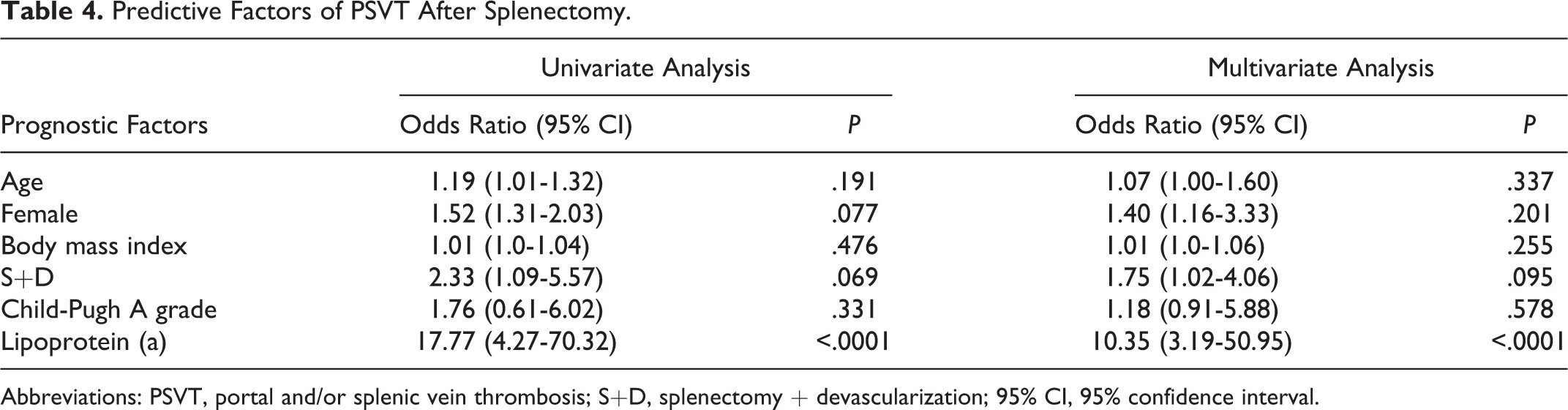
Abbreviations: PSVT, portal and/or splenic vein thrombosis; S+D, splenectomy + devascularization; 95% CI, 95% confidence interval.
Comparison Between Diagnostic Ability of Serum Lp(a) for PSVT at Various Time Points After Surgery
The AUCs were compared using the every-other-day values of Lp(a) and POD 3 serum Lp(a) was the best predictor of PSVT (Table 3 and Figure 3): AUC = 0.872, sensitivity 87.0%, and specificity 88.9% at a cutoff value of 309.06 mg/L.

Receiver operating characteristic curves of the lipoprotein (a) levels for the diagnosis of postoperative portal or splenic vein thrombosis after splenectomy in 77 patients on postoperative day (POD) 1, 73 patients on POD 3, 68 patients on POD 5, and 48 patients on POD 7.
Discussion
In the present study, we demonstrated for the first time that Lp(a) is useful for early prediction of postoperative PSVT in cirrhotic patients. Our study indicates that postoperative Lp(a) measurement on day 3 after surgery is strong predictor of postoperative PSVT. Furthermore, we have demonstrated that after operation, patients with PSVT have higher Lp(a) levels compared to those without PSVT.
Lipoprotein (a) can potentiate thrombosis as a consequence of the apolipoprotein (a), which is structurally similar to plasminogen and tissue plasminogen activator. Furthermore, Lp(a) has been shown to upregulate plasminogen activator inhibitor 1 in patients with multiple sclerosis. 25 As illustrated earlier, Lp(a) contributed to thrombotic disorders, such as deep vein thrombosis, cerebral venous sinus thrombosis, and pulmonary embolism. Our study extends the previous findings on the role of serum Lp(a), suggesting its contribution to PSVT in patients who underwent laparoscopic splenectomy for cirrhotic PHT. In addition, the concentrations of serum Lp(a) were significantly higher after surgery than before in patients with PSVT, which demonstrated that although Lp(a) concentrations are primarily genetically determined, they are not “fixed” to a certain level in given population 26,27 and some pathological conditions might influence synthesis and/or catabolism of Lp(a). 28 –30
The incidence of PSVT ranges from 20% to 96.1% in patients following splenectomy. 31,32 In the present study, the incidence rate of PSVT was 42.9%, which confirmed previous observations made in a group of 144 patients. 31 Portal and/or splenic vein thrombosis may rapidly progress and lead to intestinal vein thrombosis, and even fatal outcomes. Thus, more sensitive indicators are required to predict PSVT occurrence in order to employ more effective prevention and treatment strategies. Here, we evaluated the changes in serum Lp(a) in patients with cirrhotic PHT and its value in predicting PSVT formation. Lipoprotein (a) had an 87.0% sensitivity and 88.9% specificity for PSVT when a level of 309.06 mg/L was used as a cutoff value.
There are some limitations of this study. First, data have been collected from a single center with a limited number of cirrhotic patients. Second, we did not measure genetic polymorphisms of Lp(a) gene and its effects on association between Lp(a) levels and PSVT. Third, lack of internal or external validation of the results was also a disadvantage of our study. Finally, PSVT may occur following splenectomy for the management of PHT, splenic abscess, pancreatic cancer, gastric cancer, and idiopathic thrombocytopenic purpura. 33 The current study only enrolled patients with PHT-related splenectomy. Therefore, whether the diagnostic value of Lp(a) may also apply to patients undergoing splenectomy for other conditions requires further investigation. A forthcoming validation study for Lp(a) as a PSVT marker is being performed by analyzing a significantly large number of splenectomized patients for cirrhotic PHT during the time period from March 1, 2020, to December 31, 2022, across all Shanxi Bethune hospital.
In conclusion, this prospective study has demonstrated that there was a significant elevation in Lp(a) concentrations in patients having postoperative PSVT. Serum Lp(a) can be used to screen or diagnose PSVT following splenectomy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.