
Abstract
We measured levels of matrix metalloproteinase 9 (MMP-9) as a potential risk factor in 75 patients with acute coronary syndrome (ACS) compared to 25 patients with stable angina (SA) and 20 healthy participants. Patients were studied stressing on smoking, hypertension, diabetes, lipid profile, cardiac enzymes, MMP-9, and electrocardiography. Patients with ACS had higher MMP-9 levels than the SA group. The highest MMP-9 levels were found among ST-elevated myocardial infarction (MI), while the lowest levels were found among the control group. The MMP-9 level was significantly higher among patients with ACS having poor disease outcome (recurrent ischemic attacks, congestive heart failure, or death). The MMP-9 cutoff value of 3100 pg/mL was able to discriminate MI from unstable angina (UA), while the best prognostic utility was established at 4700 pg/mL. We suggest that serum MMP-9 could be an early marker that discriminates MI from UA and predicts poor outcome in terms of disease severity and extent of disease complications.
Introduction
Coronary heart disease (CHD) is a leading cause for morbidity and mortality in developed countries but third to AIDS and lower respiratory infections in developing countries. 1 By the year 2020, cardiovascular disease will cause an estimated 25 million deaths worldwide, becoming the predominant cause of death in the world, surpassing infectious diseases. 2
Rupture of atherosclerotic plaque with superimposed thrombosis is now considered to be the main cause of the acute coronary syndrome (ACS) that covers the spectrum of clinical conditions ranging from unstable angina (UA), non-ST-segment elevated myocardial infarction (NSTEMI), and ST-segment elevated myocardial infarction (STEMI). 3,4 Several pathophysiologic mechanisms are involved in the process of plaque rupture, including inflammation, circumferential wall stress, and vasoconstriction as well as destabilizing changes in the plaque tissue. 5 Atherosclerosis contributes to significant narrowing of the artery lumen and a tendency for plaque disruption and thrombus formation. 6
Matrix metalloproteinases (MMPs) are a family of extracellular matrix degrading enzymes that take part in biological processes, such as ontogenesis (morphogenesis, angiogenesis, growth, and wound healing) and regulation of platelet function. 7 However, the dysregulation or activation of MMPs expression is a feature of numerous pathologic conditions. 8 The MMPs are consistently implicated in atherogenesis and have a role in plaque destabilization, the most common mechanism responsible for ACS, based on contribution to tissue proteolysis as an essential factor responsible for thinning and rupturing of astherosclerotic fibrous cap. 9,10 The MMPs are expressed by macrophages, vascular smooth muscle cells, and endothelial cells in response to inflammatory stimuli and oxidative stress, all of which are involved in cardiovascular diseases. 11
Previous studies have provided evidence that MMP-9 reflects atherosclerotic plaque rupture or vulnerability. 12,13 In some prior similar studies, the diagnostic values of MMPs in patients with ACS have been studied and they showed that MMP-9 levels had a diagnostic value for early ACS. 14 However, there is still a way to go to reach the goal of precise and early identification of ACS with highest risk of detrimental outcome, which was not yet investigated in depth. When possible the right patient will receive the right treatment in the right time. The aim of this study was to assess the early level of MMP-9 in relation to patients’ characteristics as a diagnostic marker discriminating ACS from stable angina (SA) and to evaluate its value as a predictor of future risk of cardiovascular complications and disease outcome.
Materials and Methods
This study was conducted on 120 patients, 75 patients with ACS admitted to the coronary care unit, 25 patients with SA recruited from the outpatient clinic, and 20 apparently age- and sex-matched healthy participants as a control group, in the period from December 2012 to May 2013 at Ain Shams University Hospitals. Patients with malignancy, infectious disease, autoimmune disease, thyroid disease, liver disease, renal diseases, or any surgical procedure in the preceding 6 months were excluded. The study protocol was approved by Ain Shams medical research ethical committee.
Group Classification
The ACS group included 75 patients, 50 males and 25 females with a male to female ratio 2:1. Their ages ranged from 37 to 95 years with a mean of 57 ± 10.3 years. Diagnosis of ACS was based on a careful review for signs and symptoms of cardiac ischemia and electrocardiogram (ECG) findings at presentation. Accordingly, patients with ACS were subdivided into 2 major categories; those with new ST-segment elevation were diagnosed as STEMI and those who presented with ST-segment depression, T-wave changes, or no ECG abnormalities were diagnosed as NSTE ACS, encompassing both UA and NSTEMI that were differentiated clinically by the detection of elevated biomarkers of myocardial injury in case of NSTEMI. 15
The SA group included 15 males and 10 females with a male to female ratio of 1.5:1 and a mean age of 55.2 ± 11.1 years (range, 40-90 years). They were characterized clinically by the presence of ischemic chest pain, typically elicited by exertion or emotional stress and relieved by rest or nitroglycerin. Myocardial ischemia was detected by ECG stress testing. 16 The healthy control group consisted of 13 males and 7 females (ratio 1.8:1) and their ages ranged from 40 to 62 years with a mean of 52.4 ± 6.7 years.
Initial Assessment
All patients were subjected to full detailed history and careful clinical examination laying stress on risk factors, including smoking, diabetes, hypertension, family history, and previous similar attacks with calculation of body mass index (BMI), ECG, echocardiography, and coronary angiography. Routine biochemical laboratory investigations included fasting blood glucose (FBG), serum cholesterol, triglycerides, high-density lipoprotein, and low-density lipoprotein (LDL) performed on Synchron CX-9 (Beckman Coulter, California). Cardiac biomarkers were measured, total creatine kinase (CK), creatine kinase myocardial fraction (CK-MB), lactate dehydrogenase (LDH) using Synchron CX-9 (Beckman Coulter) and cardiac troponin T (cTnT) using AxSYM analyzer (Abbott Laboratories, Abbott Park, Illinois). Assessment of serum level of MMP-9 was done by enzyme-linked immunosorbent assay kit using the RayBio Human MMP-9 ELISA kit (RayBiotech, Norcross, Georgia) which employs a quantitative sandwich enzyme immunoassay technique for measurement of MMP-9. It incorporates a biotinylated antihuman MMP-9 antibody and conjugated streptavidin. The minimum detectable dose of MMP-9 was 10 pg/mL. The intra-assay reproducibility of the test showed a coefficient of variation less than 10%, and the interassay reproducibility showed a coefficient of variation less than 12%.
Sample Collection
Venous blood samples were collected, and under complete aseptic precautions, the samples were dispensed into a plain test tube without anticoagulant. After clotting, the samples were centrifuged at 1500g for 15 minutes; the separated serum was used to perform chemical analysis. Samples for measurement of MMP-9 were collected immediately after hospitalization from patients for whom the symptom complex was consistent with ACS till diagnosis was established (mainly within the first 4 hours from the start of chest pain) and the serum was stored at –20ºC in duplicates until analysis. Overnight fasting blood samples were obtained to perform FBG and lipid profile.
Follow-Up
The patients were followed up clinically for 6 months and according to their clinical outcome and ACS complications, they were divided into the following 2 groups:
Group 1 (patients with good disease outcome) included 47 (62.7%) patients defined as patients without cardiovascular complications and being in stable state.
Group 2 (patients with poor disease outcome) included 28 (37.3%) patients who developed cardiovascular events including recurrent ischemic attacks, congestive heart failure, or sudden death.
Statistical Analysis
Analysis of data was done by IBM computer using SPSS version 15 (SPSS Inc, Chicago, Illinois); quantitative data were described in the form of a mean, standard deviation, median, and range, while qualitative data were described as number and percentage. Student t test was applied to compare quantitative parametric data between the 2 groups. Quantitative nonparametric data between the 2 groups were compared using Mann-Whitney U test, while Kruskal-Wallis test was used for comparisons between more than 2 groups. The chi-square (χ2) test was used to compare qualitative data. Spearman correlation was used to assess the linear relationship between variables, and receiver–operating characteristic (ROC) curve analysis was employed for the determination of the performance characteristics of MMP-9 measurement. P value of <.05 was considered statistically significant in all analyses.
Results
Clinical and Laboratory Characteristics of Patients With ACS, Patients With SA, and Healthy Controls
Patients with ACS had a significantly higher BMI, higher mean heart rate, and higher LDL compared to patients with SA or healthy controls (P < .05). The incidence of smoking was significantly higher among ACS group than healthy controls (P = .04), while the incidence of hypertension was elevated among patients with ACS than SA group (Table 1).
Comparison of Patients With ACS, Patients With SA, and Healthy Control Participants as Regards Clinical and Laboratory Data.a
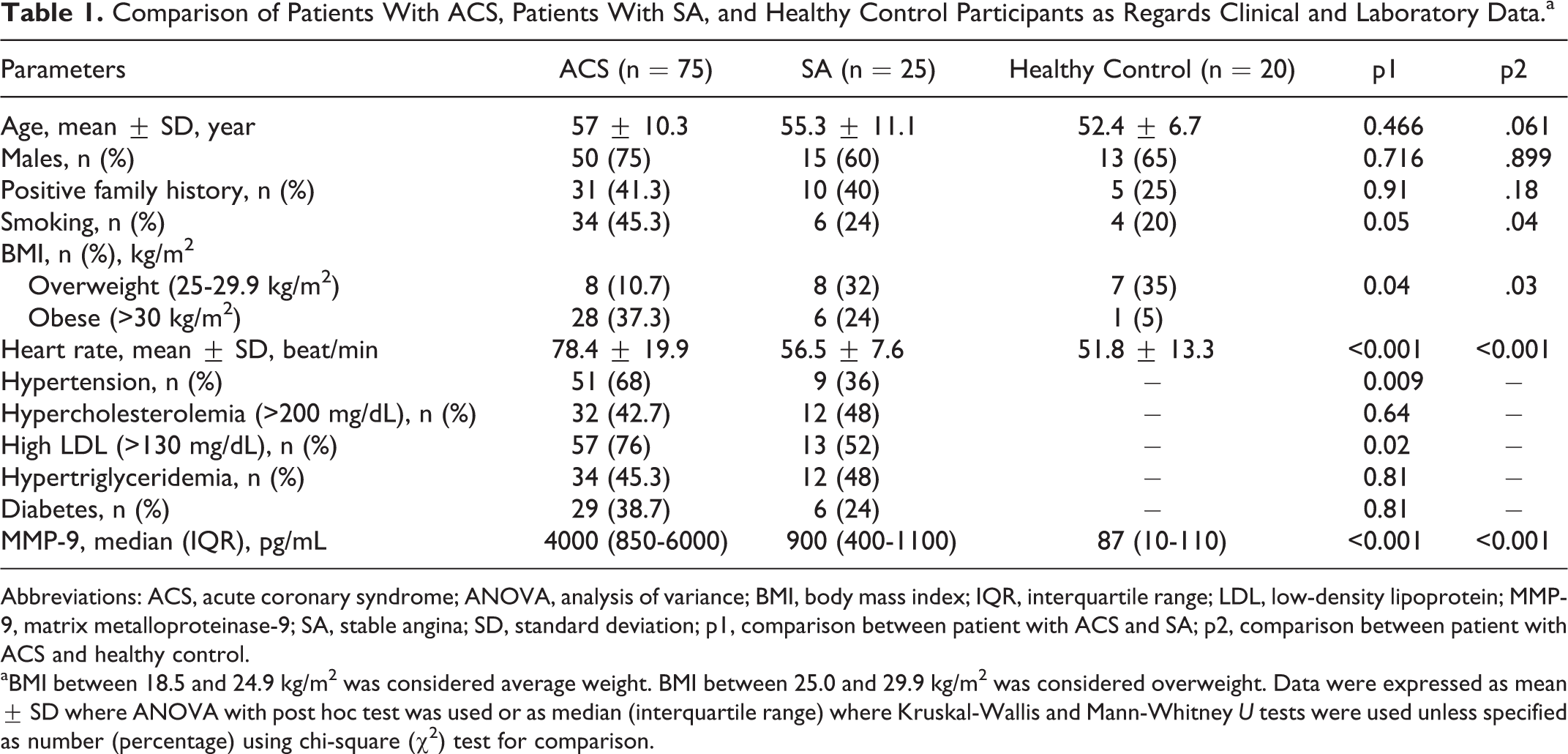
Abbreviations: ACS, acute coronary syndrome; ANOVA, analysis of variance; BMI, body mass index; IQR, interquartile range; LDL, low-density lipoprotein; MMP-9, matrix metalloproteinase-9; SA, stable angina; SD, standard deviation; p1, comparison between patient with ACS and SA; p2, comparison between patient with ACS and healthy control.
aBMI between 18.5 and 24.9 kg/m2 was considered average weight. BMI between 25.0 and 29.9 kg/m2 was considered overweight. Data were expressed as mean ± SD where ANOVA with post hoc test was used or as median (interquartile range) where Kruskal-Wallis and Mann-Whitney U tests were used unless specified as number (percentage) using chi-square (χ2) test for comparison.
Comparison Between Patients’ Subgroups as Regards Clinical and Laboratory Data
As shown in Table 2, patients with ACS having NSTEMI had the highest incidence of hypercholesterolemia (68%), hypertriglyceridemia (76%), and high LDL (84%) compared to those with UA or STEMI (P = .01), while the incidence of hypertension was significantly higher among patients with UA (P = .02). Patients with STEMI showed poorer disease outcome as denoted by the higher incidence of recurrence of ischemic attacks, congestive heart failure, or sudden death compared to UA and NSTEMI group (P <.01).
Clinical and Laboratory Data Among Different Patients’ Subgroups With Acute Coronary Syndrome.a
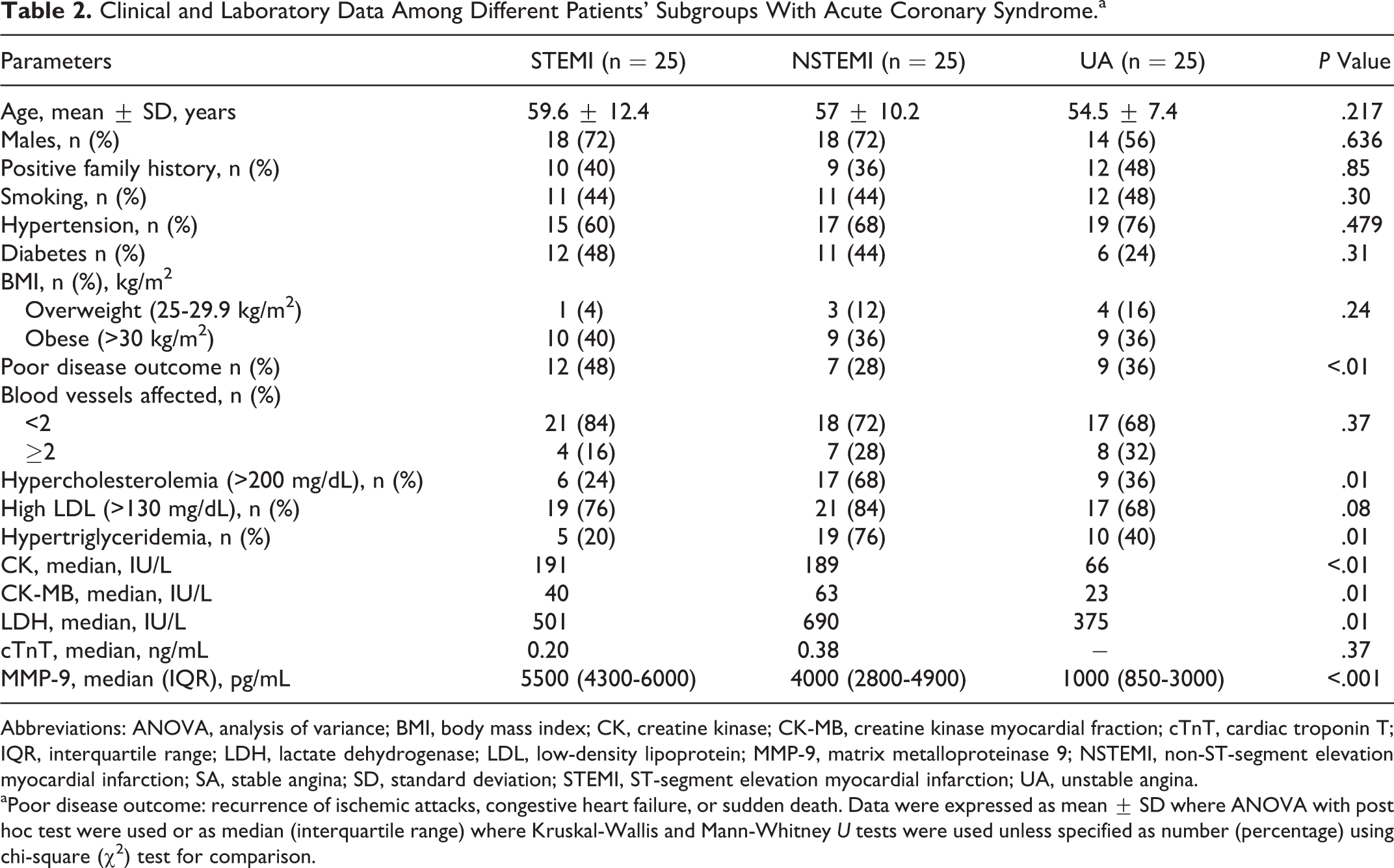
Abbreviations: ANOVA, analysis of variance; BMI, body mass index; CK, creatine kinase; CK-MB, creatine kinase myocardial fraction; cTnT, cardiac troponin T; IQR, interquartile range; LDH, lactate dehydrogenase; LDL, low-density lipoprotein; MMP-9, matrix metalloproteinase 9; NSTEMI, non-ST-segment elevation myocardial infarction; SA, stable angina; SD, standard deviation; STEMI, ST-segment elevation myocardial infarction; UA, unstable angina.
aPoor disease outcome: recurrence of ischemic attacks, congestive heart failure, or sudden death. Data were expressed as mean ± SD where ANOVA with post hoc test were used or as median (interquartile range) where Kruskal-Wallis and Mann-Whitney U tests were used unless specified as number (percentage) using chi-square (χ2) test for comparison.
As regards cardiac enzymes, total CK was significantly higher among STEMI group (P < .01), while CK-MB and LDH were higher among NSTEMI than the other 2 groups (P = .01; Table 2).
Levels of MMP-9 Among Patients With ACS and Controls
Levels of MMP-9 were significantly elevated among all patients with ACS compared to healthy controls or those with SA (P < .01; Table 1). The highest levels were found among STEMI (median 5500 pg/mL) followed by NSTEMI (median 4000 pg/mL) then UA (median 1000 pg/mL; P < .01; Table 2). It is worth to note that MMP-9 levels were also significantly elevated among all subgroups with ACS compared to patients with SA or healthy control group (Figure 1). Significant positive correlations were found between MMP-9 and heart rate (r = .26, P = .02) as well as markers of myocardial necrosis, CK (r = .3, P < .01) and LDH (r = .39, P = .01; Figure 2).
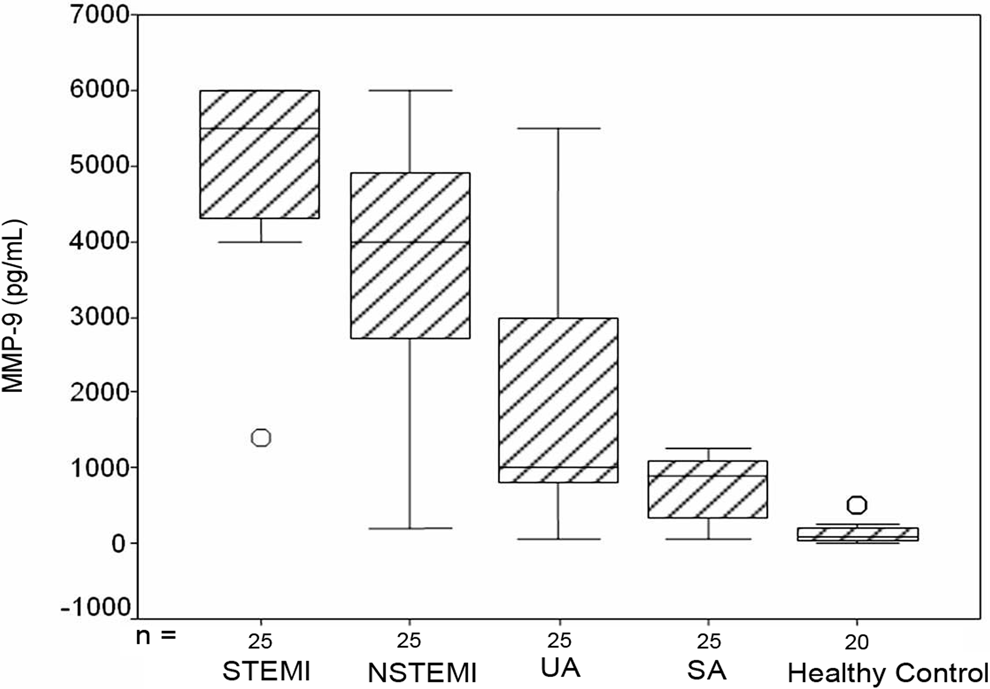
Levels of metalloproteinase 9 (MMP-9) among patients with acute coronary syndrome, stable angina, and healthy controls.
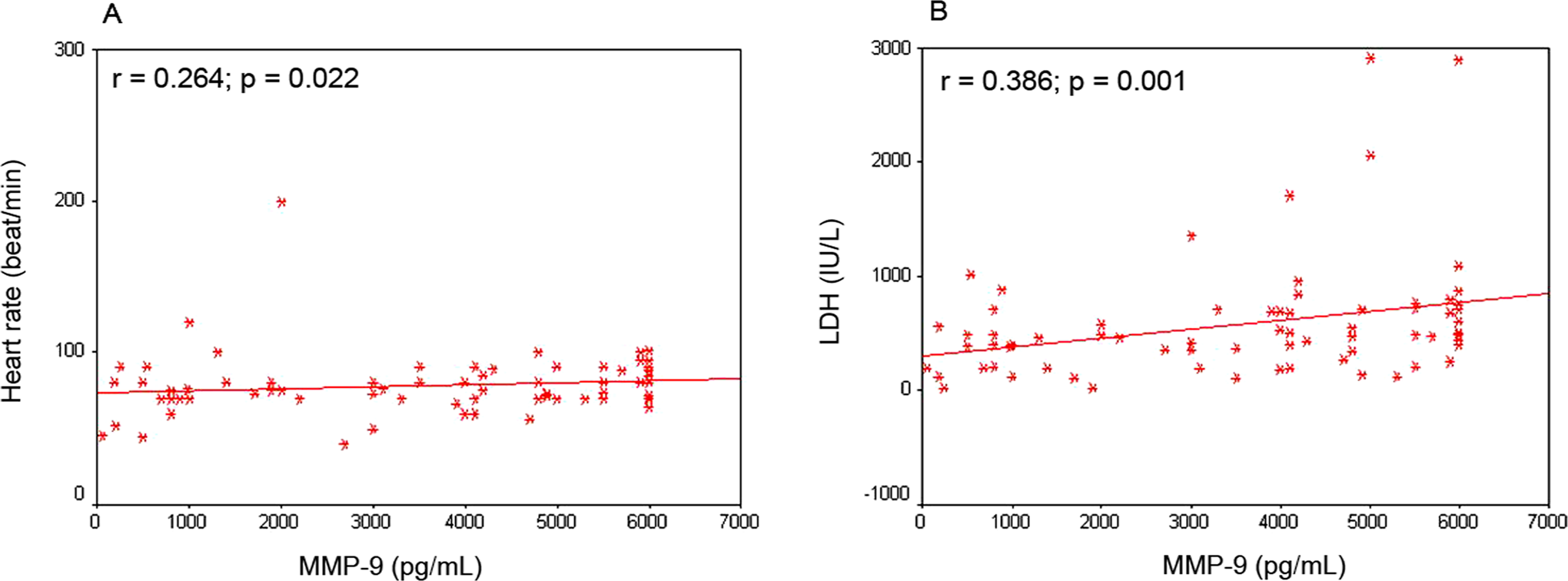
Significant positive correlations between metalloproteinase-9 (MMP-9) and heart rate (A) and lactate dehydrogenase (B) among patients with acute coronary syndrome.
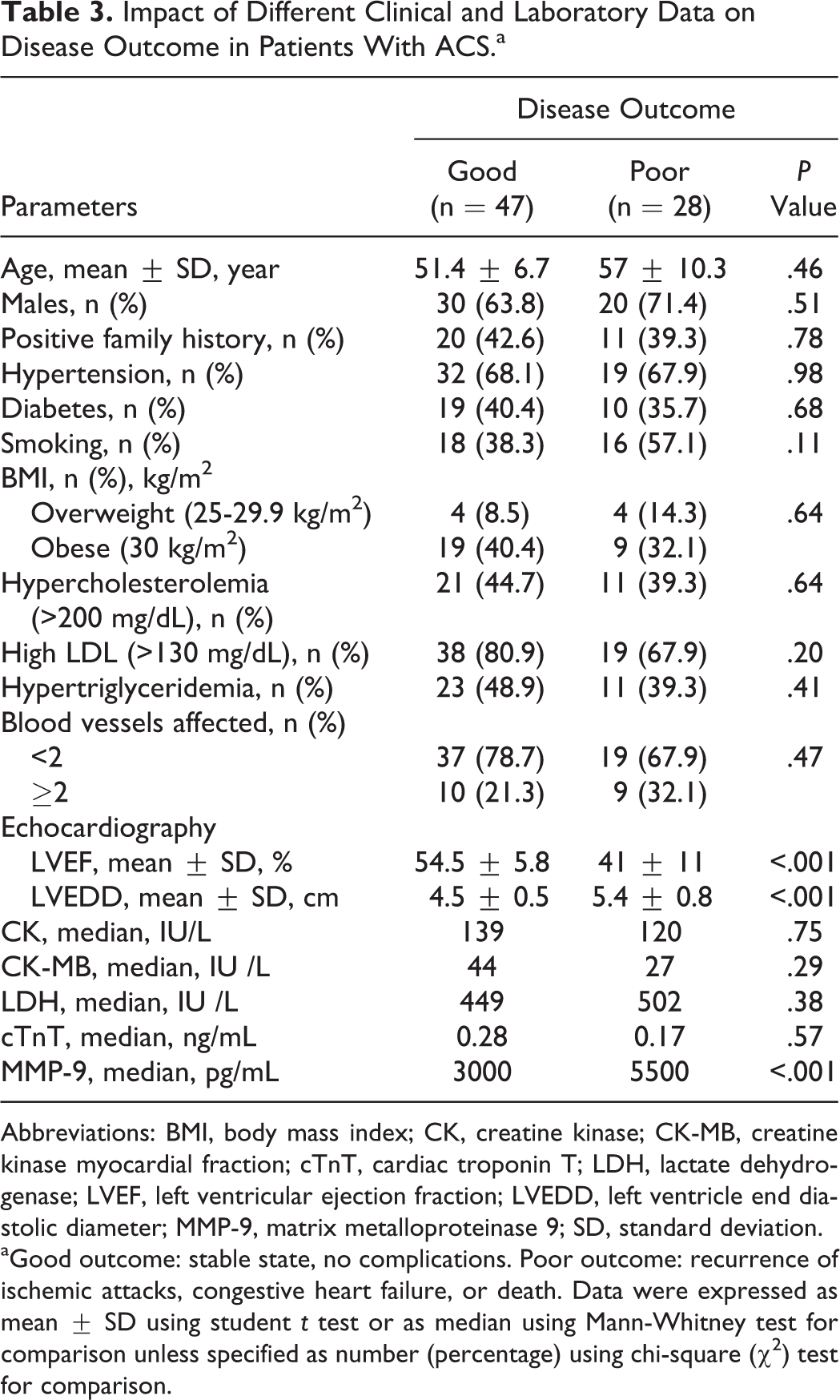
During the 6-month follow-up period, a total of 28 adverse cardiovascular events (recurrence of ischemic attack, congestive heart failure, or death due to cardiac causes) were identified, including 13 (17.3%) revascularization events (repeat percutaneous coronary artery intervention or coronary artery bypass surgery). The 28 (37.3%) patients with ACS having poor disease outcome had increased early MMP-9 levels compared to those who had better prognosis (median 5500 vs 3000 pg/mL; P < .001), while cardiac enzymes were comparable among both groups. Echocardiographic findings revealed significant reduction in left ventricle ejection fraction (LVEF; P < .001) and significant increase in left ventricular end diastolic diameter (LVEDD; P < .001) in patients with poor disease outcome, while no significant difference was found between the 2 groups as regards age, sex, or cardiovascular risk factors (Table 3). Early MMP-9 levels were also significantly higher among patients who underwent coronary revascularization compared to those without coronary revascularization (median 5800 vs 3300 pg/mL; P < .001). Early MMP-9 levels were positively correlated with LVEDD (r = .721, P < .001) and negatively correlated with LVEF (r = –.682, P < .001).
Impact of Different Clinical and Laboratory Data on Disease Outcome in Patients With ACS.a
Abbreviations: BMI, body mass index; CK, creatine kinase; CK-MB, creatine kinase myocardial fraction; cTnT, cardiac troponin T; LDH, lactate dehydrogenase; LVEF, left ventricular ejection fraction; LVEDD, left ventricle end diastolic diameter; MMP-9, matrix metalloproteinase 9; SD, standard deviation.
aGood outcome: stable state, no complications. Poor outcome: recurrence of ischemic attacks, congestive heart failure, or death. Data were expressed as mean ± SD using student t test or as median using Mann-Whitney test for comparison unless specified as number (percentage) using chi-square (χ2) test for comparison.
Diagnostic and Prognostic Utility of MMP-9 in Cardiac Disease
Receiver–operating characteristic curve analysis revealed that the best cutoff value of 3100 pg/mL of MMP-9 was able to discriminate patients with myocardial infarction (MI) from those with UA with a sensitivity of 80%, specificity of 80%, negative predictive value of 66.7%, positive predictive value of 88.9%, and accuracy of 85%. Furthermore, the prognostic utility of MMP-9 to predict a poor disease outcome was established at 4700 pg/mL showing sensitivity of 72.4%, specificity of 83%, negative predictive value of 83%, positive predictive value of 71.4%, and accuracy of 79%.
Discussion
The concept of the cardiovascular continuum, introduced during the early 1990s, created a holistic view of the chain of events connecting cardiovascular-related risk factors with the progressive development of pathological-related tissue remodeling and ultimately heart failure and death. The majority of the existing markers are useful only in the end stages of the disease where few successful intervention options exist. Since a large number of patients experience a transient underlying developing pathology long before the signs or symptoms of cardiovascular disease become apparent, the requirement for new markers that can describe the early tissue-specific, matrix remodeling process which ultimately leads to disease is evident. 17
The results of the present study revealed that patients with ACS had a significantly higher serum MMP-9 level when compared to patients with SA and the healthy control group, with the highest levels found among STEMI group. Similar results were found in other studies. 12,18 –21 This may indicate that the levels of MMP-9 progressively increase with severity of the clinical presentation.
On stratifying patients with ACS into subgroups according to disease outcome, the significant differences between patients having good versus poor disease outcome were found in relation to echocardiographic findings of impaired left ventricular function and the elevation in early MMP-9 levels in patients with poor disease outcome, while baseline levels of other cardiac enzymes which are considered well-established markers of extensive myocardial necrosis did not show a prognostic value. Furthermore, we demonstrated a strong association between serum level of MMP-9 and subsequent risk of cardiovascular complications. This was in agreement with other studies 18,22 –24 where serum concentrations of MMP-9 at baseline were found to be significantly higher among patients who subsequently experienced a fatal cardiovascular event during follow-up compared with those who did not.
The association between early MMP-9 levels and post-MI impairment of left ventricular function, as evidenced by the significant correlation with both LVEDD and LVEF among our patients, supports its usefulness in prediction of left ventricular remodeling. Kelly et al 25 found that peak plasma concentrations of MMP-9 were associated with greater impairment of LV function during the index admission and predicts the degree of LV remodeling in the weeks after discharge.
Moreover, Gostiljac et al 26 found that other markers of plaque rupture have not shown expected efficiency in comparison to MMP-9, which has been marked as a very useful marker of early rupture. These findings can be explained by the fact that MMP-9, which is released from cells in the arterial wall (such as smooth muscle cells, monocytes, and macrophages), leads to degradation of the fibrous cap of the vulnerable atherosclerotic plaque and that accelerates plaque rupture. 12 Therefore, Gostiljac and colleagues 26 suggested the use of MMP-9 to predict presence, severity, and extent of CAD complications.
In our study, we found a significant correlation between MMP-9 serum level and heart rate, in consistence with Sundström et al 27 who found that increasing heart rate was a key clinical correlate of detectable plasma MMP-9. The association of plasma MMP-9 with heart rate is intuitive because a higher heart rate is associated with increased myocardial oxygen consumption and wall stress and is an indicator of increased risk of heart failure. 28
In the current study, MMP-9 was positively correlated with markers of myocardial necrosis such as CK and LDH. Kułach et al 29 explained these results by the increased activity of circulating monocytes (which release MMP-9) that is related to more extensive myocardial necrosis and subsequently result in worse prognosis of ACS. Therefore, in agreement with Alsheikh et al, 30 we can consider MMP-9 as a reliable risk marker in patients with CHD.
On the contrary, Tanindi et al 18 failed to demonstrate a correlation between MMP-9 and these cardiac enzymes and attributed the lack of correlation between MMP-9 and these cardiac enzymes to technical inability because it was impossible to obtain the blood samples exactly at the same time from the beginning of the chest pain for each participant, as sampling was done after 72 hours of hospital admission and in many participants was done after angiography which may have altered their results.
Regarding the success of MMP-9 as a marker to predict ACS, studies assumed that the special importance of defining MMP-9 in serum comes from the supposition that making an early diagnosis of ACS is possible earlier before irreversible myocardial necrosis occurs. 14 Meanwhile, there is a growing interest for MMP-9 both as a diagnostic marker and as a therapeutic target in cardiovascular disease. 31 Therefore, in our study, we constructed an ROC curve to define the best cutoff value for discriminating patients with MI from patients with UA and showed that the best cutoff value was 3100 pg/mL, with high sensitivity and specificity. Furthermore, MMP-9 cutoff 4700 pg/mL was able to predict poor disease outcome. Taken together, the significant association between higher median MMP-9 level and poor disease outcome in our patients with ACS in the absence of any significant association between such state and any of the cardiac enzymes imply that MMP-9 may represent a promising prognostic marker in patients with ACS. In agreement, Blankenberg et al 23 found that plasma MMP-9 concentration was identified as a novel predictor of cardiovascular mortality in patients with coronary artery disease.
Moreover, the present study showed that patients with ACS having high MMP-9 levels at diagnosis have an increased risk of coronary revascularization. A recent study by Wang et al 32 analyzed MMP-9 levels 18 months after acute MI (AMI) and demonstrated that MMP-9 was an independent predictor of coronary revascularization, suggesting a pivotal role of MMP-9 in atherothrombosis in patients with AMI.
In conclusion, MMP-9 could be considered as an early risk marker for identification of patients with ACS. It can reliably discriminate those with acute MI from UA. High levels are closely associated with disease severity and the extent of ACS complications. Further prospective studies with longer follow-up and serial measurement of MMP-9 throughout the course of therapy are needed to detect its usefulness in predicting future coronary revascularization among patients with MI and validate the MMP-9 cutoff before incorporation in risk stratification.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.