
Abstract
Nowadays, we have a relatively sophisticated standard approach to a patient with acute ischemic stroke, including the sequence of diagnostic methods and treatment modalities. In practice, however, we are occasionally confronted with a patient whose medical history or comorbidities force us to make a decision without the support of guidelines. One such situation is the occurrence of acute ischemic stroke in a patient with known idiopathic thrombocytopenic purpura, where a tendency to use thrombolysis, anticoagulants, or antiplatelet agents collides with the fear of life-threatening bleeding. In this review, we try to outline current understanding of the pathophysiology of “paradoxical” ischemic events in this illness characterized by thrombocytopenia and to summarize clinical experience from case reports dealing with this topic, which could help us to rely on more than individual opinion seen through a purely “neurological” or “hematological” prism.
Keywords
What is ITP
Idiopathic thrombocytopenic purpura (also known as immune thrombocytopenia, ITP) is a chronic illness defined by a decrease in platelet count under the level of 100 × 109/liter without concomitant leukopenia or anemia. Idiopathic thrombocytopenic purpura can be divided into primary ITP, which is not associated with other conditions, and secondary ITP, which can be associated with hepatitis C virus, human immunodeficiency virus, with Helicobacter pylori infection, and with certain autoimmune (systemic lupus erythematosus and antiphospholipid syndrome) or lymphoproliferative (CLL) illnesses. 1 The estimated incidence of ITP (according to epidemiological studies with the best methodology) is 2.2 to 5.3 cases per 105 children/year and 3.3 new cases per 105 adults/year. 2 The prevalence of chronic nonsecondary ITP in adults is 0.08% (80 cases in 100 000 person). 3 The incidence of immune thrombocytopenia grows throughout adulthood. Until about the age of 60 years, the occurrence of ITP is more frequent in women. The peak of incidence in children is between 5 and 6 years and is usually bound to viral infection. 1 Idiopathic thrombocytopenic purpura can also occur in neonates, where the most frequent cause is the transplacental passage of autoantibodies from a mother with ITP. 4
Pivotal in the pathogenesis of ITP is immune-mediated platelet destruction, together with suppression of their production. 5 The primary cause of autoantibodies production is not known. 6
Idiopathic thrombocytopenic purpura can be asymptomatic or can manifest itself with petechiae, ecchymoses, bleeding from mucous membranes, frequent nosebleeds, excessive menstrual bleeding, or serious bleeding into the gastrointestinal tract or brain. 7 The diagnosis of ITP is clinical, “ per exclusionem” of other conditions. Up to now, there is no specific confirmatory test. It is also necessary to distinguish other causes of the immune-mediated thrombocytopenia than ITP: thrombotic thrombocytopenia purpura (TTP), heparin-induced thrombocytopenia (HIT), and antiphospholipid syndrome (APS). The important fact with respect to the topic of this article is that all these 3 conditions can lead to a prothrombotic state. 8 The diagnosis of primary ITP is based on the exclusion of secondary causes. 1,6
In the first line of ITP therapy, peroral or intravenous corticosteroids, intravenous immunoglobulins (IVIGs), and intravenous anti Rho(D) are used; in the second line, monoclonal antibodies (rituximab), agonists of the thrombopoietin receptor (romiplostim, eltrombopag), and splenectomy are used. 1
Thrombotic Events as Complications of ITP
Although the greatest danger of ITP is life-threatening bleeding during severe thrombocytopenia, 9 this illness is paradoxically frequently associated with thrombotic events. 10 Studies concerned with the comorbidities of ITP revealed increased risks of sudden vascular illnesses generally and of ischemic stroke and transient ischemic attack (TIA) in particular. 11
There are many possible explanations of the tendency of patients with ITP to have thromboses. The best known is the role of platelet microparticles (PMPs), products of immune-mediated platelet destruction. High serum levels of PMPs were detected in patients with ITP and concurrent TIAs or small ischemic strokes. 12,13 A causal relationship between PMP serum level and the progression of intracranial vascular stenosis was observed in a 60-year-old female patient with ITP and stroke. A decrease in PMP serum level with immunosupressive therapy correlated with an elevation of platelet count and the progressive withdrawal of neurological symptoms. After the reduction in immunosupressive therapy, the neurological symptoms again worsened. At this stage, magnetic resonance angiography revealed an extended degree of middle cerebral artery stenosis. 14 It is assumed that patients with ITP have younger and thrombotically more active platelets than healthy people, which also increases the risk of thrombosis. 15 Other contributory factors can be circulating platelet–leukocyte–monocyte aggregates, endothelium-activating antibodies, the activation of the complement system, and low serum levels of a disintegrin and metalloproteinase with a thrombospondin type 1 motif, member 13 (ADAMTS-13). 16 The risk of thrombosis in patients with ITP increases significantly in the presence of positive lupus anticoagulant. In a large proportion of these patients, antiphospholipid syndrome develops later. 17 Patients with ITP and positive antiphospholipid antibodies (lupus anticoagulant and anticardiolipin antibodies) should therefore be observed more rigorously. 18
Several epidemiological studies have been devoted to the occurrence of arterial and venous thromboembolism in patients with ITP. It was found that patients with ITP have a higher risk of venous thromboembolism, including deep venous thrombosis, portal vein thrombosis, and pulmonary embolism in comparison with the risk of arterial thromboembolism. 10,11 Concerning arterial thromboembolism, there are contradictory results—a higher risk of myocardial infarction but not of ischemic stroke or TIA 10 or a higher risk of ischemic stroke and TIA but not of myocardial infarction. 11 It is also known that there is a subpopulation of patients with ITP having a higher risk of vascular dementia. These patients have a higher level of platelet activation, a higher serum level of PMPs, and a higher level of CD62p (P-selectin) expression. 19
Thrombotic complications in patients with ITP are relatively often the consequence of IVIG treatment. Of the 15 case reports of ischemic stroke in patients with ITP mentioned subsequently, we identified 4 cases of acute ischemic stroke which occurred in the days after IVIG treatment, 20 –23 including 1 case which occurred immediately after IVIG infusion. 20 About 75% of IVIG-related thrombotic events occur within 24 hours of infusion, 50% occurring within the first 4 hours. Such events were reported only infrequently after an interval of more than 1 week. 24 The reason for these complications may be an increase in the viscosity of plasma depending on the dose of IVIG, which can persist for 3 to 5 days after the end of treatment, and an increase in the viscosity of plasma following a sudden increase in the platelet count or IVIG-induced arterial vasospasm, which can cause the destabilization of local atherosclerotic plaque with thrombosis formation. The risk of thrombotic complications after treatment with IVIG is also related to other properties of IVIG infusions, such as sugar content, or to the dosages and duration of the therapy. 21 Patient-related factors associated with the higher risk of thrombosis following treatment with IVIG are older age, associated arterial hypertension, and hypercholesterolaemia. 24 The impact of associated vascular risk factors on the risk of a thrombotic event occurring is probably proportionately higher in stabilized patients with ITP having a sufficient platelet count.
Therapy with corticosteroids can also play a possible role in the formation of a hypercoagulable state, which is common in patients with ITP. 25 Also, splenectomy increases the risk of thrombotic events. 26
Ischemic Stroke in the Context of ITP
Although ischemic stroke, alongside other thrombotic events, is a well-known complication of ITP, 11 there is no consensus on the precise therapeutic approach. 27 A necessary condition is close cooperation between the neurologist and the hematologist. A literature search on this topic provides only a few case reports concerning the manifestation of ischemic stroke in patients with ITP but no systematic study dealing with the management of stroke in these patients in the acute phase and in secondary prevention. Here, we tried to summarize case reports published up to the present time in order to enlighten physicians facing this difficult clinical situation. We included case reports concerning the manifestation of ischemic stroke in adult patients with ITP in both English and French, indexed by the PubMed service and displayed after searching for “idiopathic thrombocytopenic purpura + stroke” or “immune thrombocytopenia + stroke”. The summary is presented in Table 1.
Summary of Published Case Reports Regarding Stroke in Patients With ITP.
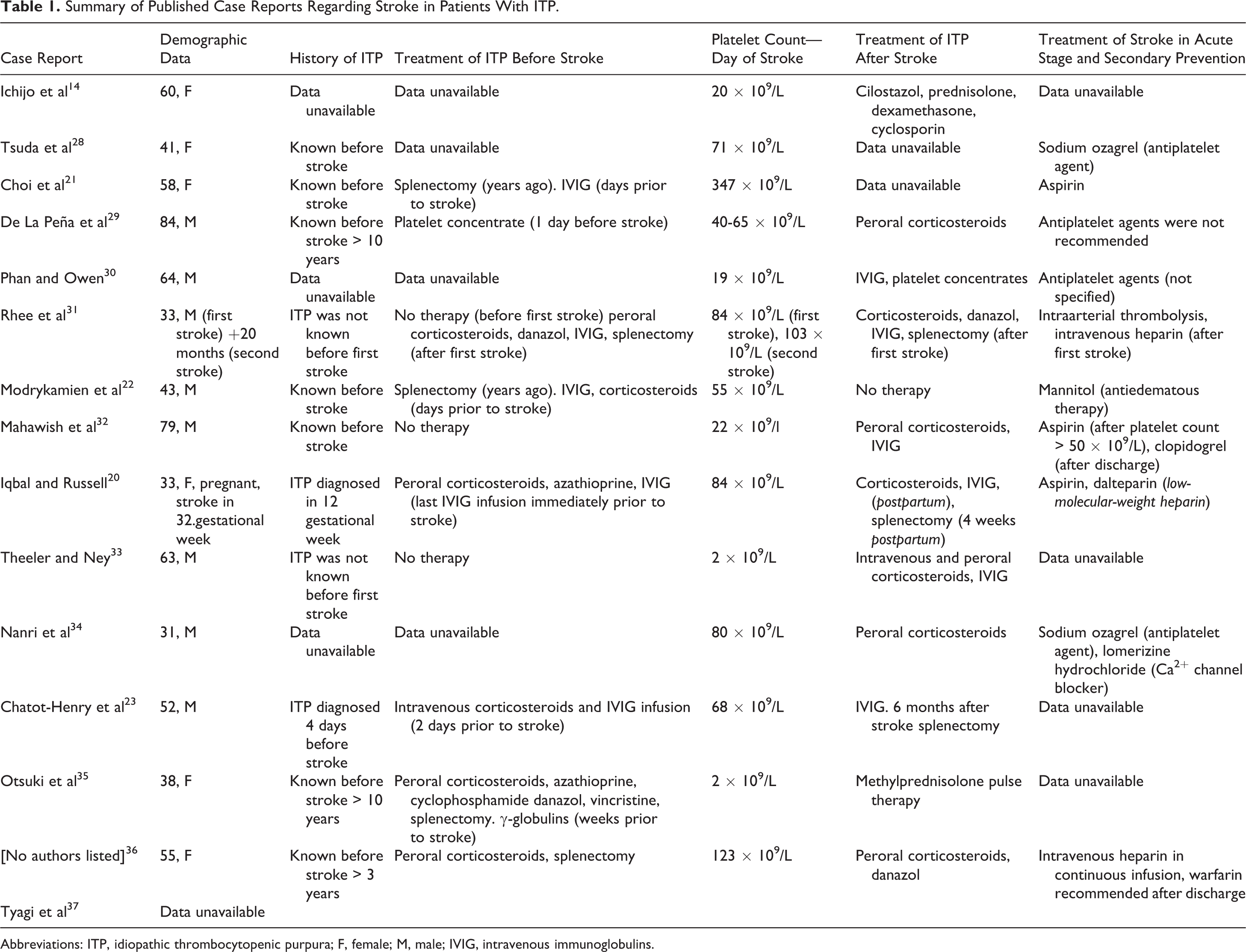
Abbreviations: ITP, idiopathic thrombocytopenic purpura; F, female; M, male; IVIG, intravenous immunoglobulins.
However, we should keep in mind that the serious neurological complication which best corresponds with the main characteristics of ITP is intracranial bleeding. According to Nørgaard et al, the 5-year cumulative rate of intracranial hemorrhage in patients with ITP is approximately double that of the control population. All patients affected by ITP and also by intracranial hemorrhage had a platelet count lower than 30 × 105/liter. 38
Treatment of Ischemic Stroke in a Patient With ITP
Thrombolysis
Patients in the acute phase of ischemic stroke need to be classified with regard to indications and contraindications for thrombolysis. One of the contraindications for treatment with tissue plasminogen activator (tPA; according to a protocol based on the The National Institute of Neurological Disorders and Stroke (NINDS)-rt-PA Stroke Study Group study) is a platelet count of less than 100 × 105/liter. 39 Other contraindications, not specified in the pivotal NINDS study but present in the summary of product characteristics of alteplase, are known hemorrhagic diathesis and significant bleeding disorder, either exhibited by the patient or having occurred within the past 6 months. 40
To our knowledge, there is no report of intravenous thrombolysis being used in a patient with ITP. Rhee et al describe the case of a patient with ischemic stroke who was treated with intraarterial thrombolysis with urokinase. His platelet count in the acute phase of stroke was 84 × 105/liter; the diagnosis of ITP was made after the thrombolytic treatment. The effect of that treatment was good; no bleeding complications occurred. 31 Up to this time, there is also no reliable data concerning the risks of administering tPA treatment to patients with thrombocytopenia. The boundary value of 100 × 105 platelets/L was defined in an initial research study with tPA and henceforth adopted in guidelines and clinical practice. 39,41 As the risk of serious bleeding in patients with ITP is associated with low platelet count, and as the risk of intracranial hemorrhage in patients with a platelet count of over 20 × 105/L and no hemostatic commorbidity, trauma, or history of recent major surgery is extremely low (the risk of major bleeding is generally low when the platelet count is over 30 × 105/liter), 6 a question arises: how risky would it be to administer tPA treatment to patients with ITP and sufficient platelet counts—for example, over 100 × 105/L? Because of the above-mentioned strict contraindications of thrombolytic treatment and the possibility of the relatively free interpretation of the term “hemorrhagic diathesis,” this remains in many cases only an academic question.
Intravenous thrombolytic treatment in the context of other immune-mediated illnesses such as TTP 42 and antiphospholipid syndrome 43 was already reported.
The use of intravenous thrombolysis in patients with ITP and concomitant thrombotic events other than stroke was reported in a patient with pulmonary embolism and bilateral deep venous thrombosis after splenectomy. 44
Antiplatelet Agents and Anticoagulation
Up to this time, the effects of antiplatelet agents and anticoagulation in the already-described clinical situations are not yet fully apparent. Skeptical opinion in relation to antiplatelet agents results from the fact that neither aspirin nor dypiridamole have an influence on levels of PMPs. 13 The effect of clopidogrel may be better: one study showed a nonsignificant lowering of PMP levels after treatment with clopidogrel. 45 The administration of antiplatelet agents and anticoagulants in the therapy for a patient with ITP and concomitant stroke should be adjusted according to his or her risk factors, comorbidities, and risk of hemorrhagic transformation. 31
In one published case, the authors decided not to administer antiplatelet agents because of the patient’s low platelet count 29 ; others treated their patients with aspirin, with other antiplatelet agents such as sodium ozagrel, 28,34 and with heparin, 20,31 or they recommended clopidogrel after discharge. 32 At the same time, most patients were treated with corticosteroids, IVIG, or immunosuppressants. 20,31,29,34,32,30 What was emphasized was the promising effect of the combination of platelet destruction suppression with IVIG and corticosteroids followed by treatment with antiplatelet agents. 32 One particularly remarkable case was described by Ichijo et al, in which intensive immunosupressive therapy led to a lowering of PMP levels, an increase in platelet count, a decrease in the degree of intracranial vascular stenosis, and an improvement in the neurologic deficit caused by stroke. 14 The level of PMPs can also decline through treatment with calcium channel blockers. 12,13 Matzdorff and Beer propose a therapeutical algorithm for patients with ITP and thrombotic complications. They suggest the administration of anticoagulants up to a platelet count of more than 30 to 50 × 105/L, but only if no life-threatening bleeding or bleeding with the need of transfusion occurs. In the first 48 hours, it is preferable to start treatment with unfractionated heparin. If no bleeding occurs, the transition to low-molecular-weight heparin is possible. 27 For a definitive evaluation of treatment with antiplatelet agents and anticoagulants, further studies are required.
Conclusion
The dilemma associated with the treatment of acute ischemic stroke in most patients with ITP concerns the use of antiplatelet agents or anticoagulants in the context of present or imminent thrombocytopenia. At the same time, there is no dispute about the parallel use of immunosuppressants. There are indications that adequate immunosupressive treatment has a causal effect on the mechanism of thrombotic vessel occlusion in the acute stage of ischemic stroke. 14 At this crucial stage of stroke, most neurologists have learned to think about thrombolysis. Because of the controversy surrounding this type of treatment in this particular clinical situation, novel approaches appear to be very attractive for future research. Meanwhile, the traditional practice of the medicamentous secondary prevention of stroke retains its validity, particularly with respect to a patient with a significant vascular risk factor profile, assuming a stabilized hematological status.
Currently, there is a need for additional research into the pathophysiology of thrombotic events in the context of ITP and of its therapeutic influence, which could help to promote isolated examples of successful treatment into standard practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.