
Abstract
Deep vein thrombosis (DVT) and pulmonary embolism are major causes of morbidity and mortality in patients during hospitalization; previous studies have proposed that an advanced age of more than 60 years is a risk factor for these conditions. This study analyzes the relative risk of DVT in very elderly patients older than 90 years of age compared with elderly patients aged 80 to 89 years. The study was performed at the Department of Internal Medicine, University Hospital of Saarland, Homburg/Saar, Germany, between 2004 and 2012. After completing ultrasound examinations, 20 (64.52%, 12 [60%] female patients, mean age 91.8 ± 1.83 years) of the 31 patients in the study group and 132 (62.26%, 87 [65.91%] female patients, mean age 83.84 ± 2.66 years) of the 212 patients in the control group were diagnosed with DVT. An increased relative risk of DVT was not discovered in the very elderly patients (relative risk, 1.04; P = .80).
Introduction
Deep vein thrombosis (DVT), which is the clotting of blood components in the veins located deep within the leg, is the third most common cardiovascular disease after heart attack and stroke. 1 –3 Deep vein thrombosis can create a high risk for the development of pulmonary embolism, which is a primary and potentially life-threatening complication of DVT. Therefore, early diagnosis and aggressive and proactive treatment of DVT is crucial in effectively preventing pulmonary embolism. Deep vein thrombosis and the development of pulmonary embolism are the main causes of morbidity and mortality in patients of all ages and medical backgrounds; nevertheless, elderly patients are at a higher risk of DVT than younger patients. 4 Reduced physical mobility is relevant to the development of the condition, and elderly patients have reduced physical mobility and high hospitalization rates for illnesses that contribute to the development of DVT and induce a greater risk of generating pulmonary embolism. 5 Previous studies have asserted that advanced age is a risk factor in the development of DVT and that the incidence of DVT increases significantly with increasing age. 4 –7 As the average life expectancy continues to increase, DVT will become a major health problem worldwide. Further, elderly patients develop common internal illnesses, such as congestive heart failure, chronic obstructive pulmonary disease (COPD), acute infection, and atherosclerotic vascular disease, which increase the risk of DVT. 5 Since the detection of DVT can be a challenge, given that common symptoms of DVT may be absent, this study was conducted to accurately identify very elderly patients at risk of DVT. Ultimately, DVT can only be prevented when the risk factors and risk groups for DVT are understood and identified.
Hospital chart data from the Department of Internal Medicine, University Hospital of Saarland, Homburg/Saar, Germany, were analyzed for nonagenarian and octogenarian patients who were examined after DVT to assess the relative risk of DVT in this age-group. All outpatients treated at the Internal Medicine Emergency Department and all the Internal Medicine Department’s hospitalized patients aged older than 80 years were included in the study. Patients hospitalized in all other departments of the University Hospital were excluded from this study for better comparison of the study population by including possible internal medicine primary disease as a requirement of the study design. This study was also performed to identify the typical clinical manifestations of DVT in the very elderly patients as well as acute and chronic comorbidities as possible risk factors. Further,
Materials and Methods
Patients
All data pertaining to patients with risk factors for DVT based on clinical gestalt were collected at the Department of Internal Medicine of the University Hospital of Saarland, between 2004 and 2012. The relative risk of DVT in the last decade of a patient’s life was considered theoretically by assuming that the average life expectancy would be 100 years of age. For the control group, the second highest decade of life was chosen to avoid any distortion in the data analysis due to age. The second highest decade of life refers to patients between 80 and 89 years of age. Thus, the study population was composed of very elderly patients older than 90 years of age diagnosed with DVT, and the control group was composed of elderly patients between 80 and 89 years of age diagnosed with DVT. The relative risk was calculated from the ratio of the probability of the presence of DVT to the probability of the absence of DVT by examining duplex ultrasounds of patients in both the groups. Deep vein thrombosis is defined as a blood clot within a major vein with the primary location of the iliac vein, femoral vein, popliteal vein, and the lower leg veins in one or both legs at the same time. All patients suspected to have developed DVT based on the use of physician clinical gestalt assessment underwent venous ultrasound imaging after physical examinations to confirm or refute the diagnosis of DVT. This suspicion was established along with symptoms of likelihood of DVT including pain, erythema, swelling, and warmth in the affected leg. Although the probability of DVT can be calculated using either the Wells or the Revised Geneva scores, these calculations were not considered for this study since all patients underwent follow-up ultrasound testing. Therefore, the negative influence of the nonexamination of patients by means of ultrasound should be avoided since these 2 scores estimate the pretest probability of DVT.
The description of the location of DVT in the veins was classified into iliofemoral, femoropopliteal, popliteal, and calf DVT. The classification of DVT was performed according to the most recent edition of the International Classification of Disease (ICD I80.20) from 2004 to 2012. A
Statistical Analysis
The data were expressed in proportion, mean, and standard deviation wherever appropriate. Relative risk and 95% confidence intervals (CIs) were calculated and compared between the very elderly patients and the elderly patients for the occurrence of DVT. Fisher exact test was used to compute the location of DVT in the legs, clinical signs for DVT in the very elderly patients and elderly patients, the difference in cardiovascular risk between the 2 groups, and the difference in acute and prior thromboembolic diseases in both the groups. The chi-square test was used to calculate sex difference, demographic data, clinical data, cardiovascular risk factors, acute and prior thromboembolic diseases, and acute and chronic internal illnesses. The Mann-Whitney U test was used to compare age difference, the difference in
Results
A total of 2770 patients who were believed to be at risk of DVT based on clinical features, such as pain, erythema, swelling, and warmth in legs, were examined for DVT at the Department of Internal Medicine of the University Hospital, in the study period from 2004 to 2012. Of these, 31 (1.12%) were in the study group and 212 (7.65%) were in the control group. The number of patients with DVT rose with the annual fluctuation rates between 2004 and 2012 (Figure 1). There was a significant difference in the number of cases between both the groups during the study period (P = .000287). There were 11 (35.48%) men and 20 (64.52%) women in the study group, and 74 (34.91%) men and 138 (65.09%) women in the control group (P = .9497). Deep vein thrombosis was diagnosed in 20 (64.52%; 95% CI, 47.68-81.36) patients in the study group and 132 (62.26%; 95% CI, 55.73-68.79) patients in the control group. More women were diagnosed with DVT in both groups but without statistical significance (P = .6053; Table 1). The relative risk (1.04; 95% CI, 0.78-1.37; P = .80) for the occurrence of DVT did not increase in the very elderly patients older than 90 years of age compared with elderly patients who were between 80 and 89 years of age. A significant difference in the age of patients with DVT was found between the 2 groups (P < .001). There was also no statistical difference in the frequency of the right or left leg being affected by DVT (P = .2875) and the location of DVT (P = .6272). The clinical symptoms of pain, erythema, swelling, and warmth were not statistically significant signs of DVT in the very elderly group compared with the control group (P = .2196). The numerical difference in the level of
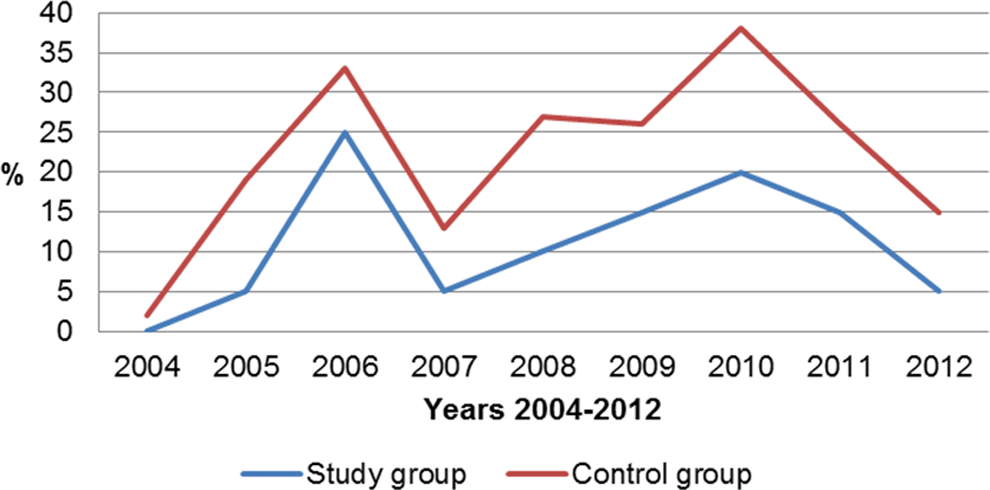
Trends in rates of deep vein thrombosis in both the groups.
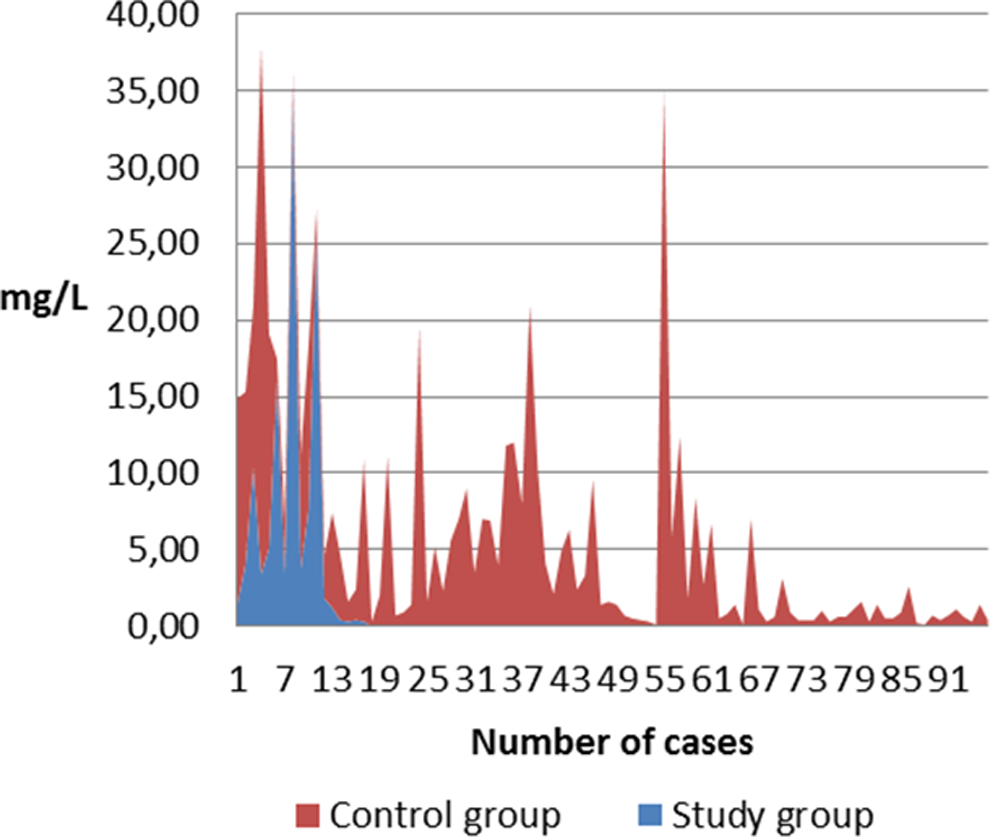
Comparison of
Demographic and Clinical Data of Patients with Deep Vein Thrombosis.a
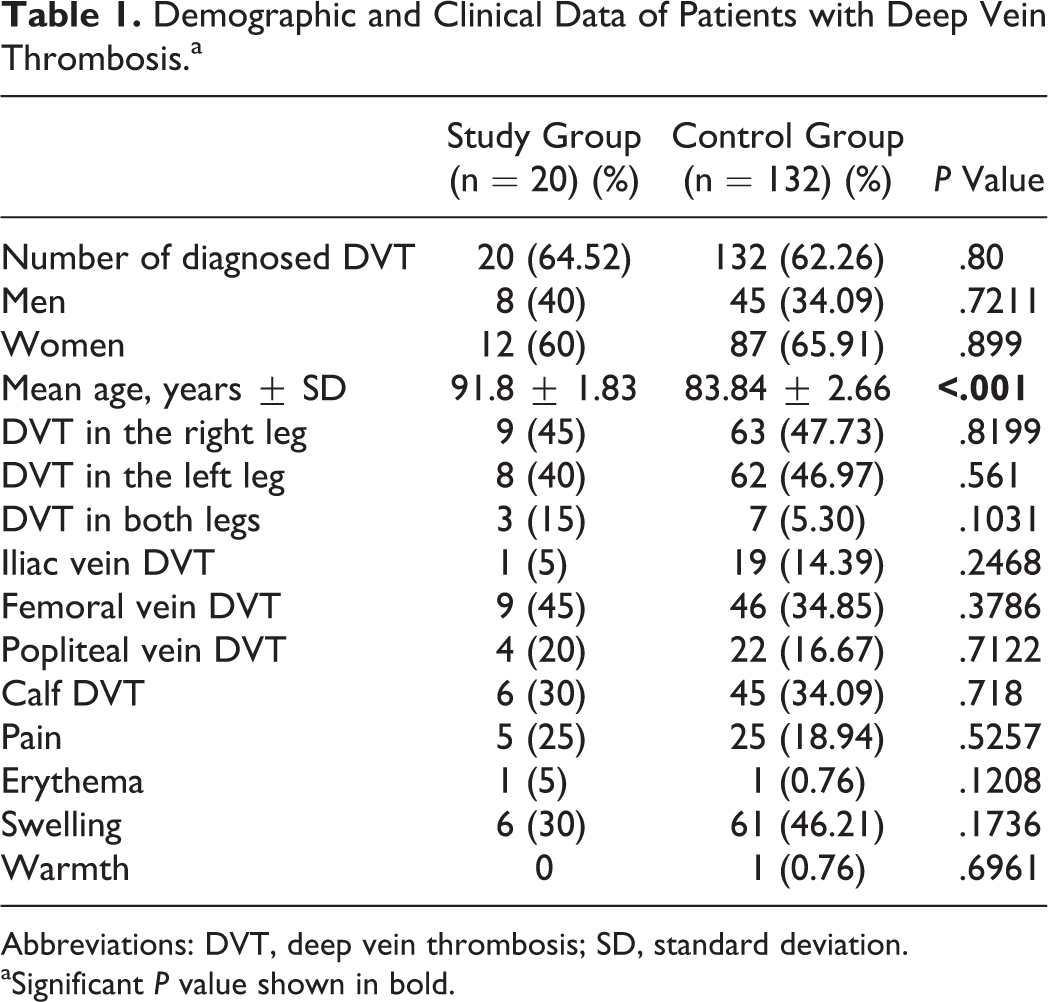
Abbreviations: DVT, deep vein thrombosis; SD, standard deviation.
aSignificant P value shown in bold.
Comparison of
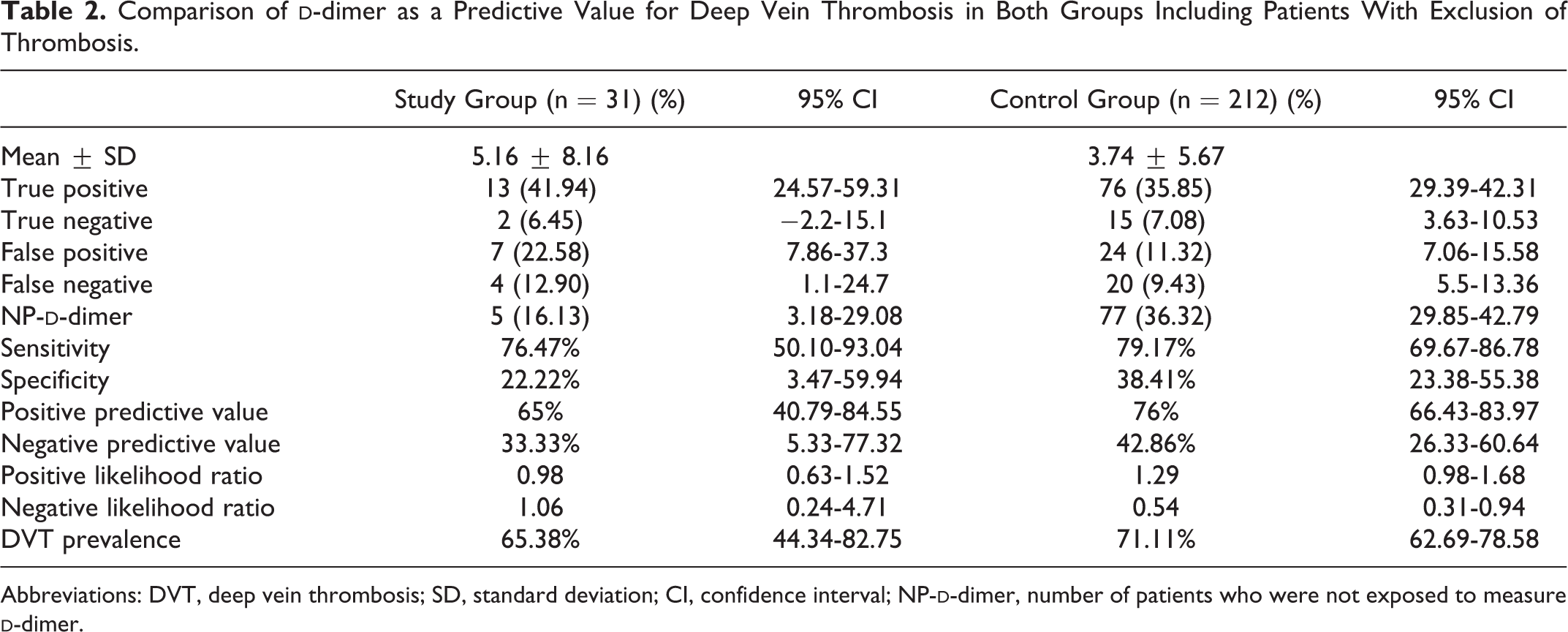
Abbreviations: DVT, deep vein thrombosis; SD, standard deviation; CI, confidence interval; NP-
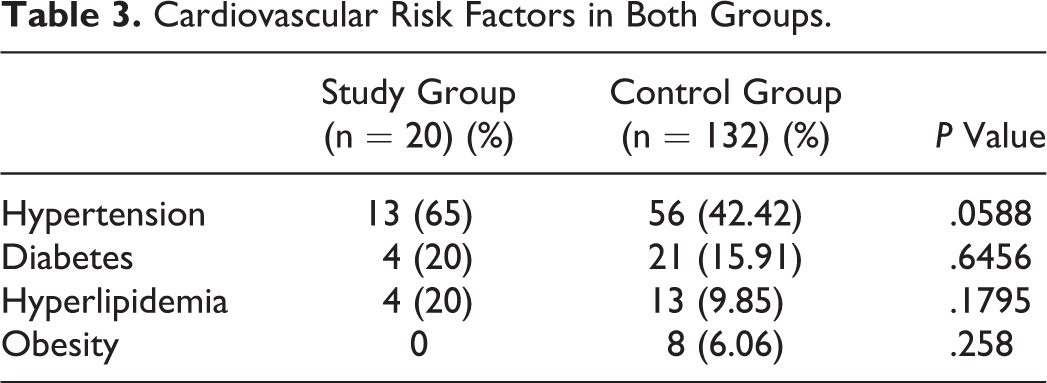
Cardiovascular Risk Factors in Both Groups.
Recognized Disorders as a Risk Factor for Deep Vein Thrombosis in Both Groups.a
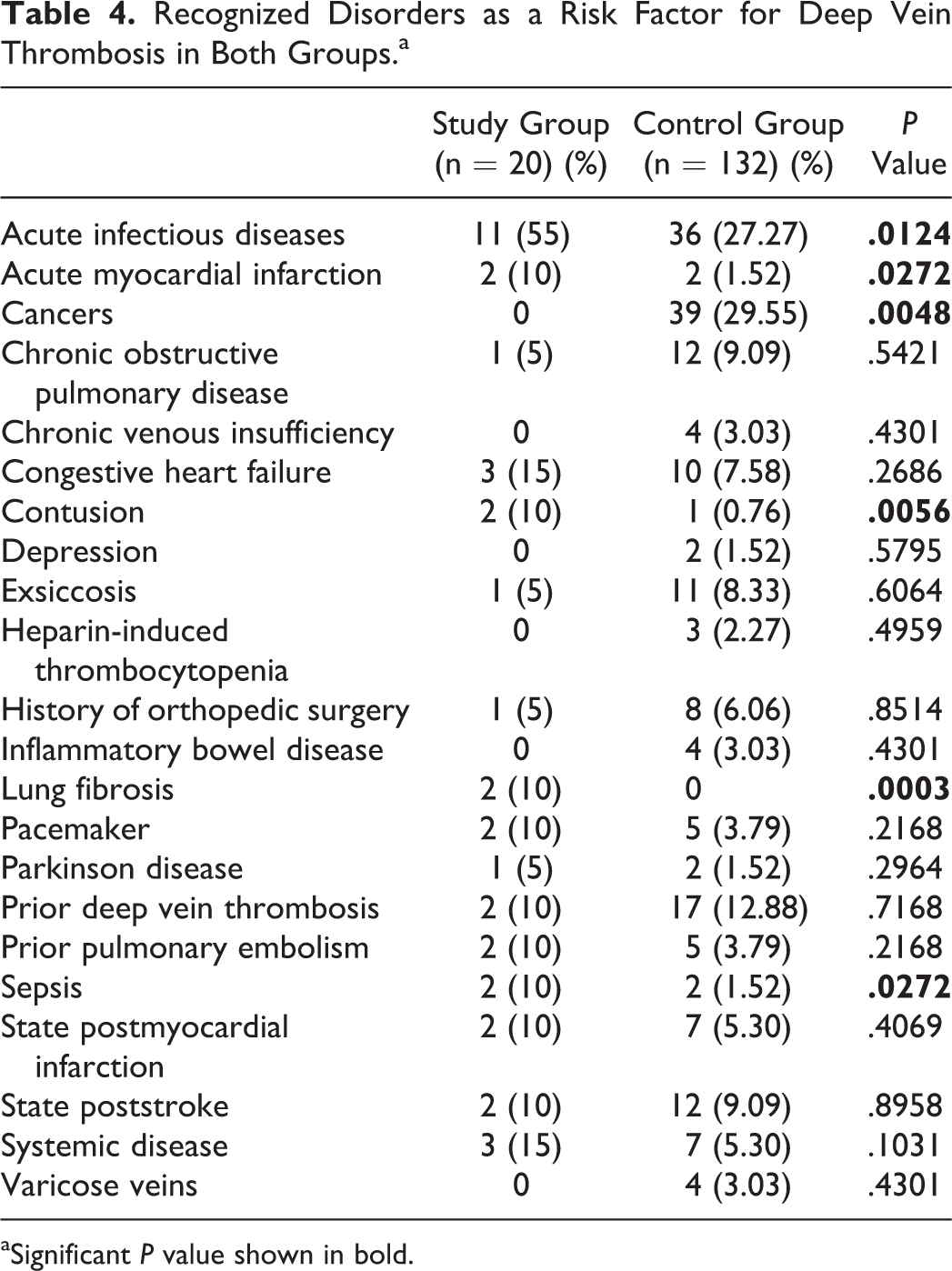
aSignificant P value shown in bold.
Acute Comorbidities in the Study and Control Groups.a
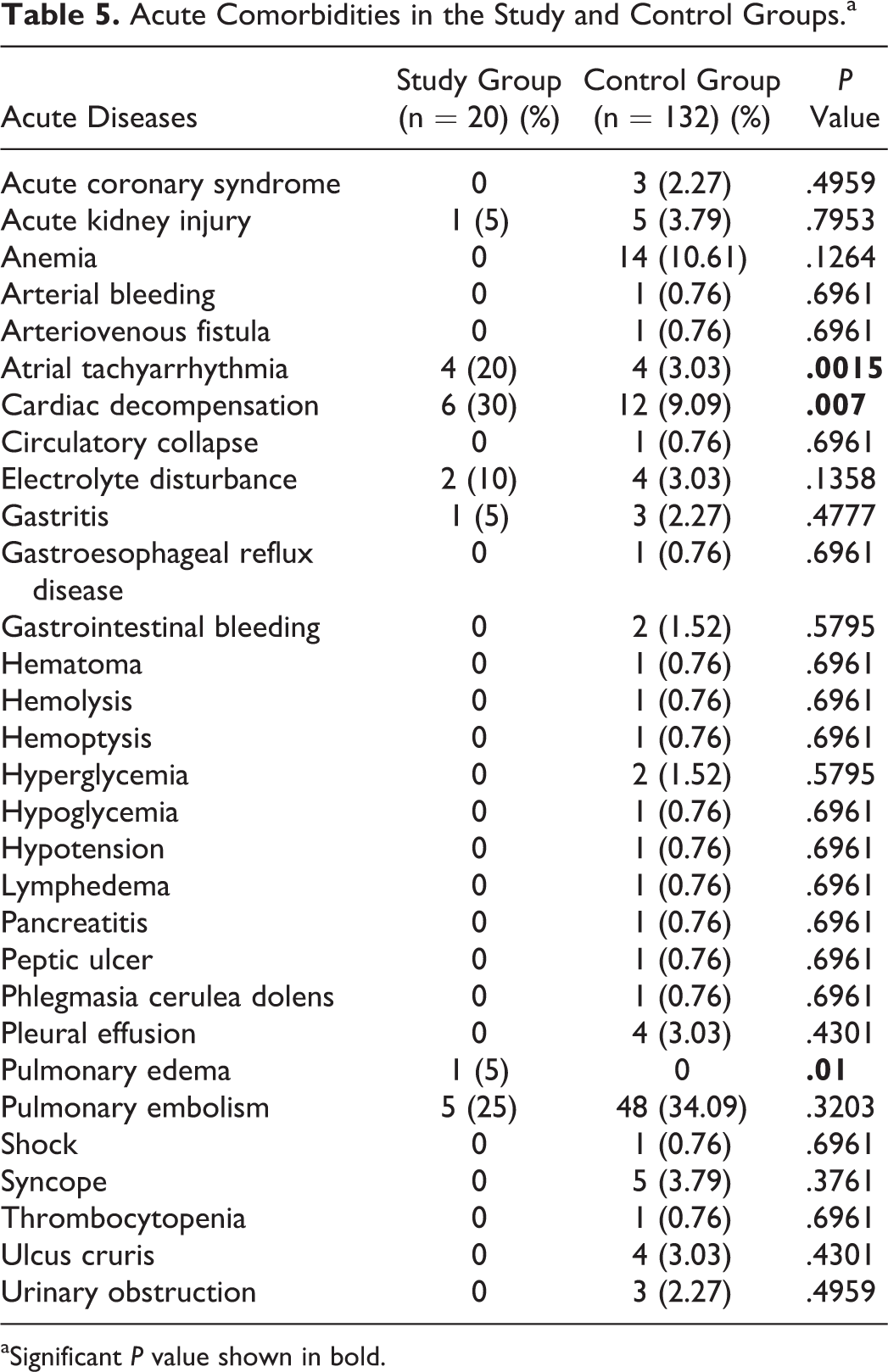
aSignificant P value shown in bold.
Various Comorbidities in Elderly Patients Aged >80 Years With and Without Deep Vein Thrombosis.a
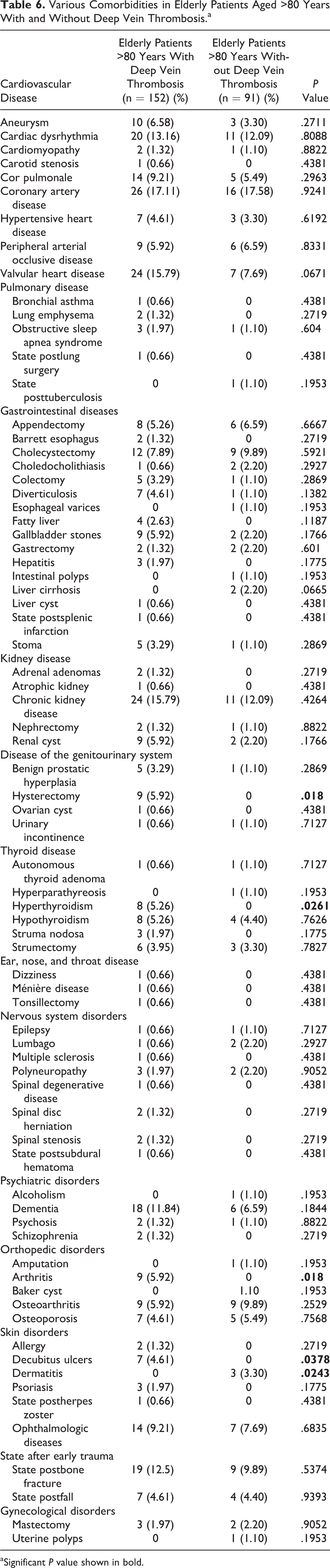
aSignificant P value shown in bold.
Therapy of Deep Vein Thrombosis in Both Groups.a
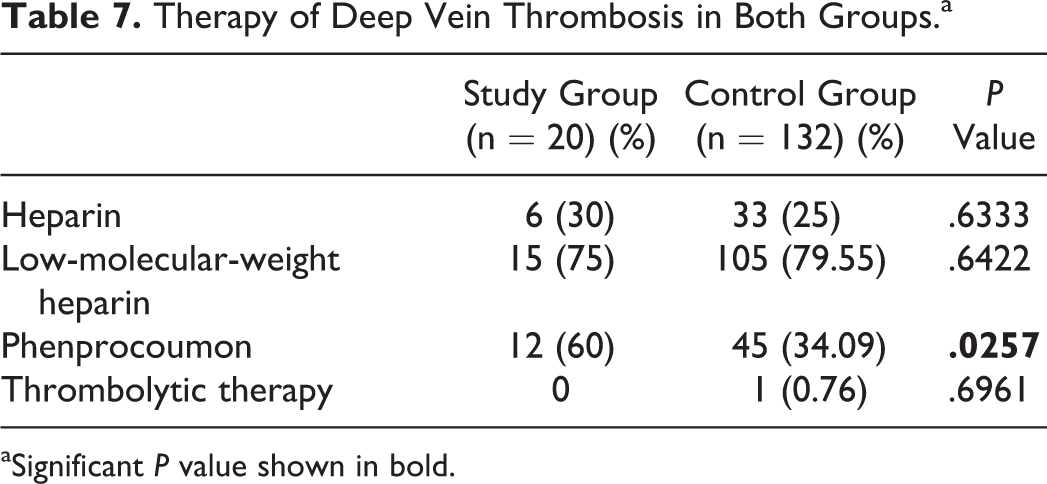
aSignificant P value shown in bold.
Discussion
Although previous studies postulated a higher risk of DVT with increasing age, 3 –7 the results of the current study showed relatively no increased risk of DVT in the very elderly patients older 90 years of age compared with the elderly patients between 80 and 89 years of age. Although the incidence of pulmonary embolism decreased in patients of all ages over time, the incidence of DVT in older men remained unchanged while it increased in older women. 7,13 The annual number of DVT diagnoses also increased in our study but was not continuous, with a marked rise and fall according to annual fluctuation rates. We diagnosed more elderly women with DVT than elderly men, but without statistical significance, corroborating the findings in the study by Silverstein et al. 7 There was a considerably lower proportion of very elderly patients included in our study, and these patients did not have an increased risk of DVT in comparison with the elderly patients. The outcomes of our study could be affected by the small number of patients in the study group as well as the fact that our study was conducted in a single Department of Internal Medicine. Furthermore, the number of patients becomes smaller with increasing biological age.
Since the typical clinical symptoms of DVT may be absent or uncharacteristic, 5 diagnosing DVT can be a challenge, and the illness can be easily overlooked. Accordingly, pain, erythema, swelling, and warmth were not statistically significant signs of DVT in the very elderly patients. In our study, the most common symptoms in both the groups were swelling and pain. In a study by Naess et al, DVT was described as originating in the left leg and then developing in the right leg, although DVT rarely occurred in both legs; in contrast, DVT was detected more often in the right leg in both the groups. 14 Our study was in agreement with Naess et al, as we found no statistical significance in the detection of DVT in the right leg, and we detected more proximal DVT in both groups but without statistical significance. In a previous study by Zhu et al, 15 the development of pulmonary embolism caused by DVT was detected in approximately 44% of cases. Likewise, in our study, pulmonary embolism was a common complication of DVT in both the groups. Further, we found that one-third of the deaths in the very elderly patients were caused by pulmonary embolism; however, in the study by Heit, 6 up to one-quarter of sudden deaths in all age-groups was caused by pulmonary embolism. Longo et al 16 observed that DVT was more frequently associated with pulmonary embolism and less frequently associated with neoplasms in elderly patients; further, they provided different data regarding the prevalence of DVT and sex differences. In the study by Longo et al, 16 more elderly patients had DVT with different clinical features, and no differences were found between males and females regarding the prevalence of DVT.
Frailty has been identified as a risk factor for DVT in the elderly patients in a previous study by Folsom et al. 17 However, we did not measure frailty in our study. Generally, frailty should be assumed to be more prevalent in the age-group studied herein. Folsom et al studied frailty based on weight loss, grip strength, feelings of exhaustion, walking time, and physical activity. 17 These parameters have not been considered in detail in our study. Further studies are needed to examine the relationship between frailty and DVT in the very elderly patients. Previous studies reported minor injuries as a risk factor for venous thrombosis, 18 this observation was made in our study in patients with contusions after a fall. Furthermore, a high prevalence of venous thromboembolism has been reported in patients with COPD. 19 Although no significant increased risk of DVT was found in patients with COPD in our study, acute inflammatory diseases appeared to be a risk factor for the development of DVT. Acute respiratory and urinary infections were also described as a risk factor for DVT in a study by Smeeth et al. 20 General acute inflammatory diseases could increase the risk of developing DVT in very elderly patients. An association was found between atherosclerosis and venous thrombosis in a previous study by Prandoni et al 21 ; this observation was made in patients with acute myocardial infarction in our study as well. A high risk of DVT was discovered in patients with heart failure in the study by Beemath et al. 22 These findings were also confirmed in very elderly patients with cardiac decompensation due to heart failure in our study. Generally, cancer is considered a risk factor for DVT. 23 –25 In our study, cancer was found only in the elderly patients in the control group who were diagnosed with both cancer and DVT, probably due to the fact that patients with cancer included in our study did not reach the age of 90 years or older. Recent studies have reported an increased risk of DVT in patients with lung fibrosis. 26 Accordingly, analysis of the data in our study indicates that an association between lung fibrosis and DVT might exist. However, further investigations are required to clarify this relationship.
A correlation has been implied between sepsis and DVT. 27 The incidence of sepsis in the study population with DVT was increased in our study, although further studies are warranted. Comparison of various comorbidities in groups with and without DVT showed an elevated incidence of hysterectomy, hyperthyroidism, arthritis, and decubitus ulcers in the elderly patients aged older than 80 years with DVT in our study. In agreement, data of the latest studies show that the incidence of venous thromboembolism rises after major cancer surgery such as hysterectomy, 28 as is the case in our study. Following a small number of published studies, it remains unclear whether hyperthyroidism leads to an increased risk of venous thromboembolism through modifications of the hemostatic system causing a hypercoagulable condition. 29,30 Recent developments in the interpretation of blood coagulation processes support an inflammatory origin, such as osteoarthritis and rheumatoid arthritis, for thromboembolic events. 31 These discoveries permit the administration of a pharmacological thromboprophylaxis in patients with osteoarthritis and rheumatoid arthritis. Finally, for the increased incidence of decubitus in patients with DVT, we could find no published data.
A negative
Study Limitations
This study examined very elderly patients diagnosed with DVT in one Department of Internal Medicine but did not investigate very elderly patients diagnosed with DVT in other medical departments. The differences in our descriptive results may be due to the age difference between both the groups and individual biological variations regarding limited life expectancy. Other limitations of this study include the small number of patients observed in the study group, the retrospective study design, and the single-center analysis.
Conclusions
The study group had no increased risk of DVT compared with the control group. The typical clinical symptoms of DVT may be absent in the very elderly patients. Common acute illnesses among the very elderly patients, such as congestive heart failure, respiratory and urinary infections, acute myocardial infarction, sepsis, atrial tachyarrhythmia, contusion, and pulmonary edema, increased the risk of DVT. Further, an increased risk of DVT was found for cancer, lung fibrosis, hysterectomy, hyperthyroidism, and arthritis. The
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.