
Abstract
Objective
To analyze independent risk factors for postoperative venous thromboembolism (VTE) in patients after thoracoscopic lobectomy and establish a risk model for predicting thrombosis.
Methods
We selected 135 patients who underwent thoracoscopic lobectomy and assigned them to a VTE group (n = 31) and a non-VTE group (n = 104) according to the presence or absence of postoperative VTE. Univariate and multivariate logistic regression models were built to identify independent risk factors for postoperative thrombosis. A nomogram to predict the risk of thrombosis was generated, with the predictive performance of the model being evaluated by plotting calibration curve and the receiver operating characteristic (ROC) curve.
Results
D-dimer on the first postoperative day and Caprini scores were independent high-risk factors for VTE after thoracoscopic lobectomy as revealed by univariate and multivariate logistic regression analyses (p < .05). The nomogram was evaluated, and the fitting degree of calibration curve indicated good accuracy of the model in predicting thrombosis. The area under the curve (AUC) value was 0.8654, suggesting favorable diagnostic efficacy of the model.
Conclusion
The D-dimer on the first postoperative day and Caprini scores were independent risk factors for VTE after thoracoscopic lobectomy. The nomogram that was generated to predict the risk of thrombosis had good accuracy and diagnostic efficacy, which can guide individual risk assessment and management decisions in clinical practice.
Introduction
Current treatments for lung cancer (LC) include surgical resection, immunotherapy, radiotherapy, and targeted therapy, among which pneumonectomy is the best option for patients with early-stage LC. 1 In the early 1990s, video-assisted thoracoscopic surgery (VATS) lobectomy was, for the first time, used for LC resection and became the gold standard for LC surgery as its safety and feasibility were confirmed by mounting clinical evidence. 2 Thoracoscopic lobectomy can relieve pain and accelerate recovery postoperatively in patients and is associated with lower complication rates, mortality, and costs into the bargain.3–5 Patients undergoing thoracoscopic lobectomy have a complication rate of 58% lower and an overall survival rate higher than those undergoing open lobectomy (p < .001).6,7 On this basis, thoracoscopic lobectomy is deemed safe and effective as a high-performance alternative to open lobectomy.
Thoracoscopic lobectomy is beneficial in many aspects, while postoperative complications may still occur to varying degrees. Venous thromboembolism (VTE) is a serious complication after thoracoscopic lobectomy,8,9 and patients with thrombosis are at high risk of critical symptoms including pulmonary embolism, infarction, or chronic thromboembolic pulmonary hypertension. As a case report presented, a patient with LC who underwent right lower lobectomy and mediastinal lymphadenectomy developed thrombosis in the right lower lobar pulmonary artery stump three months later. 10 A patient with small cell LC who underwent thoracoscopic left upper lobectomy experienced epigastric abdominal pain and vomiting 16 days later and then received a diagnosis of propagation of thrombus in the stump of the left superior pulmonary vein complicated with splenic infarction as shown by contrast-enhanced computed tomography (CT). 11 Additionally, Kitajima et al 12 reported a case of acute cerebral infarction due to stasis of blood flow in the left upper pulmonary vein stump around 30 h after the left upper lobectomy. Thrombosis is often implicated in poor outcomes. As demonstrated by Chen et al., 13 a lower survival rate was observed in patients with thrombosis than in those without thrombosis after pneumonectomy. In conclusion, thrombosis is prone to occur after thoracoscopic lobectomy and increases the risk of death in patients, thus high priority should be accorded in clinical practice. But studies on predicting the risk of thrombosis after thoracoscopic lobectomy are insufficient to fully elucidate risk factors.
In this study, the clinical data of patients who underwent thoracoscopic lobectomy at Dongyang People's Hospital from January 2017 to December 2022 were statistically analyzed to investigate the risk factors for postoperative VTE. A nomogram was generated in the combination of factors to predict the onset risk, so as to guide the stratification of high-risk patients for adopting effective prevention, diagnosis, and treatment, thereby accelerating postoperative recovery.
Methods
Subjects
Patients who underwent thoracoscopic lobectomy at Dongyang People's Hospital from January 2017 to December 2022 were selected. Information on clinical characteristics of patients was collected, including age, gender, blood type, body mass index (BMI), diabetes, hypertension, coronary heart disease, preoperative D-dimer, preoperative carcinoembryonic antigen (CEA), preoperative forced expiratory volume in 1 s (FEV1), Caprini score, operation time, surgical site, D-dimer on the first postoperative day, pathological type, and pathological stage. Patients who met the following inclusion criteria were deemed eligible: (1) patients were diagnosed as LC by pathological examination; (2) patients received thoracoscopic lobectomy; (3) patients received a diagnosis of postoperative thrombus by vascular ultrasound. Exclusion criteria included: (1) idiopathic thrombocytopenic purpura; (2) cerebral infarction or myocardial infarction in the past year; (3) perioperative use of anticoagulant drugs due to coagulopathy or other causes; (4) preoperative thrombosis; (5) incomplete clinical data. As per the inclusion and exclusion criteria, 135 patients who underwent thoracoscopic lobectomy were included and assigned to a VTE group (n = 31) and a non-VTE group (n = 104) according to the presence or absence of postoperative VTE.
Construction and Evaluation of Nomogram
The risk factors of thrombosis after thoracoscopic lobectomy obtained by multivariate logistic analysis were the basis of nomogram construction. Discrimination evaluation of the model was done by plotting receiver operating characteristics (ROC) curves and calculating the area under the curve (AUC). Regarding the calibration evaluation of the model, the calibration curve of the predicted complication probability by nomogram and the actual complication probability was plotted to validate the consistency of the model.
Statistics
Statistical analysis was performed on SPSS 24.0 software. Measurement data were expressed as mean ± standard deviation, and an independent sample t-test was used; enumeration data were expressed as N (%), and a chi-square test was used. Logistic regression model was established with risk factors at p < .1, and independent risk factors were determined. Univariate and multivariate logistic regression models were used for nomogram construction. The Caprini scores were calculated and summarized postoperatively based on the modified Caprini risk assessment model. p < .05 meant statistical significance.
Results
Patient Baseline Characteristics
135 patients who underwent thoracoscopic lobectomy were included and assigned to the VTE group and the non-VTE group according to the presence or absence of thrombosis. The baseline information of patients was listed in Table 1. Univariate analysis of patient clinical data presented significant differences in age, gender, coronary heart disease, surgical site, D-dimer on the first postoperative day, preoperative FEV1, and Caprini score between the two groups (p < .1). No significant differences were seen in other factors (p > .1).
Patient Baseline Characteristics.

*VTE: venous thromboembolism; BMI: body mass index; FEV1: forced expiratory volume in 1 s; CEA: carcinoembryonic antigen.
Note: The bold value indicates p < .05, which is statistically significant.
Results of Logistic Regression Analysis
By using variables with statistical differences between the two groups as independent variables and thrombosis as the dependent variable, multivariate logistic regression analysis was performed, and a logistic model was built:
Variables in the Logistic Regression Equation.
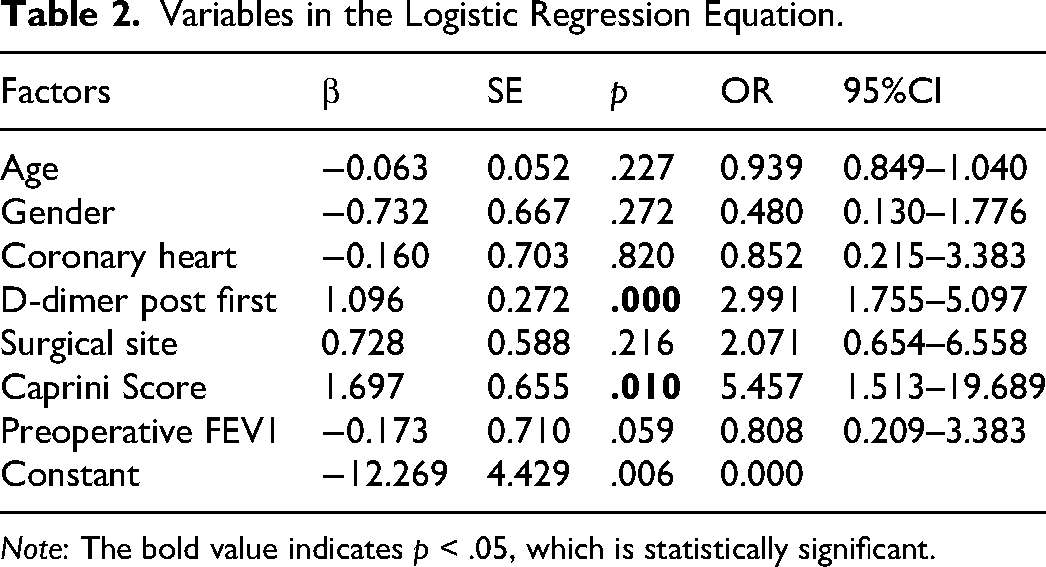
Note: The bold value indicates p < .05, which is statistically significant.
Establishment of a Nomogram for the Risk Model
A nomogram was developed to predict the risk of VTE after thoracoscopic lobectomy based on the logistic regression model (Figure 1). As depicted by the nomogram, the development of postoperative thrombosis was mostly affected by preoperative D-dimer, followed by Caprini score. The preoperative D-dimer and Caprini scores as single scores were calculated, and the total score was accumulated. The probability of postoperative thrombosis could be predicted according to the total score. The calibration curve of the nomogram was plotted and showed a tendency to be a standard curve, indicating that the predicted value was basically in line with the actual situation (Figure 2). As analyzed on the ROC curve, the AUC value was 0.8654, suggesting that the model had favorable accuracy and discrimination (Figure 3).
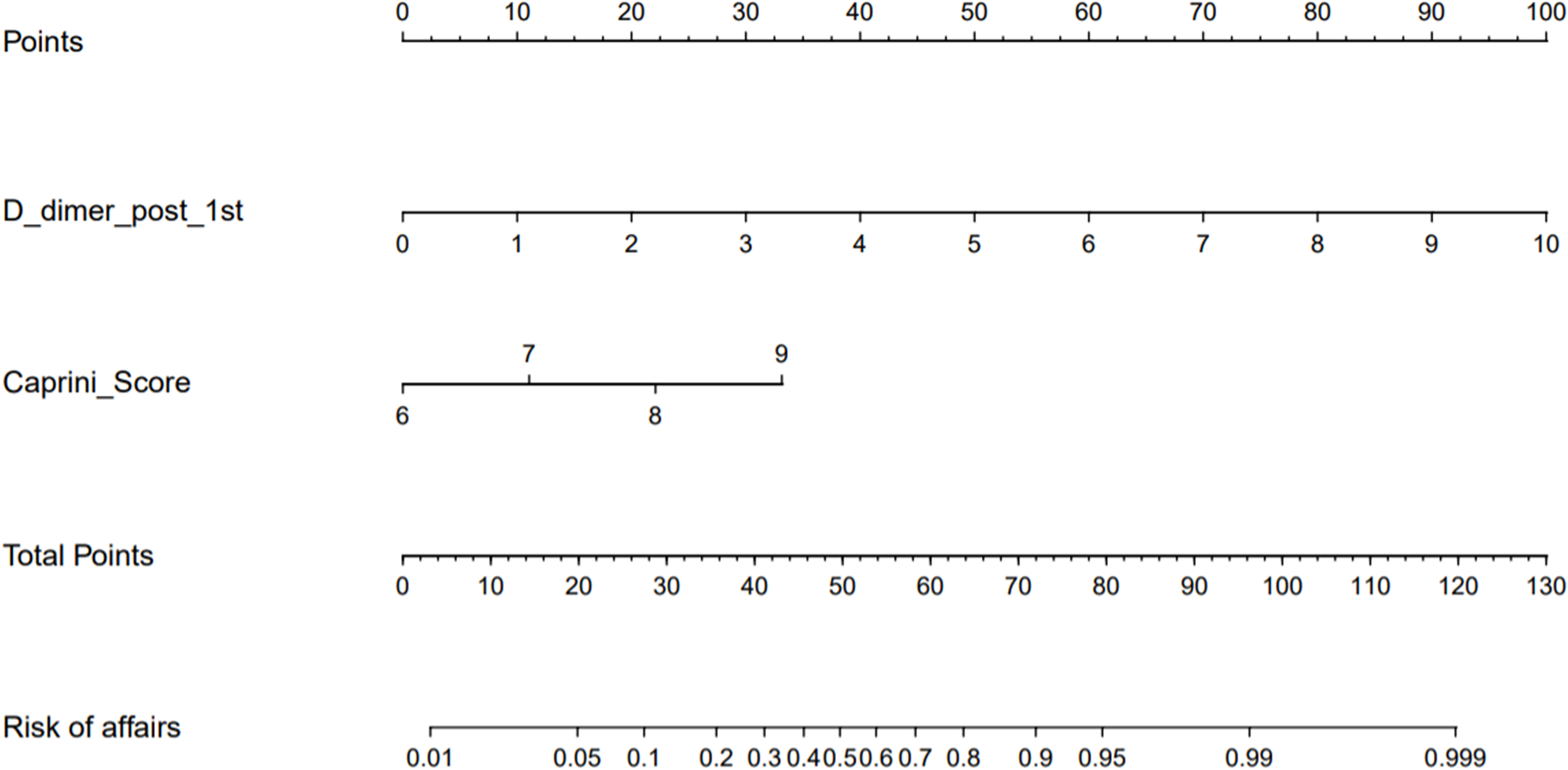
Nomogram of high-risk factors for thrombosis after thoracoscopic lobectomy.

Calibration curve of the nomogram.

ROC curve of the nomogram.
Discussion
Thoracoscopic lobectomy is the main approach for LC treatment and can achieve satisfactory clinical efficacy, but postoperative complications such as VTE are prone to arise. Risk factors for VTE include surgical approach, anesthesia, and patient stress.14,15 Clinical interests have grown up around the theme of causes of postoperative thrombosis after thoracoscopic lobectomy, but no consensus is reached on the independent risk factors for postoperative thrombosis after thoracoscopic lobectomy and its prevention. In this study, D-dimer on the first postoperative day and Caprini scores were independent risk factors for postoperative VTE after thoracoscopic lobectomy as identified by univariate and multivariate analyses.
D-dimer is associated with the prognoses of LC patients, and elevated postoperative serum D-dimer levels increase the risk of postoperative thrombosis in LC patients. Wang et al. 16 reported that up to 87.17% (523/600) of patients undergoing lung tumor surgery have postoperative VTE, and postoperative D-dimer levels differ substantially between the VTE group and the non-VTE group. Additionally, Yao et al. 17 confirmed that at 24 h after thoracoscopic surgery, hypercoagulation, and progressively elevated D-dimer are observed, but the impact is less than thoracotomy. D-dimer is the smallest fibrinolysis-specific degradation product known in the circulation, 18 and its elevated level is generally indicative of hypercoagulation and secondary hyperfibrinolysis. 19 Serial postoperative testing of D-dimer levels combined with risk factors associated with thrombosis allows well evaluation of VTE occurrence. Caprini score is a valid and reliable predictive tool for assessing the risk of thrombosis. Zhou et al. 20 revealed that the Caprini score identifies 84.3% of VTE cases, whereas the Padua Prediction score only identifies 49.1% of VTE cases, besides, the Caprini risk level is associated with in-hospital and 6-month mortality. Chen et al. 21 observed VTE in 10 of 117 patients who underwent pneumonectomy, and Caprini score is proportional to the VTE ratio, indicating the superior performance of Caprini score in predicting VTE. Thence, serial assessment of perioperative Caprini scores is effective in reducing the incidence of thrombosis and mortality of critically ill patients, improving patient prognosis and quality of life. 22 Together these findings confirm that D-dimer levels on the first postoperative day and Caprini scores can be key indicators for postoperative thrombotic screening, suggesting that a combination of these two indicators is highly sensitive for identifying patients who may benefit from prevention.
In this study, a predictive model was successfully constructed with D-dimer levels on the first postoperative day and Caprini scores on the basis of multivariate regression analysis. Meanwhile, the calibration curve and ROC curve suggested that the nomogram had favorable predictive performance and discrimination. Clinicians can stratify patients at high risk of postoperative thrombosis referring to this model and be prepared to take targeted preventive measures. High-risk patients are encouraged to receive regular checkups for early detection and treatment. A growing body of research is done on the prevention of postoperative thrombosis after thoracoscopic lobectomy. Chen et al. 23 determined that self-heating calf sleeves (SHCSs) prevent postoperative VTE in patients undergoing thoracoscopic lobectomy, and SHCS is a satisfactory prophylaxis method to improve venous blood flow and thus alleviate venous stasis in the lower extremities. Nakano et al. 24 reported that cases with thrombus formation in the pulmonary vein stump as shortened by ligating the pulmonary vein at the pericardial reflection after left upper lobectomy are substantially fewer than those not treated with the ligation method (p = .010), demonstrating that the proximal ligation method is markedly linked to less thrombus formation in the pulmonary vein stump. Thus, stratifying patients at high risk for postoperative thrombosis after thoracoscopic lobectomy facilitates the implementation of prevention measures and reduces patient harm and economic burden.
Taken together, D-dimer level on the first postoperative day and Caprini score are independent risk factors for VTE after thoracoscopic lobectomy. In this study, the predictive model shows good accuracy and discrimination and is beneficial for clinical screening of high-risk groups, thus interventions can be taken correspondingly to improve patient prognosis. This model is valuable in clinical applications. However, this study still has some limitations. This study is a single center, retrospective study, which may have bias. Secondly, the limited sample size and the lack of external validation of the nomogram allow unavoidable errors. A multi-center, large sample-size clinical study is ongoing to optimize and validate the model.
Footnotes
Authors’ Contributions
(I) Conception and design: Junkai Qiao. (II) Administrative support: Yueming Wu. (III) Provision of study materials or patients: Yueming Wu. (IV) Collection and assembly of data: Jiang Feng. (V) Data analysis and interpretation: Weiwei Hu. (VI) Manuscript writing: Junkai Qiao. (VII) Final approval of manuscript: All authors.
Availability of Data and Materials
The data and materials in the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Ethical approval to report this case was obtained from Dongyang People’s Hospital (2020-YX-077).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Dongyang Municipal Science and Technology Program (grant number 20-323).
Informed Consent
Written informed consent was obtained from a legally authorized representative for anonymized patient information to be published in this article.
Correction (May 2023):
The funding and Introduction text has been edited slightly since its original publication.