
Abstract
Chronic thromboembolic pulmonary hypertension (CTEPH) is an ominous disease leading to progressive right heart failure. Selected patients can be treated by pulmonary endarterectomy (PEA). We assessed long-term clinical outcome of patients with CTEPH who underwent PEA and patients who remained on medical treatment alone. A total of 112 consecutive patients with CTEPH referred between 1998 and 2008 to one center were followed for a mean of 35 (range 0-128) months after diagnosis. All the patients had advanced pulmonary hypertension at baseline. The operated group had higher World Health Organization functional class compared to the nonoperated group. No other differences in hemodynamic, echocardiographic, or biochemical parameters were observed at baseline. Despite the perioperative mortality rate of 9.1%, patients who underwent PEA had significantly lower long-term mortality compared to nonoperated patients (12.7% vs 34.8%; P = .003), and PEA survivors showed sustained clinical improvement. All efforts should be undertaken to perform PEA in all patients with operable CTEPH.
Keywords
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is a relatively rare but clinically important group classified as group 4 of pulmonary hypertension (PH). It has a very poor outcome if left untreated because of progressive right heart overload and failure. 1 –3 Pulmonary endarterectomy (PEA) has been considered as treatment of choice. 4,5 It can provide dramatic improvement in symptoms and restore life expectancy to normal. However, PEA is a difficult procedure. It requires long periods of cardiopulmonary bypass and intermittent complete cardiac arrest with deep hypothermia. The decision about operability is made by a multidisciplinary team consisting of an experienced cardiac surgeon, a cardiologist or pulmonologist, and a radiologist. 5 Operability depends not only on the location of intravascular lesions but also on comorbidities, functional class, and hemodynamics. Because of complexity of PEA, some patients are reluctant to accept the risk of surgery. We tried to assess prognostic markers and outcomes according to the treatment selected for patients with CTEPH diagnosed at our center.
Materials and Methods
Study Population
We analyzed the outcome of consecutive patients diagnosed with CTEPH at the Department of Chest Medicine at Institute of Tuberculosis and Lung Diseases, Warsaw, Poland, between June 1998 and May 2008. In all cases, PH was confirmed by right heart catheterization. Thromboembolic etiology of PH was confirmed when organized thromboembolic material in pulmonary arteries was revealed by computed tomography pulmonary angiography or/and conventional pulmonary angiography. At baseline World Health Organization (WHO) functional class, arterialized capillary blood gasses, lung function tests, spiral computed tomography with both contrast enhancement and high resolution assessment, transthoracic echocardiography, right heart catheterization, and 6-minute walk test were performed. N-terminal probrain natriuretic peptide (NT-proBNP) levels and troponin T levels in were measured in 82 and 85 patients, respectively.
Pulmonary Endarterectomy
All patients with CTEPH were discussed by a multidisciplinary team consisting of a cardiologist/pulmonologist, experienced radiologist, and PEA cardiac surgeon. When the decision to operate was made, PEA was performed in the Department of Cardiac Surgery, Institute of Cardiology in Warsaw according to San Diego technique using deep hypothermic circulatory arrest. 6,7 An inferior vena cava filter was placed in the vena cava inferior in 53 (80.3%) operated patients before the PEA procedure. During the period covered by the trial, targeted therapy was not used in those patients.
Medical Treatment
Forty-six patients who were not suitable for surgical treatment or who refused surgical treatment remained on conventional medical treatment (MT) including anticoagulants, diuretics, and oxygen, as appropriate. Of them, 20 (43.5% of nonoperated patients) received off-label targeted MT in monotherapy sildenafil, bosentan, iloprost, or treprostinil. Targeted MT was introduced according to the current availability of specific drug in the center.
Follow-Up
Patients had a follow-up visit at a median of 1 year after PEA or, in the case of patients from the MT group, after baseline hospitalization. The WHO functional class, exercise capacity, 6-minute walk distance, and transthoracic echocardiography were reassessed.
Statistical Analyses
Data were analyzed with the SAS software package version 9.1. The normality of distribution of variables was analyzed by the Kolmogorov-Smirnov test. Quantitative variables with normal distribution were presented as mean ± standard deviation (SD), otherwise as median and range.
For categorical variables, the differences were compared by chi-square test. For continuous variables, Student t test was used when normal distribution of variables was present and the Wilcoxon rank-sum test (Mann-Whitney U test) when distribution was not normal. Hemodynamic parameters in the operated group and noninvasive parameters in both the groups were assessed at baseline and at follow–up, and their values were compared in the follow-up by an analysis of paired samples. The P value of <.05 was interpreted as statistically significant. The proportion of patients surviving was estimated by the Kaplan-Meier method. The operated and nonoperated groups were compared by the log-rank test. Univariate and multivariate Cox proportional hazard analyses for selected variables from baseline were preformed to identify factors that are independently related to all-cause mortality. Results were presented as hazard ratio and 95% confidence interval.
Ethical Approval
The study was approved by the local ethical committee at the Institute of Tuberculosis and Lung Diseases, Warsaw, Poland, number KE-70/2007.
Results
From June 1998 to May 2008, 112 consecutive patients diagnosed with CTEPH were enrolled for the observation. Sixty-six (59%) patients underwent PEA and 46 (41%) remained on MT alone. The main reason why patients were not operated (Figure 1) was a distal location of thromboembolic material in pulmonary arteries, not accessible for surgery (n = 29; 63%). Other causes included death before a scheduled operation (n = 1, 2%), lack of patient’s consent (n = 6; 13%), and perceived increased surgical risk related to comorbidities, as assessed after considering the experience of surgical and anesthesiologic team at the time of qualification (n = 10; 22%). Comorbidities included chronic obstructive pulmonary disease (COPD; n = 1), uncontrolled hyperthyroidism (n = 1), immune-mediated hemolytic anemia with cold agglutinins (n = 1), antiphospholipid syndrome with thrombocytopenia (n = 1), severe obesity (n = 2), and cachexia (n = 1). Three patients were not operated on because of advanced age and concomitant left ventricular failure (n = 1), obesity (n = 1), and epilepsy (n = 1), respectively. All patients with comorbidities were clinically stable and completed all the standard elements of CTEPH evaluation, including right heart catheterization and 6-minute walk distance test. Among the operated patients 55 (83%) of the 66 had comorbidities: history of myocardial infarction 5 (7.6%), coronary artery disease 14 (21.2%), COPD 8 (12.1%), arterial hypertension 22 (33.3%), obesity 12 (18.1%), valvular heart disease 9 (13.6%), diabetes mellitus 4 (6.0%), thrombophilia 6 (9%), and hyperlipidemia or antihyperlipidemic therapy 32 (52.5%). Of them, 7 (10.6%) required additional concomitant procedure further increasing the risk of PEA surgery: coronary artery bypass graft (n = 4), mitral valve surgery (n = 2), and tricuspid valve surgery (n = 1).
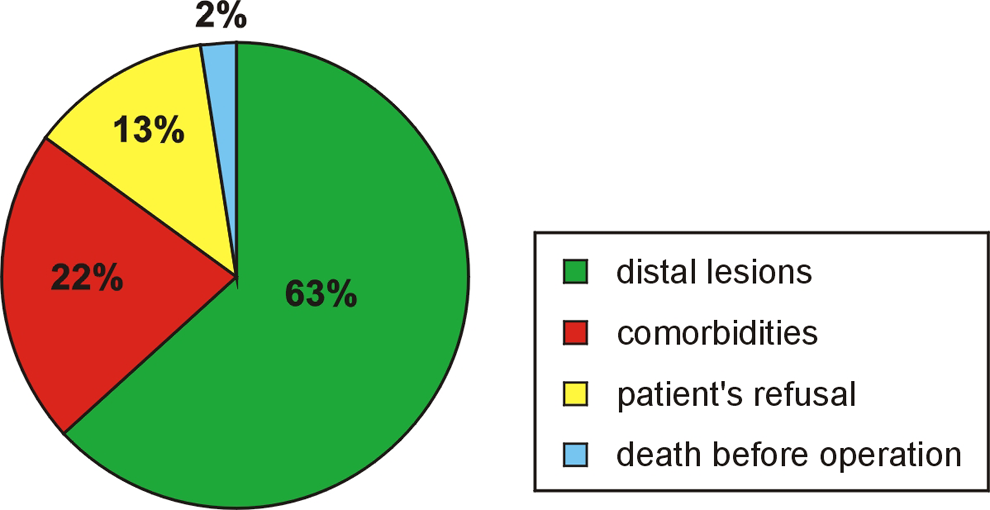
The causes of patient disqualification from pulmonary endarterectomy.
Characteristics of patients are presented in Table 1. Age was similar in PEA and MT patients. There were 75 men and 37 women among patients with CTEPH as a group. Patients with CTEPH had advanced PH and right ventricular dysfunction at baseline. The patients in the operated group had worse WHO functional class compared to those in MT group. In all, 55 (83.3%) ultimately operated patients had WHO functional class III or IV compared to 28 (60.9%) patients in the nonoperated group; P < .05. There were no other differences between both groups in clinical, hemodynamic, echocardiographic, and biochemical parameters at baseline. The operated group had more patients with a history suggesting acute pulmonary embolism (74% vs 57%, P < .05) and deep venous thrombosis (76% vs 54%; P = .001). An inferior vena cava filter was placed into the vena cava inferior in 53 (80.3%) patients before PEA and in 10 (21.7%) nonoperated patients (P < .0001). Nobody from the operated group received targeted therapy before PEA. Of the nonoperated patients, 20 received off-label targeted MT in monotherapy: bosentan (n = 9), sildenafil (n = 8), treprostinil (n = 2), and iloprost (n = 1).
Baseline Clinical Characteristics, Exercise Capacity, Hemodynamic, Echocardiographic Data in Patients With CTEPH, and a Comparison Between the Operated and Nonoperated Group.
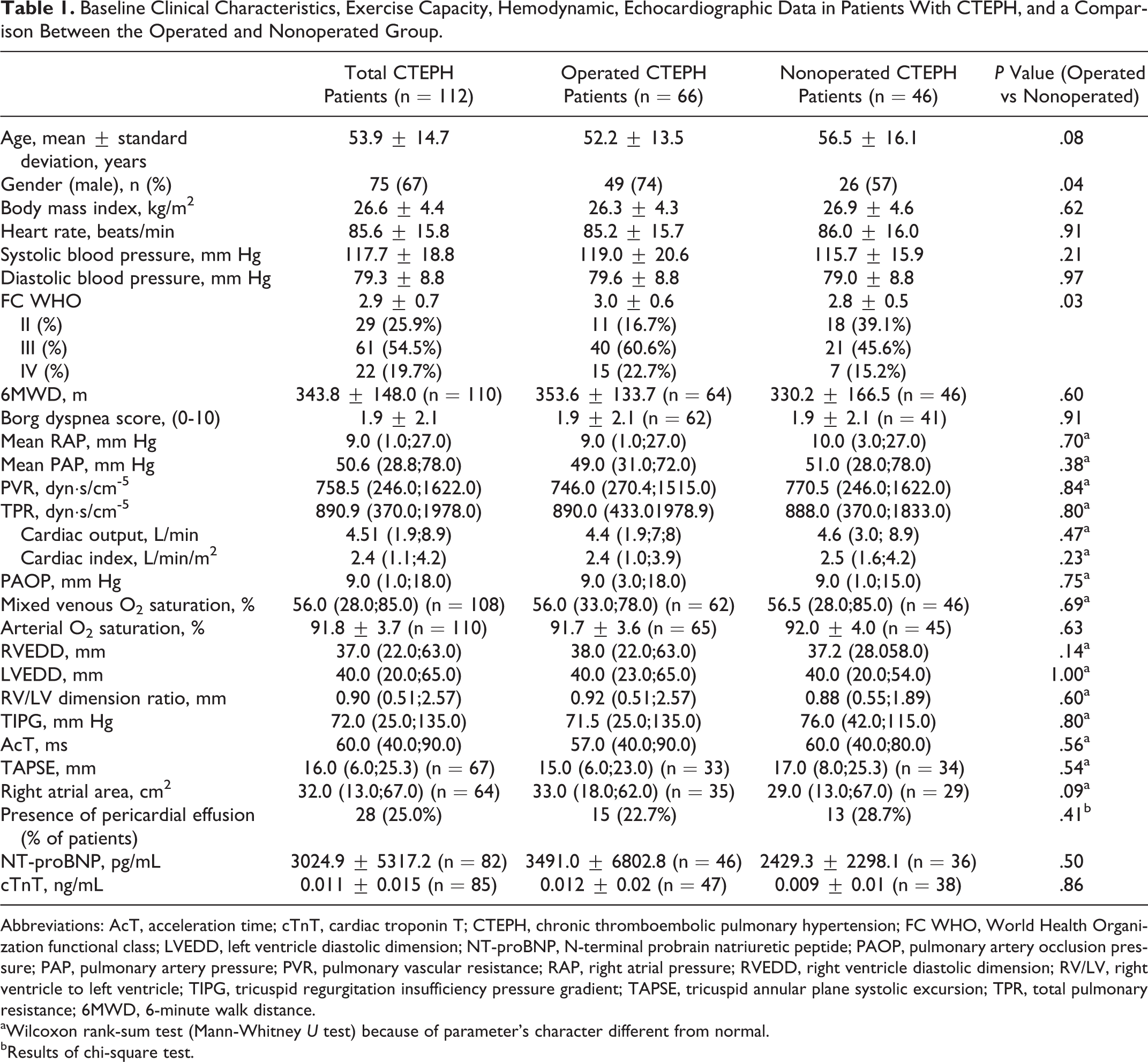
Abbreviations: AcT, acceleration time; cTnT, cardiac troponin T; CTEPH, chronic thromboembolic pulmonary hypertension; FC WHO, World Health Organization functional class; LVEDD, left ventricle diastolic dimension; NT-proBNP, N-terminal probrain natriuretic peptide; PAOP, pulmonary artery occlusion pressure; PAP, pulmonary artery pressure; PVR, pulmonary vascular resistance; RAP, right atrial pressure; RVEDD, right ventricle diastolic dimension; RV/LV, right ventricle to left ventricle; TIPG, tricuspid regurgitation insufficiency pressure gradient; TAPSE, tricuspid annular plane systolic excursion; TPR, total pulmonary resistance; 6MWD, 6-minute walk distance.
aWilcoxon rank-sum test (Mann-Whitney U test) because of parameter’s character different from normal.
bResults of chi-square test.
Patients were followed for a maximum of 10.7 years. In the whole group, 27 of the 112 patients died during follow-up. Total mortality rate was 24.1%. Despite worse WHO functional class at baseline, the patients who underwent PEA had better survival compared to those who remained on MT alone (Figure 2).
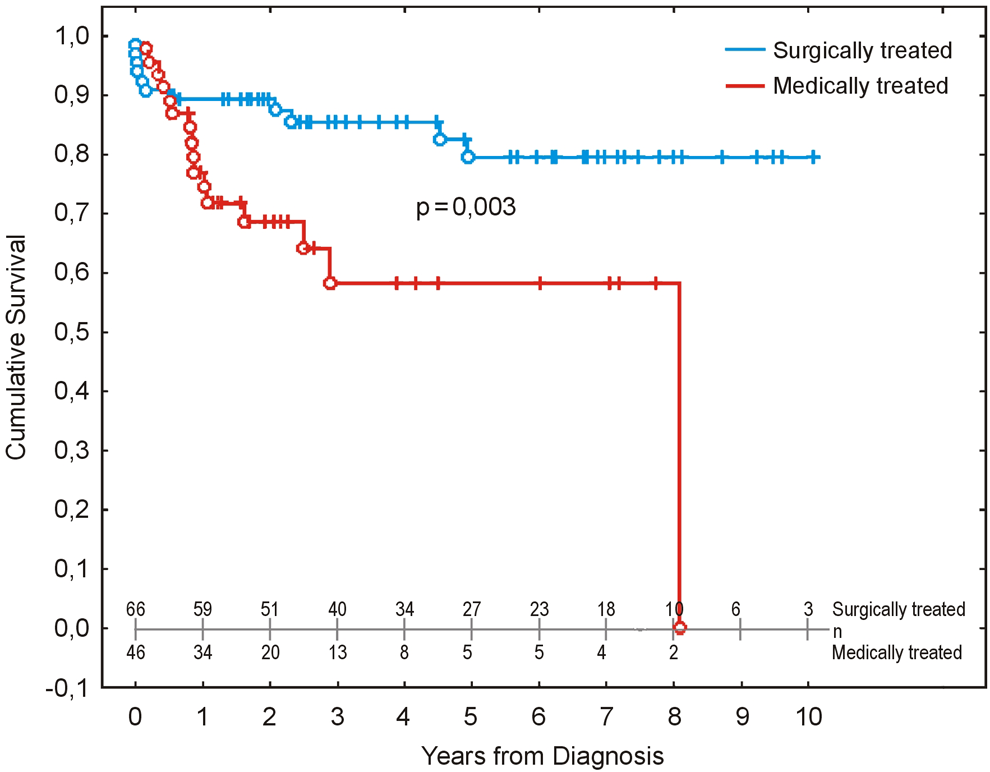
Kaplan-Meier survival curves for patients with chronic thromboembolic pulmonary hypertension who did and did not undergo pulmonary endarterectomy.
Outcome in PEA Patients
In PEA group, 11 (16.7%) of 66 patients died during follow-up. After PEA, 6 patients died before leaving the hospital: 3 patients (on days 2, 4, and 7 after operation) because of inefficient surgery and persistently high pulmonary vascular resistance (PVR), 1 patient (on day 3) because of reperfusion edema, 1 patient (on day 35) because of septic shock, and 1 patient (on day 51) because of severe hemorrhage from the respiratory tract requiring right inferior lobectomy. The in-hospital mortality was 9.1%. During long-term follow-up, 5 patients died because of persistent PH and progressive right heart failure (n = 3), biventricular heart failure (n = 1), and peritonitis and septic shock not associated with PEA (n = 1). One-year mortality rate was 9.1% and was associated with perioperative complications, while 3-year mortality was 12.7%.
Outcome in Medically Treated Patients
In the MT group, 16 (34.8%) of 46 patients died during follow-up, including 1 patient awaiting surgical treatment. The main cause of death was progressive right ventricle dysfunction (12; 75%). One (6.2%) patient died because of right and left heart failure; there were 3 (18.7%) sudden deaths, which could be associated with severe CTEPH. One-year mortality rate was 21.7% and 3-year mortality rate was 32.6%. Nonoperated patients who received targeted MT showed trend for better survival compared to MT patients on supportive therapy alone .
Prognostic Factors
An univariate Cox proportional hazard analysis (Table 2) revealed that PEA was among factors related to lower mortality in the observed CTEPH population. An advanced WHO functional class of IV versus II or III, worse hemodynamic parameters, the presence of pericardial effusion, and right ventricular end-diastolic dimension in echocardiography at baseline were risk factors for death. A multivariate analysis identified PEA as an independent factor for improved survival, while WHO functional class IV versus II, the mean right atrial pressure (RAP) at baseline ≥9 mm Hg, and the presence of pericardial effusion all contributed to increased mortality.
Univariate and Multivariate Analyses of Variables Associated With Mortality in the Whole Population of Patients With CTEPH.
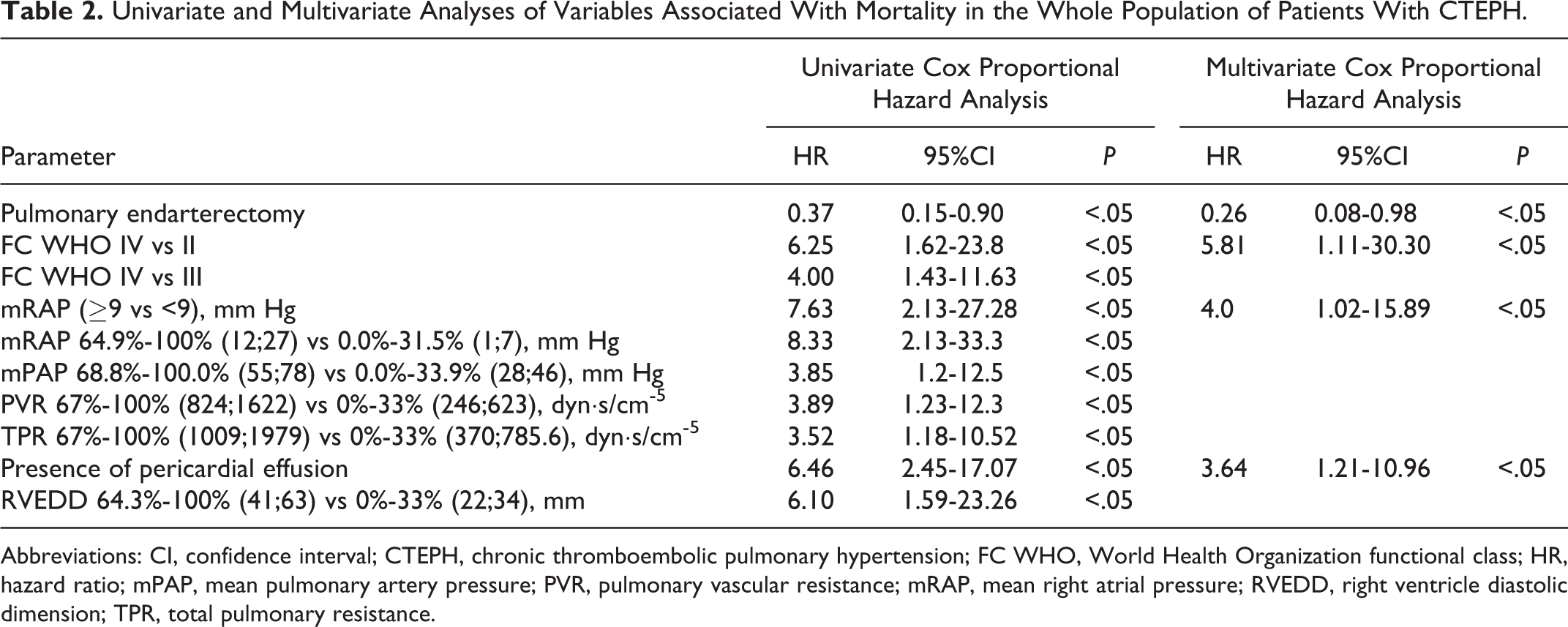
Abbreviations: CI, confidence interval; CTEPH, chronic thromboembolic pulmonary hypertension; FC WHO, World Health Organization functional class; HR, hazard ratio; mPAP, mean pulmonary artery pressure; PVR, pulmonary vascular resistance; mRAP, mean right atrial pressure; RVEDD, right ventricle diastolic dimension; TPR, total pulmonary resistance.
Hemodynamic Assessment in the Operated Group
All hemodynamic parameters measured directly after PEA showed significant improvement. Mean pulmonary pressure (mPAP) decreased from 49.9 ± 8.8 to 24.6 ± 7.4 mm Hg (P < .0001) and PVR decreased from 752.0 ± 242.5 to 176.2 ± 128.4 dyn s/cm-5 (P < .0001) while cardiac output increased from 4.5 ± 1.0 to 5.7 ± 1.5 L/min (P < .0001). Persistent PH after PEA defined as PVR of ≥400 dyn s/cm-5 or a decrease in PVR by less than 50% from baseline was present in 4 (6.1%) operated patients.
Noninvasive Assessment at Follow-Up
Noninvasive assessment was repeated at least 6 months after baseline assessment in the nonoperated group (n = 35) and at least 6 months after PEA in the operated group (n = 60). Six patients from the operated group and 11 from the MT group died before the follow-up visit.
Patients who survived PEA (n = 60) had significant improvement in WHO functional class at follow-up (3.0 ± 0.6 SD vs 2.5 ± 0.5 SD, P < .005; Figure 3A). In the MT group, a trend for clinical deterioration in WHO functional class was observed (Figure 3B). After PEA, 6-minute walk distance increased by 121 m compared to baseline, contrasting with the trend to decrease which was observed in MT group (Figure 4).
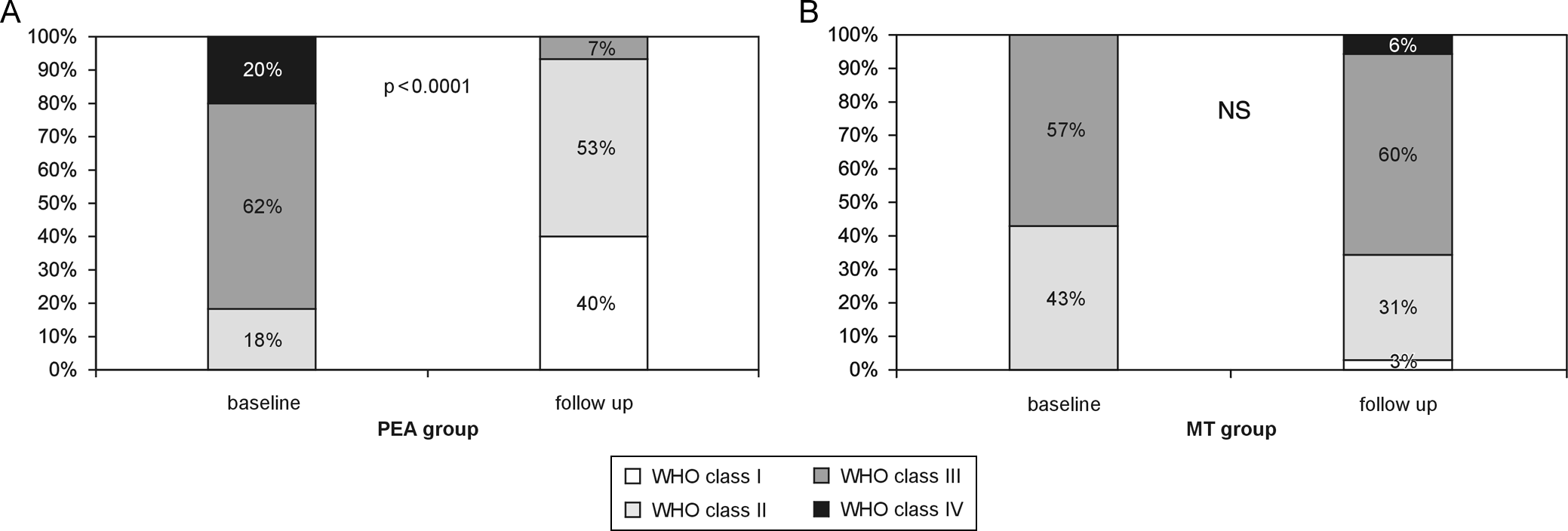
Functional World Health Organization (WHO) class changes in both operated (A) and nonoperated (B) patients with chronic thromboembolic pulmonary hypertension.
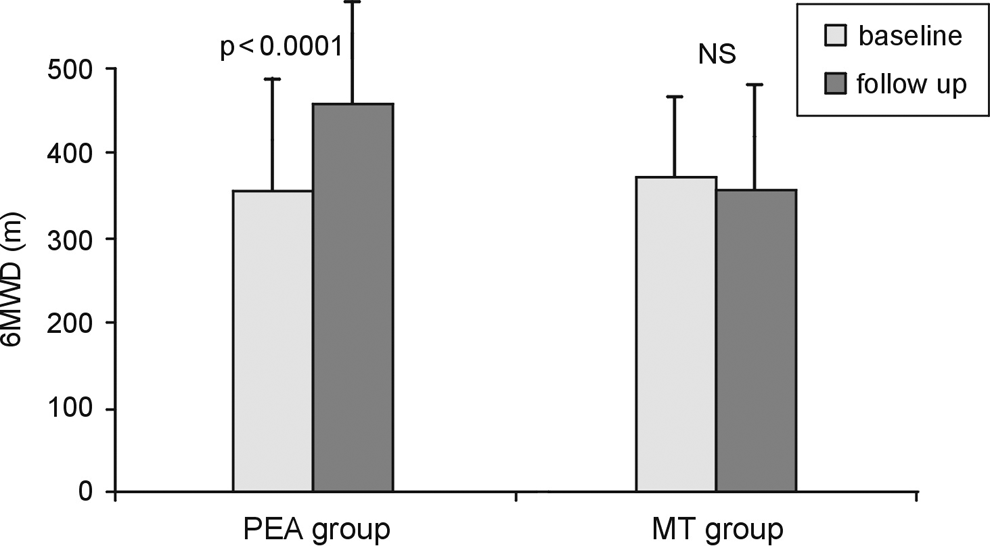
Six-minute walk distance (6MWD) changes among the patients with chronic thromboembolic pulmonary hypertension, in 2 groups, who underwent pulmonary endarterectomy and medically treated.
Echocardiographic parameters of right ventricular dysfunction improved significantly at follow-up in the operated group, while persisted in the MT group. Persistent PH defined at echocardiography as tricuspid insufficiency pulmonary gradient ≥ 46 mm Hg was present in 6 (11%) of the 54 operated patients and 4 (66.7%) of the 6 patients died because of right heart failure. In the MT group, all the patients had persistent PH with a tendency for progression.
Not all patients had NT-proBNP levels measured prior to the operation because until 2002, this was not possible in our center. In the 33 operated patients who were tested a significant decrease in NT-proBNP levels from 3588.9 ± 7909.7 to 1024.1 ± 3703.5 pg/mL was observed after PEA (P < .0001). In the MT group, 29 patients were tested and high levels of NT-proBNP persisted at follow-up (2037.6 ± 2053.4 pg/mL at baseline and 2357.9 ± 2146.1 pg/mL at follow-up, P = not significant).
Discussion
This study is based on a single-center, real-life, long-term observation of patients with CTEPH regardless of the mode of initial treatment. The most clinically relevant result is the significant improvement in survival in patients treated by PEA compared to MT alone.
Some earlier reports have demonstrated that PEA improved survival, functional class, and hemodynamic parameters compared to those in a historical control group. 8 –12 Our study compared both the operated and the nonoperated groups within the same recruiting period and confirmed better survival in patients who underwent PEA. Although one would expect such difference in a nonrandomized trial to be at least partly due to clustering of the older, more hemodynamically compromised patients, with more comorbidities in the MT subgroup this was not the case. Different from previous reports, in which operated patients were younger than nonoperated ones, 13 –15 the age of patients in both the groups was similar in our series. Patients at advanced age were more carefully qualified for PEA, but advanced age was not considered by us as a contraindication for this procedure. 4 In contrast to previous observations, 8,9,12,14 –17 there were no differences in 6-minute walk distance, weight, comorbidities, or associated medical conditions between the PEA and the MT groups. Both groups had the same hemodynamic, echocardiographic, and biochemical signs of right ventricle overload and dysfunction at baseline, while WHO functional class was even higher in patients assigned to PEA. We conclude that in our series, the decision in favor of surgery in most cases depended on the location of thromboembolic material and its expected accessibility by the surgeon, not on the severity of CTEPH, age, or comorbidities. A history of acute pulmonary embolism and deep venous thrombosis was more often present in operated than in MT patients, and this observation is in agreement with the recent studies. 13,15,18 It had been described that thromboembolic material more often occupied central pulmonary arteries in patients with symptomatic acute pulmonary embolism and recurring thromboembolic events.
The survival benefit of PEA was noted despite an average 9.1% surgical in-hospital mortality rate calculated at our center between 1998 and 2008. Such level of risk is compatible with previous reports from various centers where it ranged from 4.4% to 16% 7,9,10,14,19 as well as with European Society of Cardiology guidelines definition of experienced CTEPH surgical center. Such a center should have perioperative mortality rate of less than 10.0%. 20 The perioperative mortality rate in our center dropped from 9.7% in the period of 1998 to 2004 to 6.3%, between 2004 and 2008, which reflect growing an improved PEA technique, a better qualification process for the procedure, and better perioperative treatment. A similar observation was made in other centers, including the most experienced center in San Diego, where the mortality rate was 20% before and 4.5% after 2004, respectively. 7,21 In a recently published prospective registry containing PEA outcome data from 26 European and 1 Canadian CTEPH expert centers, including ours, mean in-hospital mortality of patients diagnosed after 2007 dropped further to 4.7%. 19 Thus, the survival benefit of PEA over MT may continue to increase with time in individual centers due to better surgical and perioperative management.
Persistent PH was found in 6.1% of operated patients directly after the operation and in 11.1% at follow-up, which is consistent with other observations after PEA. 22 –24 High baseline PVR was related to mortality in short- and long-term follow-up in univariate but not in multivariate analysis.
The prognosis for MT patients with CTEPH without PEA was unfavorable. The main cause of death was progressive right ventricular dysfunction and insufficiency. In the MT group, the total mortality rate was 34.8% during 2.2 years of follow-up and was significantly higher than that in the PEA group. This mortality rate was comparable to that in other observations. 2,3,14 Riedel et al showed that the mortality rate of MT patients with CTEPH having mPAP >30 mm Hg was 30% during a 2-year period and Lewczuk et al reported 50% mortality rate during 18.7 months of follow-up. In our group, all nonoperated patients had mPAP above 30 mm Hg.
In the last decades, several novel therapies targeted specifically to improve pulmonary circulation have been developed and successfully used to treat pulmonary arterial hypertension. Some prospective trials showed that targeted MT including 3 main groups of drugs was effective in improving hemodynamics and also the clinical status in patients with CTEPH, 25 –28 but still there is no evidence that targeted MT prolonged survival in patients with CTEPH. 15,17 In our study, 43.5% of patients in the nonoperated group received off-label targeted MT in monotherapy with a trend toward improved survival comparable to that observed in other studies. 14,15,17
In our observation, PEA was an independent favorable prognostic factor in CTEPH both in univariate and in multivariate analyses. Nonoperated patients had a 2.7 times higher mortality risk than patients who underwent PEA. Similarly, Bonderman et al showed PEA to be an independent positive prognostic factor for survival in patients with CTEPH. 14
In our observation of the whole group of patients with CTEPH, a multivariate analysis revealed that only RAP ≥9 mm Hg was a negative prognostic factor. Condliffe et al showed that RAP >10 mm Hg increased the mortality risk by 2.1, Saouti et al indicated that RAP >12 mm Hg was a predictor of death in nonoperated CTEPH patients. 15,17 In a study by Bonderman et al, only a high PVR was a risk factor for mortality in patients with CTEPH. 14 Unlike Bonderman et al 14 but similarly to Saouti et al, 17 we did not confirm that conditions associated with CTEPH (splenectomy, osteomyelitis, colitis, central venous catheterization, or atrioventricular shunt) were prognostic factors in MT patients. The presence of pericardial effusion at baseline was a factor for worse survival in the whole group of patients. The presence of pericardial effusion is a known risk factor for unfavorable prognosis in pulmonary arterial hypertension, with the mortality rate increasing proportional to the amount of fluid in the pericardium. 29
Chronic thromboembolic PH is characterized by progressive impairment of exercise capacity caused by right ventricular dysfunction due to increasing PVR. 5 At baseline, majority of our patients were in WHO functional class III or IV with worse profile among MT patients. The functional class improved significantly after PEA while tended to worsen in the MT group. Similar observations were made for NT-proBNP in patients in whom those data were available and for echocardiographic parameters.
Trial Limitations
Our analysis has limitations of an observational study, mainly the selection bias of surgical candidates. It is impossible to completely eliminate the existence of bias in such studies. Patients who undergo surgery are generally those in better hemodynamic and general conditions, with less comorbidities. Theoretically, this might have adversely influenced the prognosis of MT patients in our trial. Particularly, comorbidities among causes of surgical disqualification in 10 of the 46 patients deserve a comment. Despite the fact that similar prevalence and type of comorbidities were also present in the PEA group, it is possible that they were more severe in MT patients and could represent a potential cause of more frequent adverse outcome. However, the most common cause of death in MT patients was progressive right ventricular failure or sudden death and not problems related to specific comorbid conditions. In our patients, comorbidities were not perceived as severe enough to limit life expectancy, but predominantly as factors creating excessive perioperative risk, considering experience of the anesthesiology team at the time of evaluation for PEA. Most of the patients with comorbidities among the MT group would be qualified by our team for PEA, if surgery would be considered in 2014 and not between 1998 and 2008. Finally, the most universal so far prognostic factor in nonoperated CTEPH, that is, WHO functional class which to some degree was probably affected by comorbididties, was significantly worse in PEA than in MT, which should have resulted in better survival of MT patients.
In summary, although some differences existed between PEA and MT groups, it seems unlikely that they were driving the observed, striking difference in survival. Indeed, somewhat unexpectedly, we had faced a quite well-balanced baseline characteristics of the PEA and MT groups, offering a chance to directly compare their outcome, which would not be possible in a frame of a randomized trial due to ethical reasons.
The relatively long inclusion period of 10 years, during which the management protocols, indications for surgery, expertise of the surgical team, perioperative management, and targeted therapeutic options have been evolving, can be considered as another trial limitation. We were unable to account for those changes. Systematic evaluation for the presence of thrombophilia was not performed, but this should not have a major impact on the results as all patients were chronically anticoagulated since the moment of diagnosis.
Conclusions and Clinical Implications
The long-term prognosis in patients with advanced-stage CTEPH who remained on MT alone is unfavorable compared to that in patients who underwent PEA. Pulmonary endarterectomy reduced the mortality risk in the whole group of patients with CTEPH. In our observation, operated patients were not preselected according to the stage of their disease because there were no differences between operated and nonoperated groups in terms of clinical, hemodynamic, echocardiographic, or biochemical parameters at baseline except worse functional WHO class in the PEA group. An advanced WHO functional class, the presence of pericardial effusion in echocardiography, and elevated mean RAP at hemodynamic evaluation increased the mortality risk in the whole group of patients with CTEPH.
Our observations demonstrated that PEA leads to marked and sustained improvement in clinical, hemodynamic, and echocardiographic indices in survivors, with acceptable perioperative mortality rate, compared to patients who were not operated (irrespective of the reason). This fact should be carefully considered while making therapeutic decisions in patients with CTEPH. All efforts should be undertaken to perform PEA in all patients with operable CTEPH. Survival curves constructed based on local follow-up data should be created in all CTEPH centers. They may be helpful in discussing management strategies with patients who might be reluctant to accept relatively high perioperative risk of PEA. Moreover, our data on long outcome may serve as a reference for emerging treatment methods in CTEPH, like percutaneous transluminal angioplasty in distal postthromboembolic pulmonary arterial occlusions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by institutional grants of The Ministry of Science and Higher Education, Poland, number: NN 402 080834.