
Abstract
Pulmonary hypertension (PH) is a fatal disease although significant improvements in treatment are achieved. Easily implemented and noninvasive prognostic techniques are needed while following-up these patients. The aim was to investigate the role of fractional exhaled nitric oxide (FeNO) in follow-up for patients with PH. In this longitudinal study, patients with pulmonary arterial hypertension (PAH) and chronic thromboembolic PH (CTEPH) who were seen in PH Outpatient Clinic, Istanbul Faculty of Medicine, Istanbul University, were enrolled in the study. Echocardiography, 6-minute walking test, brain natriuretic peptide, and FeNO measurements were performed, and World Health Organization functional class was evaluated to all patients at baseline, and third, and sixth months. Right-heart catheterization and pulmonary function tests at the time of diagnosis were recorded. The study comprised 31 patients (23 women, 8 men; mean age: 53.4 ± 17.1 years) with PAH (n = 19) and CTEPH (n = 12) and 80 healthy controls. Patients with PH had lower FeNO values than the control group (16.5 ppb vs 19.8 ppb; P < .05). Fractional exhaled nitric oxide values did not change during follow-up and did not correlate with other follow-up measures except tricuspid annular plane systolic excursion values. Fractional exhaled nitric oxide was higher in the idiopathic PAH subgroup at baseline and at third month than patients with PAH associated with other diseases. Fractional exhaled nitric oxide did not change in patients who had clinical deterioration. As a conclusion; Patients with PH had lower FeNO values than healthy controls, but FeNO did not change significantly during follow-up. Large-scale studies with prolonged follow-up periods are needed to understand the role of FeNO in the follow-up of the patients with PH.
Keywords
Introduction
Pulmonary hypertension (PH) is a group of diseases that involves pulmonary small vessels and can be seen secondary to various diseases, which results in an increase in pulmonary arterial pressure and narrowing of pulmonary blood vessels. 1 –3 The imbalance between vasoconstrictors, thromboxane and endothelin, and the vasodilators, prostacyclin and nitric oxide, results in vasoconstriction. 4 Pulmonary hypertension is defined as an elevation in the mean pulmonary arterial pressure ≥25 mm Hg as measured using right-heart catheterization. 1,2 The treatment goals of PH are based on the basal and follow-up measurements of the prognostic parameters such as brain natriuretic peptide (pro-BNP), 6-minute walk test (6MWT), functional class, and echocardiographic findings. However, these tools are not adequate for decision-making about prognosis. Therefore, easily applicable, noninvasive prognostic determinants are still needed for the follow-up of patients with PH.
Nitric oxide (NO) is synthesized as a potent vasodilator in various cells in the respiratory tract. It is well-known that epithelial cells of airways, endothelial cells of circulation, and circulating inflammatory cells synthesize NO from
As described previously, there is very limited information in using FeNO as a follow-up parameter in patients with PH. The aim of this study was first to compare the basal FeNO values with healthy controls and second to evaluate the level of FeNO in patients with PH during follow-up, regardless of the therapy given and comparing FeNO with other follow-up parameters for determining its value for prognosis.
Methods
Patients with pulmonary arterial hypertension (PAH) and chronic thromboembolic PH (CTEPH) who were followed-up in the PH Clinic of Istanbul University, Istanbul Faculty of Medicine, were enrolled in this study. All participants voluntarily signed their informed consent. The study was conducted in accordance with the principles of the Helsinki Declaration and was approved by, Istanbul Faculty of Medicine Institutional Board, Istanbul University (Ethics Board file no: 2013/730). This is a longitudinal study.
Demographics, comorbid diseases, PH class, respiratory symptoms, World Health Organization functional class, and findings of right-heart catheterization made at the time of diagnosis were recorded. Exclusion criteria were patients with groups 2, 3, and 5 PH, active smoking, and acute upper or lower respiratory tract infection.
All patients underwent spirometry, carbon monoxide diffusion (DLCO) test, transthoracic echocardiography, 6MWT, and pro-BNP measurements. Spirometry (ZAN 74N, Sydney, Australia) was performed according to approved standards. 13 Forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and FEV1–FVC ratio were measured. FEV1/FVC >80% and FVC <80%were evaluated as restriction, and FEV1/FVC <70% was evaluated as obstruction. Diffusing capacity of the lungs for DLCO was measured using Zan 74N (nSpire, Sydney, Australia) device and DLCO <70% is considered as pathologic. Transthoracic echocardiography was performed using a commercially available system (Vivid 7 Dimension). Transthoracic echocardiography was performed at the beginning of the study and in the third and sixth month by the same physician. Echocardiographic systolic pulmonary artery pressure (PAP), ejection fraction, right atrium, right ventricle, left ventricular end-systolic and left ventricular end-diastolic diameters, and tricuspid annular plane systolic excursion (TAPSE) values were recorded. Pulmonary artery systolic pressure was estimated from tricuspid regurgitation peak velocity and right atrial pressure. 14 Brain natriuretic peptide values at baseline, and third, and sixth months were recorded, and the presence of clinical worsening and treatments used were questioned. Fractional exhaled nitric oxide was measured at baseline, and third, and sixth months in a constant expiratory flow rate (50 mL/sec) for a 6-second duration using Aerocrine NIOX MINO. The American Thoracic Society (ATS)/European Respiratory Society (ERS) 2005 guideline recommendations were taken into account in providing the FeNO measurements: No eating in the last 1 hour before the measurement, measurements were taken at the same time of the day, and the patients were rested 15 minutes before the measurements. 15 Baseline FeNO levels of healthy nonsmoker controls were measured to compare with the patient group.
Statistical analysis was performed using SPSS 21.0 software (AIMS, Istanbul, Turkey). Descriptive values are shown as mean, standard deviation, median, and minimum–maximum. Categorical variables were expressed as case numbers and percentages. The normality of distribution of variables was examined using Kolmogorov-Smirnov and Shapiro-Wilk tests. Changes in echocardiography parameters, FeNO, pro-BNP, and 6MWT variables during follow-up were assessed using the paired t test and Wilcoxon test. Comparison of categorical variables was made using the χ2 test. Spearman correlation test was used to examine the relationship between the variables. In the multisubgroup analysis, 1-way analysis of variance was applied. P < .05 was considered as statistical significance.
Results
In total, 31 patients with PH including 19 PAH (61.3%), 12 CTEPH (38.7%), and 80 age- and sex-matched nonsmoker healthy controls were included in the study. Of the patients, 23 (74.2%) were women and 8 (25.8%) were men, and the average age was 53.4 ± 17.1 years. The average ages of the women and men were 51.0 ± 18.0 years and 60.2 ± 12.8 years, respectively (P = .13). Smoking history was present in 32.3% (n = 10) of patients (average 19.8 pack-years); all had quit smoking. In the PAH group, there were 13 patients with idiopathic PAH (IPAH) and 6 PAH associated with other diseases. Patients with PAH associated with other diseases included congenital heart disease (n = 3; 2 Eisenmenger syndrome, 1 truncus arteriosus); patients with connective tissue disease scleroderma (n = 1), scleroderma plus Sjogren syndrome (n = 1), and one was diagnosed as having familial mediteranean fever. The general characteristics of the patients are summarized in Table 1.
General Characteristics of the Whole Patients.
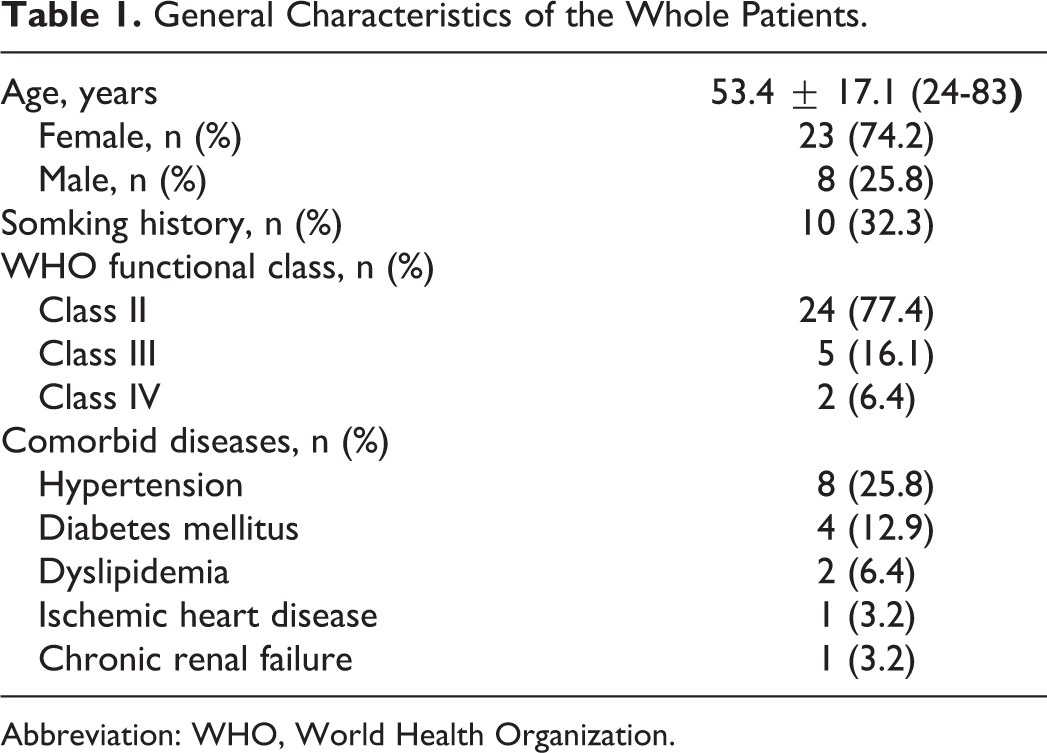
Abbreviation: WHO, World Health Organization.
The mean PAP was 56.16 ± 23.34 mm Hg, pulmonary capillary wedge pressure was 12.33 ± 3.77 mm Hg, and pulmonary vascular resistance was 8.42 ± 5.12 wood units in right-heart catheterization at the time of diagnosis. Four patients had a restrictive pattern and the remaining patients were evaluated as normal using spirometry. Six patients had low DLCO (<70%) levels. Right-heart catheterization and spirometry findings are given in Table 2.
Right-Heart Catheterization and Spirometry Findings of Patients With PH.
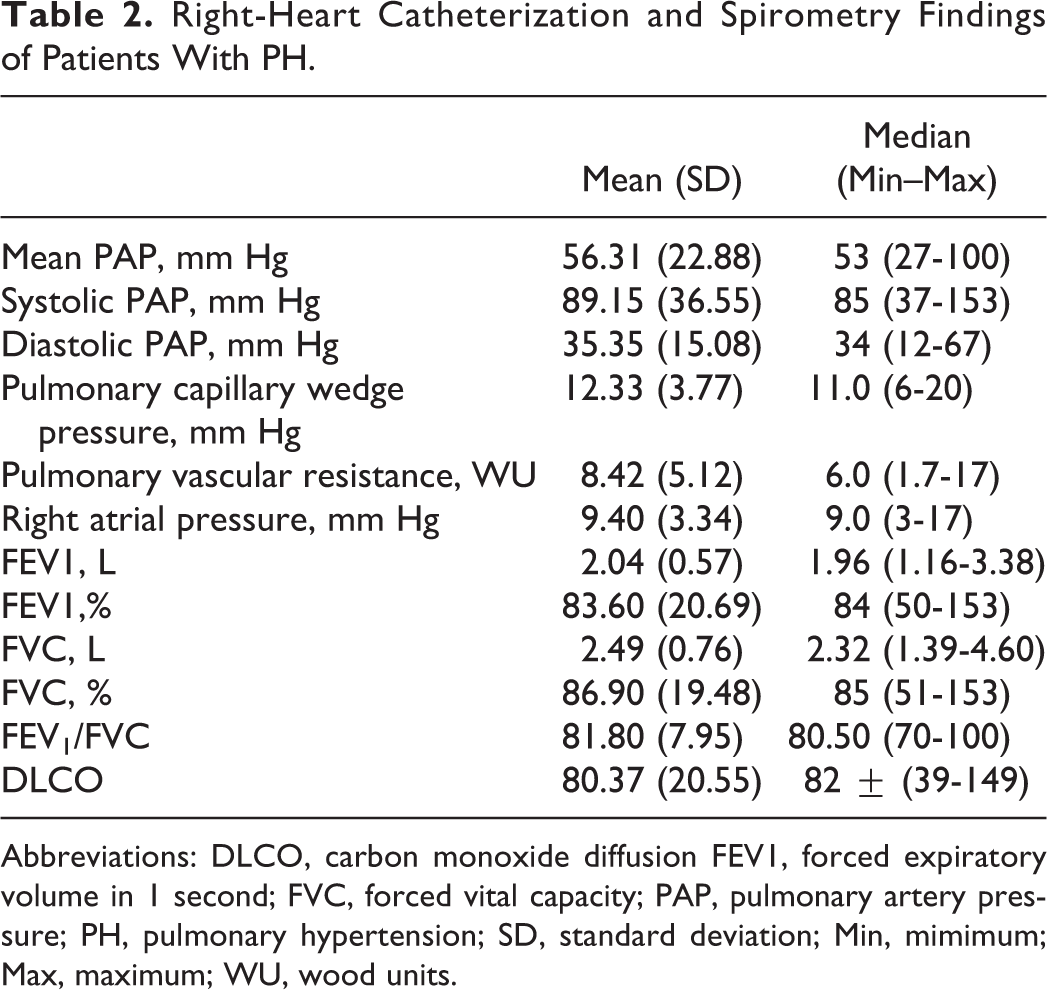
Abbreviations: DLCO, carbon monoxide diffusion FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; PAP, pulmonary artery pressure; PH, pulmonary hypertension; SD, standard deviation; Min, mimimum; Max, maximum; WU, wood units.
One patient could not cooperate with FeNO measurements and was excluded from the study in the third month; only measurements taken at the beginning of the study were used. Fractional exhaled nitric oxide measurements were made with 80 controls to compare with the patient group. Fractional exhaled nitric oxide did not differ between women and men throughout the patient and control groups. Fractional exhaled nitric oxide was statistically significantly lower in the control group than in the patient group (P = .04; Table 3).
Comparison of FeNO Levels in Patients and Controls.
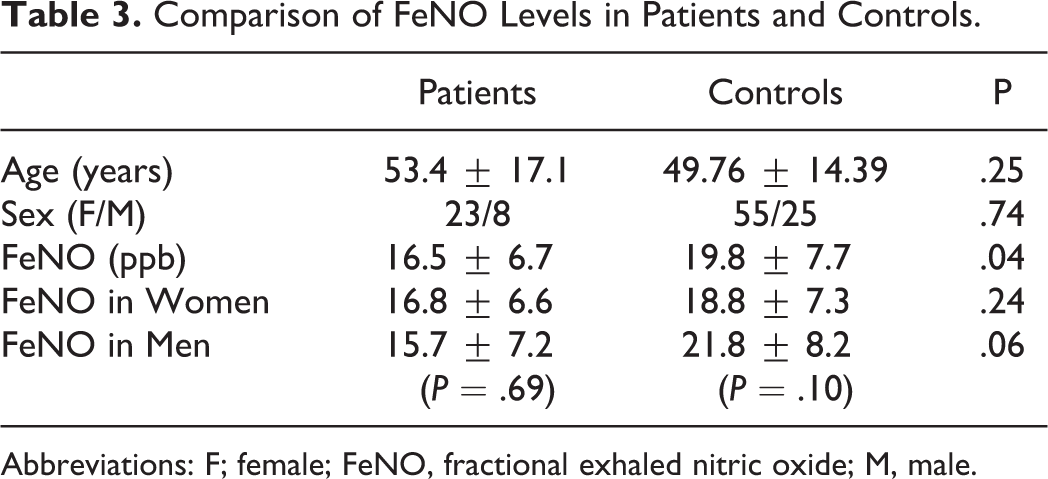
Abbreviations: F; female; FeNO, fractional exhaled nitric oxide; M, male.
Fractional exhaled nitric oxide levels were significantly decreased in the third month when compared to baseline, but FeNO levels did not change between 3 and 6 months and 0 and 6 months. At the third month, shorter 6-minute walk distance and higher pro-BNP levels were accompanied by FeNO decrease, but the results were not statistically significant. Results of other follow-up parameters are shown in Table 4.
Follow-Up Parameters at 6 Months.
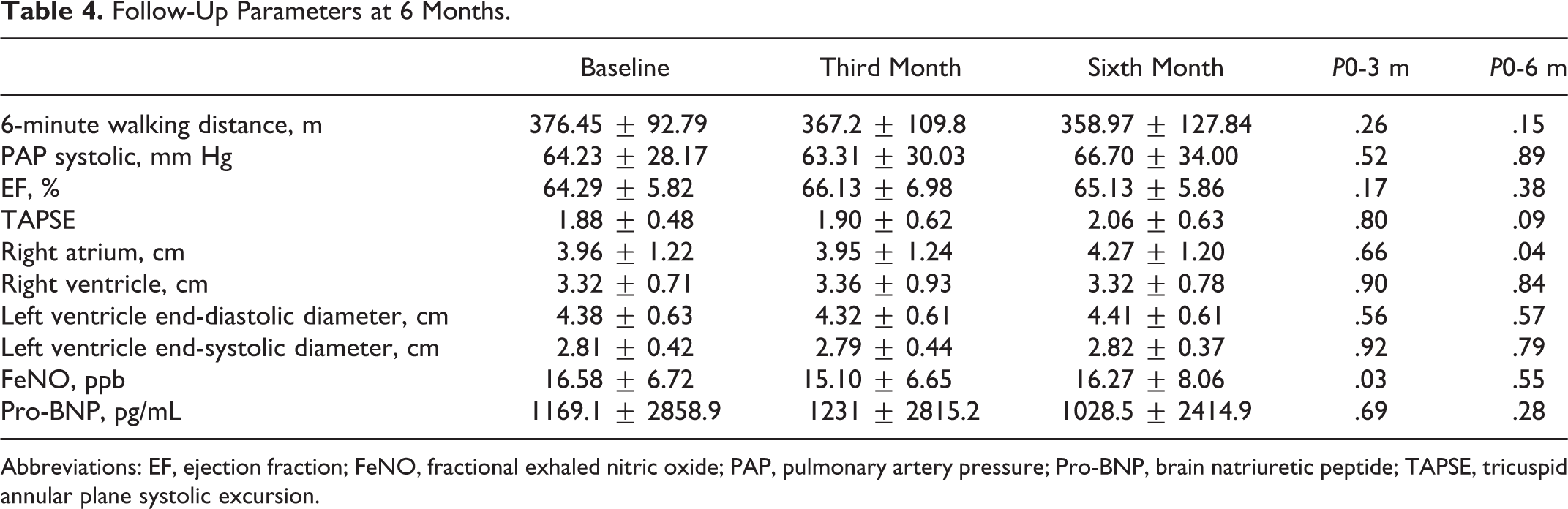
Abbreviations: EF, ejection fraction; FeNO, fractional exhaled nitric oxide; PAP, pulmonary artery pressure; Pro-BNP, brain natriuretic peptide; TAPSE, tricuspid annular plane systolic excursion.
There was no correlation between FVC, FEV1, FEV1/FVC, DLCO, and FeNO levels. The FeNO levels were lower in 6 patients who had TAPSE< 1.5 mm than in patients who had TAPSE> 1.5 mm (11.8 ± 3.7 ppb, 17.7 ± 6.8 ppb, respectively; P = .01). There was no correlation between FeNO and other follow-up measurements (Table 5).
Correlations Between FeNO and Follow-Up Parameters.
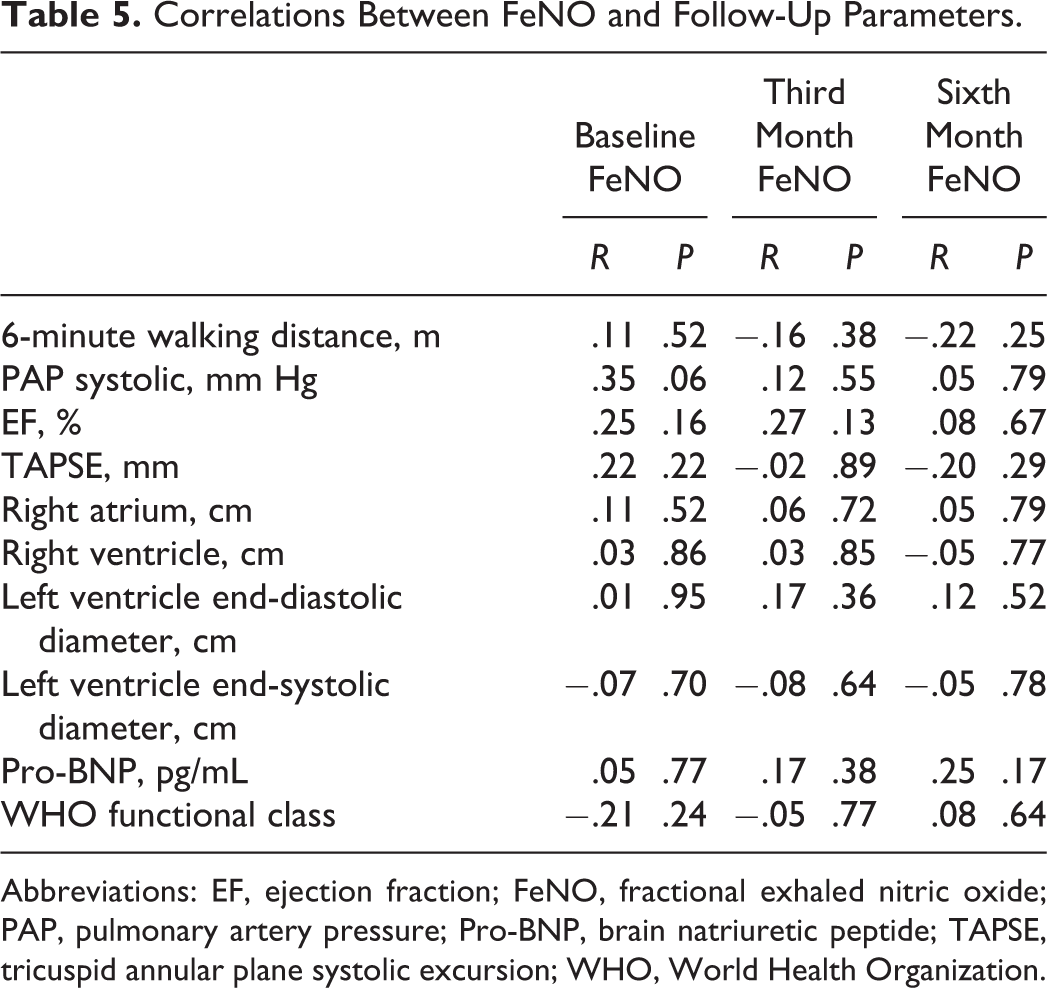
Abbreviations: EF, ejection fraction; FeNO, fractional exhaled nitric oxide; PAP, pulmonary artery pressure; Pro-BNP, brain natriuretic peptide; TAPSE, tricuspid annular plane systolic excursion; WHO, World Health Organization.
When the PAH group was subdivided into IPAH (n = 13) and PAH associated with other diseases (n = 6), FeNO was higher in the IPAH group in baseline and at the third month (P < .05; Table 6).
Comparison of FeNO Levels Between PAH Subgroups.
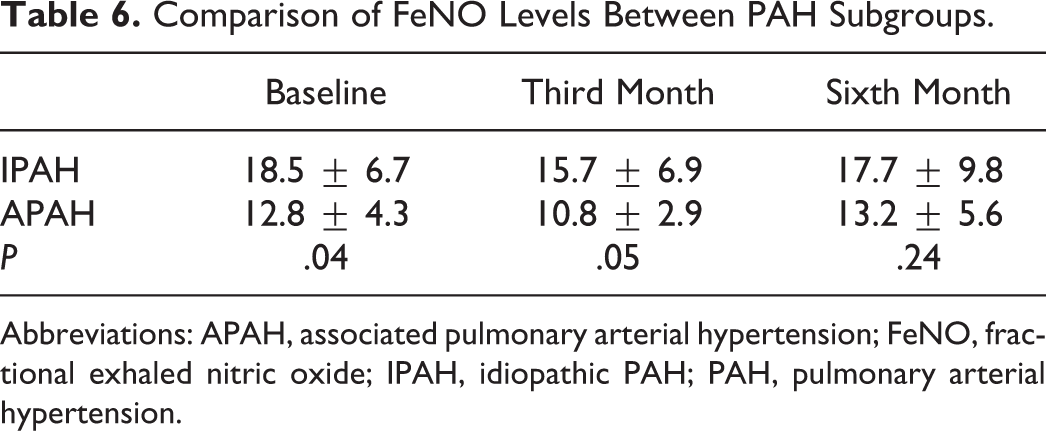
Abbreviations: APAH, associated pulmonary arterial hypertension; FeNO, fractional exhaled nitric oxide; IPAH, idiopathic PAH; PAH, pulmonary arterial hypertension.
Five patients showed clinical worsening, 2 were between 0 and 3 months, and 3 were between 3 and 6 months. When follow-up parameters were compared between the subgroups, the clinically deteriorated patients had shorter 6-minute walk distance (baseline P = .009, third month P = .02), higher mean PAP values (third month P = .05, sixth month P = .01), and slightly higher pro-BNP levels than patients who were clinically stable. Fractional exhaled nitric oxide was slightly higher in patients who had clinical worsening (Figure 1).
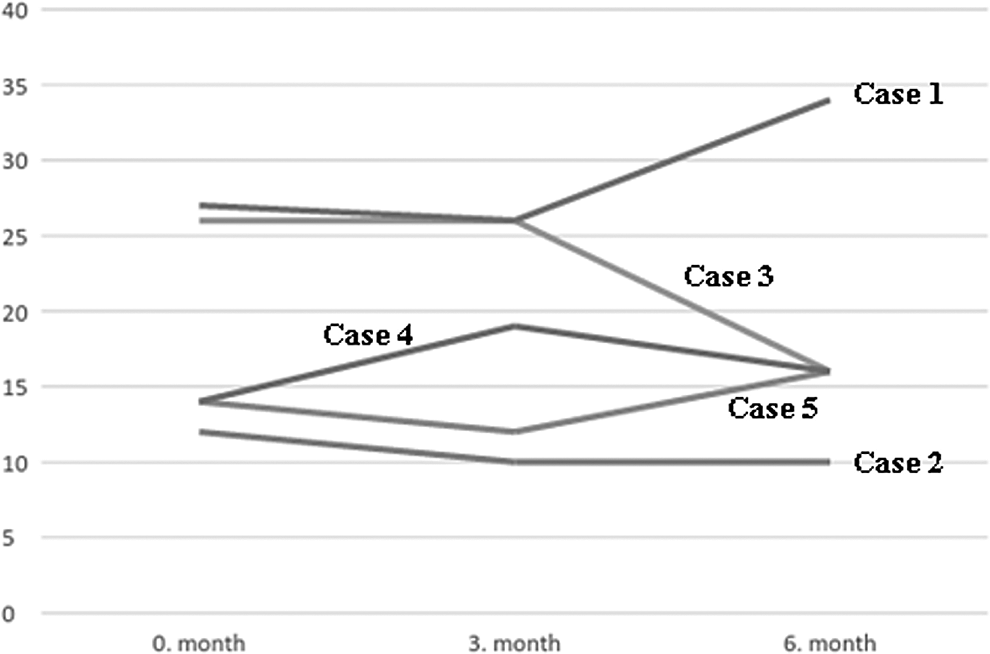
FeNO values (ppb) in clinically worsening patients. FeNO indicates fractional exhaled nitric oxide.
Discussion
Using FeNO as a follow-up measure in patients with PH is a very little investigated issue. In this study, we showed that FeNO is lower in patients with PH than healthy controls. We also showed that FeNO did not change significantly during the sixth month of follow-up and also did not change in patients who had clinical deterioration.
Since NO is detected in exhaled breath, there have been studies that investigate FeNO values in various disesases and also in patients with PH. There are studies that find FeNO in patients with PH higher, same, or lower compared to healthy controls. Our study revealed that the patient group had significantly lower FeNO levels when compared to controls. Kaneko et al 8 and Girgis et al 11 also found that FeNO levels of patients were lower than the healthy controls. In contrast, Malinovschi et al observed no difference between FeNO levels measured at various flow rates (20, 50, 100, and 200 mL/s) during their study that included 11 patients with PH and 21 controls. 16 In our study, the measurements were performed at a flow rate of 50 mL/s per the recommendations of the ATS. In another study by Riley et al, FeNO levels were measured at rest and peak exercise, and their findings reported no difference in FeNO between patients with IPAH and healthy controls. 17 In our study, the measurements were made at rest in accordance with the ATS guidelines. There are also 2 studies that have reported higher FeNO levels in patients compared to healthy controls. 10,18 When compared to these studies our study did not include patients with PH due to left-heart disease or patients with drug-induced PAH.
In the literature, only 2 follow-up studies were found which examined exhaled NO exchange in patients with PH. In the first study, Girgis et al compared the measurements of 10 patients with PAH (8 IPAH and 2 drug-induced PH) with those of 12 controls; FeNO was lower in the patient group than in the controls. 11 Fractional exhaled nitric oxide was increased to the level of controls after bosentan treatment. In our study, both baseline and follow-up FeNO measurements were performed under treatment; therefore, similar changes were not detected. In the other follow-up study, Machado et al performed measurements of FeNO and expired-air carbon monoxide on 17 patients who were treated for PAH for 2 years through baseline and first- and second year-end measurements. In the survived patients, no difference was observed between baseline measurements and FeNO levels at the end of first year. However, at the end of second year, FeNO levels were relatively increased. 12 In nonsurvived patients, NO levels were unchanged and FeNO appeared not to correlate with hemodynamic parameters, whereas baseline NO values of survived versus nonsurvived patients seemed to not differ. In our study, baseline and follow-up measurements were performed under treatment in a similar way, yet no significant change was observed among baseline, third month, and sixth month FeNO values. There was no treatment change that could explain the decrease in FeNO levels in the third month of follow-up. We did not observe the improvements in FeNO levels that Machado et al reported, during the second year of their study. We believe that the follow-up intervals might be the possible explanation for such inconsistency between the 2 studies. On the other hand, we did not have any nonsurvived patients during the follow-up period. Five patients experienced clinical deterioration, but no significant change was observed among follow-up values of FeNO, and there appeared to be no correlation between FeNO and follow-up parameters.
There is no other study that compared patients with IPAH and PAH associated with other diseases in terms of FeNO values. Our findings demonstrated that patients with IPAH exhibited statistical significantly higher FeNO levels than those with PAH associated with other diseases.
When looking to the correlations between the follow-up parameters that are used in routine clinical examinations, Andersen et al examined the relation between FeNO and biomarkers such as pro-BNP, troponin-T, and
We found patients with DLCO levels lower than 70% exhibited relatively lower FeNO values in the third and sixth months, but no statistical significance was found. Kharitonov et al and Malerba et al also did not find any relation between DLCO and FeNO values. 5 –20
The limitation of our study was the lack of data on pretreatment FeNO levels of patients. In addition, because FeNO measurements require a significant amount of patient cooperation, we observed a difficulty in performing measurements in patients who presented with low effort capacity and shortness of breath, and these patients were not able to complete the respiratory maneuver (follow-up measurements could not be performed in 2 patients). Thus, we observed that it was very difficult to evaluate the course of FeNO levels in patients with clinical deterioration.
Conclusion
In conclusion, our study demonstrated that FeNO is lower in patients with PH than in healthy controls. Fractional exhaled nitric oxide did not significantly change during the follow-up period. We found that FeNO correlated with TAPSE values, but these results are premature in determining the usefulness of FeNO in monitoring patients with PH. This can be explained by the small sample size and heterogeneous treatment regimens. Patient follow-up requires tools that are easy to deploy and could serve as a guide during the phase of transition to combination treatments. The present data show that more extensive studies on larger patient groups are needed to further clarify the usefulness of FeNO in patient follow-up.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.