
Abstract
Inflammation is a key feature of atherosclerosis and its clinical manifestations. The leukocyte count has emerged as a marker of inflammation that is widely available in clinical practice. Since inflammation plays a key role in atherosclerosis and its end results, discovering new biomarkers of inflammation becomes important in order to help diagnostic accuracy and provide prognostic information about coronary cardiac disease. In acute coronary syndromes and percutaneous coronary intervention, elevated levels of almost all subtypes of white blood cell counts, including eosinophils, monocytes, neutrophils, and lymphocytes, and neutrophil–lymphocyte ratio and eosinophil–leukocyte ratio constitute independent predictors of adverse outcomes. Eosinophil count and eosinophil–leukocyte ratio, in particular, emerge as novel biomarkers for risk stratification in patients with coronary artery disease. Since the presence of eosinophils denotes hypersensitivity inflammation and hypersensitivity associated with Kounis syndrome, this reality is essential for elucidating the etiology of inflammation in order to consider predictive and preventive measures and to apply the appropriate therapeutic methods.
Keywords
Introduction
Cardiovascular diseases are the most common cause of death in European men younger than 65 years of age and the second most common cause in women, while they cause 38% of all deaths in North America. 1 These diseases are expected to increase and to be the main cause of death globally in the following years owing to a rapidly increasing prevalence in developing countries and to the rising incidence of obesity and diabetes in the Western world. 2 Atherosclerosis and its consequences, coronary artery disease and myocardial infarction, continue to be significant causes of mortality and morbidity in the Western world. 3 Recent research has shown that immune cells are present in early atherosclerotic lesions and release effector substances that accelerate the progression of lesions and induce activation of inflammation that can elicit acute coronary syndromes. Since inflammation plays a key role in atherosclerosis and its end results coronary artery disease, angina pectoris, and myocardial infarction, discovering new biomarkers of inflammation becomes important in order to help diagnostic accuracy and to provide prognostic information about this disease. This will help clinicians in deciding how aggressively they need to treat such diseases. This review highlights the role of inflammatory biomarkers in prediction, prevention, and treatment of acute coronary syndromes.
Atherosclerosis as Inflammatory Process
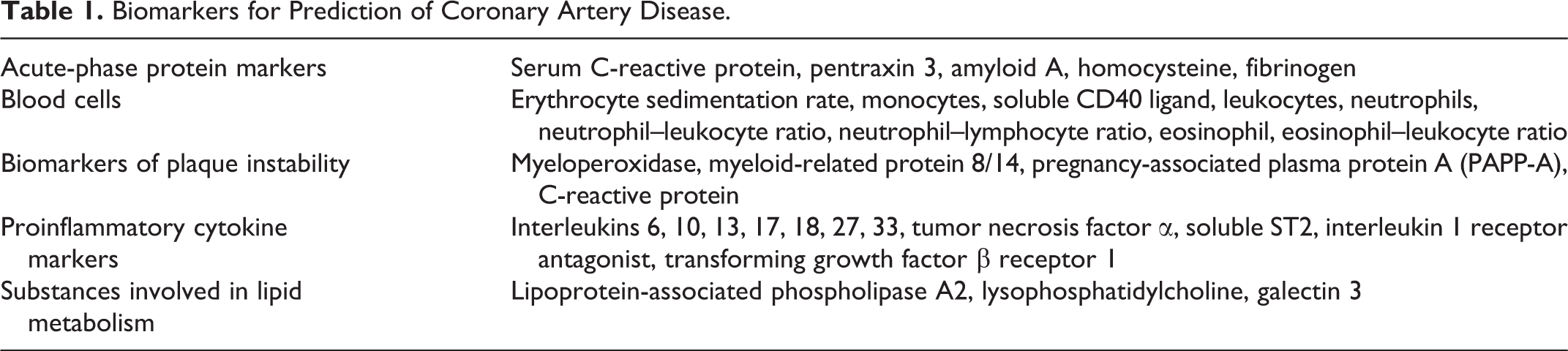
Inflammation plays an important role in the development of atherosclerosis, which can lead to acute myocardial infarction and is also a key factor in the long-term outcome of acute coronary syndromes. Although in the past atherosclerosis was considered to be the result of passive lipid accumulation in the vessel wall, today it is considered as chronic inflammatory disease that results in the formation of plaques that can erode or rupture, leading to acute coronary events. Cells of the innate and adaptive immune system play a crucial role in pathogenesis of atherosclerosis. The immune system decisively influences the propensity of a given plaque to rupture and cause clinical symptoms such as cardiovascular and cerebrovascular events. This takes place via transformation of immune cells into pro- and anti-inflammatory chemokine- and cytokine-producing units and by guiding the interactions between the different immune cells. 4 The inflammatory activity within the atherosclerotic plaques may be detected by markers of inflammation that have been found to be associated with both extent and severity of atherosclerotic lesions. In an effort to predict single or repeated ischemic episodes of non-ST-segment elevation myocardial infarction, ST-segment elevation myocardial infarction, and unstable angina, 5 numerous such markers have been proposed (Table 1). There is a lack of measurement standardization, missing regularity in epidemiological results from prospective studies with end points, and failure of evidence that the novel biomarker adds to risk prediction over and above that already achievable through the use of traditional risk factors. 5 This has rendered such biomarkers not reliable for routine use in risk evaluation for coronary artery disease. 6 However, the knowledge that atherosclerosis is an inflammatory disease offers new opportunities for the prevention and treatment of coronary artery disease, and in this extend, the discovery of new biomarkers of inflammation is of paramount importance.
Biomarkers for Prediction of Coronary Artery Disease.
White Blood Cell Count as Predictor of Major Adverse Cardiovascular Events and Mortality in Acute Coronary Syndromes
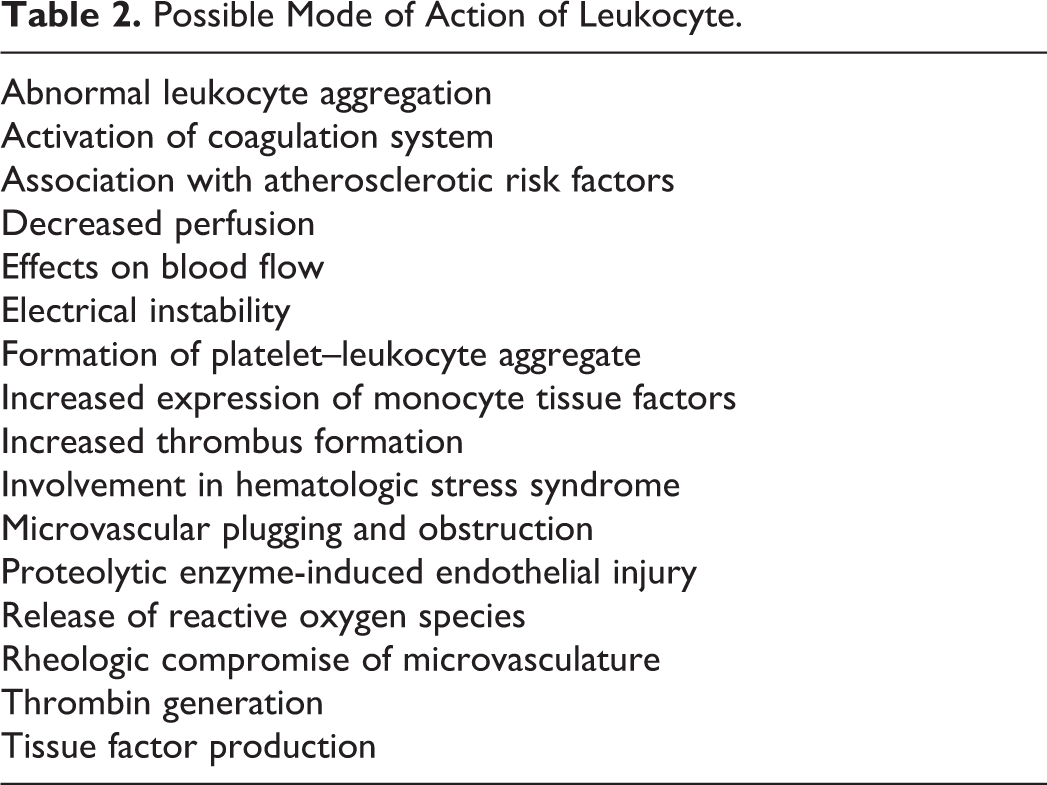
The role of total white blood cell count in patients with acute myocardial infarction has been emphasized in several studies. Leukocytes are major mediators of inflammation and have a key role in host defense to injury. Increased white blood cell count has been associated with a worse outcome in patients with stable coronary disease, in acute coronary syndromes, and even in general population. 7,8 It has been stated that the relationship between white blood cell count and coronary heart disease is strong, consistent, dose dependent, independent, biologically plausible, coherent with the current paradigm of the inflammatory origin of atherosclerosis, and appears to be independent of other traditional coronary risk factors, including smoking. 9,10 These cells may act through several mechanisms (Table 2) including the production of rheologic compromise of the microvasculature by adhesion, aggregation, platelet recruitment, distal embolization, microvascular plugging, and microvasculature obstruction. 11 They can form platelet–leukocyte aggregate, provide catalytic surface for thrombin generation, and produce tissue factor thus facilitating thrombosis and acute coronary events. 12 Leukocytes, through the release of reactive oxygen species, proteases, eicosanoids, interleukins, and myeloperoxidase, may contribute to oxidative and proteolytic myocardial injury. 13 Furthermore, leukocyte count was found to be a modulating factor for the mortality benefit of bivalirudin in ST-segment elevation acute myocardial infarction in the Harmonizing Outcome with Revascularization and Stent in Acute Myocardial Infarction (HORIZONS-AMI) trial. 14 The reduction in mortality was independent of major bleeding, suggesting that other mechanisms, involving leukocytes, may be implicated in the survival benefit observed with bivalirudin. In 2013, 11 studies have examined the role of neutrophil–lymphocyte ratio in association with acute myocardial infarction. Three of these very interesting studies have been published recently in Clinical and Applied Thrombosis/Hemostasis. 15 –17 The first showed that a high neutrophil–lymphocyte ratio is a strong and independent predictor of in-hospital cardiovascular mortality due to acute myocardial infarction with ST-segment elevation. 14 The second examined the association of the neutrophil–lymphocyte ratio with Global Registry of Acute Coronary Events (GRACE) risk scores in patients with ST-segment elevation myocardial infarction and found that this ratio is significantly associated with adverse in-hospital outcomes, independent of GRACE risk score. 16 The third evaluated leukocytes and neutrophil–lymphocyte ratio in prediction of coronary thrombus formation in non-ST-segment elevation acute coronary syndrome and concluded that leukocyte count and neutrophil–lymphocyte ratio may give an indication about the presence of coronary thrombus. 17 The significance of neutrophil–lymphocyte ratio has also been emphasized in other similar contemporary studies. This ratio is significantly correlated with angiographic severity of acute coronary syndromes assessed by SYNTAX score. 18 It is an excellent predictor of short- and long-term survival in patients with revascularized ST-segment elevation myocardial infarction with optimal cutoff value of 7.4. 19 It is an independent indicator for no-reflow development in patients who have undergone percutaneous coronary intervention for acute ST-segment elevation myocardial infarction. 20,21 It is a significant independent predictor of major adverse cardiovascular events in diabetic patients. 22 It is significantly related to angiographic thrombus burden and spontaneous early infarct-related artery patency in patients with acute ST-segment elevation myocardial infarction. 23 Finally, this ratio is significantly associated with patients at high risk of critical limb ischemia and other vascular end points. 24
Possible Mode of Action of Leukocyte.
Eosinophils and Eosinophil–Leukocyte Ratio as Inflammatory Markers in Patients With Coronary Artery Disease
In all of the above-mentioned studies, detailed differential count was not available and therefore assessing the relative impact of white blood cell count subpopulations on myocardial infarction was not reported. None of the above-mentioned studies have focused attention on the presence of eosinophils and/or eosinophil–leukocyte ratio. This was probably based on the study, which has suggested that total white blood cell count is a better correlate of long term than differentials. 8 However, some older studies have shown that elevated levels of almost all subtypes of white blood cell counts, including eosinophils, 25 monocytes, 26 neutrophils, 27 and lymphocytes (an inverse relationship), 28 have been associated with increased risk of coronary heart disease. The large, disease-free patient cohort from the Adult Health Study of Hiroshima and Nagasaki showed a relationship between the total white blood cell count, including the eosinophil, neutrophil, and monocyte counts, and the incidence of coronary heart disease. 26 The Caerphilly and Speedwell studies showed that increased coronary risk was associated with high neutrophil, eosinophil, lymphocyte, monocyte, or basophil counts. 29 The etiology of inflammation is variable, but the presence of eosinophils identifies the etiology of inflammation since they denote hypersensitivity inflammation. 30 Eosinophils are multifunctional leukocytes implicated in the pathogenesis of numerous inflammatory processes including allergic diseases, tumor immunity tissue injury, bacterial and viral infections, and parasitic helminth. Eosinophils are recruited from the circulation into inflammatory sites where they modulate immune responses through an array of mechanisms. Their surface brings H4 histamine receptors that facilitate eosinophil chemotaxis toward mast cells, which are the major producers of an array of inflammatory soluble mediators. Soluble mediators secreted by mast cells and eosinophils also modulate reciprocal interactions between these 2 cells in the so-called “allergic effector unit.” 31
Several studies have shown the role of eosnophils as a novel biomarker for risk stratification of patients with coronary artery disease. Eosinophilic cationic protein, which is highly basic, cytotoxic, heparin-binding ribonuclease exclusively secreted from eosinophils and constitutes a tool for monitoring hypersensitivity inflammation, was found to be associated with the use of bare metal and drug-eluting stents. Basal eosinophilic cationic protein levels are associated with major adverse cardiac events after bare metal stent implantation, 32 suggesting that hypersensitivity-mediated inflammation against the metal could explain adverse reactions associated with coronary stenting. Furthermore, preintervention eosinophilic cationic protein baseline serum levels can predict clinical outcomes such as sudden death, stent thrombosis, and myocardial infarction following implantation of drug-eluting stents. 33 Coronary vasospasm associated with eosinophilia responds poorly to conventional vasodilator treatment, and while the risk of recurrent coronary events is high, the majority of patients respond to treatment that suppresses eosinophilia such as corticosteroids. 34 In another study, 35 it was found that eosinophil count in the third tertile was associated with an increased risk of all-cause, long-term mortality after the initial 6 months following percutaneous coronary intervention. This was attributed to an increased risk of thrombus formation because eosinophils infiltrate the site of stent implantation and release a number of mediators that can increase platelet activation and aggregation. 36 Eosinophils are participating in the pathogenesis of Kounis syndrome. 37 The Kounis syndrome was described in 1991 as allergic angina and allergic myocardial syndrome and is defined today as the concurrence of acute coronary syndromes with conditions associated with mast cell activation, involving interrelated and interacting inflammatory cells, and including allergic or hypersensitivity and anaphylactic or anaphylactoid insults. It is caused by inflammatory mediators such as histamine, neutral proteases, arachidonic acid products, platelet-activating factor, and a variety of cytokines and chemokines released during the activation process. A subset of platelets bearing FCγRI, FCγRII, FCεRI, and FCεRII receptors are also involved in the activation cascade. There are 3 variants of this syndrome which include vasospastic angina with normal or near-normal coronary arteries which can progress to acute myocardial infarction, acute myocardial infarction with culprit but quiescent coronary artery disease, and hypersensitivity-associated stent thrombosis. Indeed, in Kounis hypersensitivity associated with acute coronary syndrome type third variant, stent thrombus is infiltrated by eosinophis and/or mast cells. 37
In a recent study concerning 89 patients with persistent atrial fibrillation and thrombus formation in the left atrium and left atrial appendage, eosinophil concentration, independent of hemodynamic risk factors, was found to have procoagulant effects in predicting thrombus formation, in comparison to the control group. The conclusion was that eosinophils and mean platelet volume value can be predictive on left atrial thrombus formation in patients with atrial fibrillation. 38 The relationship between eosinophil count and coronary artery calcification was also assessed in a study of 1363 consecutive participants with clinical suspicion of coronary heart disease. 39 Evaluation of the relationship between coronary artery calcification scores was determined by multislice computed tomography and peripheral eosinophil count as well as major cardiovascular risk factors, including age, body mass index, smoking status, hypertension, dyslipidemia, diabetes mellitus, high-sensitivity C-reactive protein, and estimated glomerular filtration rate. Positive correlations were found between age and eosinophil count, and the conclusion was that eosinophil count is correlated positively with coronary artery calcification. In an autopsy study of 20 randomly selected patients having acute myocardial infarction complicated by cardiac rupture, the number of eosinophils in the inflammatory response was significantly greater in hearts with cardiac rupture than in the control hearts. This was attributed to eosinophil rich in arylsulfatase B, peroxidase, glucuronidase, β-glycerophosphatase, major basic protein, and eosinophilic cationic protein that may further weaken the necrotic myocardium and, in part, determine whether acute myocardial infarction will eventually result in cardiac rupture. 40 In a thrombus aspiration study of 209 consecutive patients, 41 with acute coronary syndromes during emergency coronary angiography, 165 thrombus sample sections were stained with hematoxylin and eosin and were examined for eosinophils. Eosinophil infiltration was observed predominantly in the area between white thrombus and red thrombus in 106 samples. The conclusion was that eosinophils may play an important role in coronary occlusion by promoting thrombus growth.
In a case–control study of 190 individuals with and without coronary artery disease, it was found that the absolute number of eosinophils and the eosinophil–leukocyte ratio in the peripheral blood smear was significantly elevated in patients with coronary artery disease compared to the control group. 42
Finally, in a genome-wide association scan of blood in more than 9000 Icelanders, a genetic analysis of the inflammatory role of eosinophils was conducted in order to determine the sequence variants affecting eosinophil counts and to evaluate the association with inflammatory disorders. The analysis revealed that a single-nucleotide polymorphism at 12q24, in SH2B3, had significant association with myocardial infarction in the scan data set and that was consistent with 6 replication sets of European ancestry, with an odds ratio of 1.13 (95% confidence interval, 1.08-1.18). 43
Conclusion
Elevated levels of almost all subtypes of white blood cell counts, including eosinophils, monocytes, neutrophils, and lymphocytes, and neutrophil–lymphocyte ratio and eosinophil–leukocyte ratio constitute independent predictors of adverse outcomes following acute coronary syndromes and percutaneous coronary intervention. Eosinophil count and eosinophil–leukocyte ratio, in particular, emerge as novel biomarkers for risk stratification in patients with coronary artery disease. Since the presence of eosinophils denotes hypersensitivity inflammation, this reality is essential for elucidating the etiology of inflammation in order to apply predictive and preventive measures and to consider appropriate therapeutic methods.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.