
Abstract
Introduction: We postulated that the risk of venous thromboembolic disease (VTE) may persist after discharge and tested this hypothesis in patients undergoing colorectal resection for cancer. Methods: The American College of Surgeons National Surgery Quality Improvement Program database was queried for patients undergoing colorectal resections for cancer from 2005 to 2009. The outcome analyzed was a 30-day deep vein thrombosis (DVT) and/or pulmonary embolism (PE). Multivariable forward stepwise regression was used to identify independent predictors of VTE. Results: The database contained 21 943 colorectal cancer resections. The 30-day DVT rate was 1.4% (306 of 21 943), 29% (89 of 306) were diagnosed post-discharge. The 30-day PE rate was 0.8% (180 of 21 943), 33% (60 of 180) was diagnosed post-discharge, the combined DVT/PE rate was 2.0% (446 of 21 943). The median time to diagnosis of VTE was 9 days (interquartile range 4-16) after surgery. Post-discharge VTE rates in patients with length of stay (LOS) less than 1 week (0.6%) were similar to patients with LOS greater than 1 week (0.7%, Fisher exact P not significant). Independent risk factors for post-discharge VTE were preoperative steroid use for chronic condition (odds ratio [OR] 2.90, 95% confidence interval [CI] 1.51-5.57, P = .001) and preoperative systemic inflammatory response syndrome (OR 2.26, 95% CI 1.24-4.10, P = .008). Conclusions: Diagnosis of almost one third of postoperative VTE in this patient population occurred after discharge. The duration of the prothrombotic stimulus of surgery is not well defined, and patients with malignancy are at high risk of VTE; thromboprophylaxis after discharge should be considered for these patients.
Keywords
Introduction
Mechanical and pharmacological prophylaxis is effective in preventing postoperative VTE, but thromboprophylaxis is often discontinued after discharge. The risk of VTE may persist long after the initial triggering event for some patients.1,2 The American College of Chest Physicians (ACCP) 2008 guidelines state “For selected high-risk general surgery patients, including some of those who have undergone major cancer surgery or have previously had VTE, we suggest that continuing thromboprophylaxis after hospital discharge with LMWH for up to 28 days be considered (Grade 2A).” 3 The activation of the coagulation system persists for at least 14 days after surgery. 4 We postulated that patients may still be at risk of venous thromboembolic (VTE) events after discharge and tested this hypothesis in patients undergoing colorectal resection for cancer, a high-risk population. We therefore sought to determine the rates and risk factors for VTE in-hospital and post-discharge within 30 days of colorectal cancer resection. The American College of Surgeons National Surgery Quality Improvement Program (ACS NSQIP) has rigorous follow-up for 30 days after surgery on a large systematic multicenter sample of general surgery patients, therefore it provided a clinically robust data set for the analysis.5,6
Methods
A prospective, systematic study of patients undergoing major general surgical procedures was performed at over 200 hospitals as part of the ACS NSQIP. In participating hospitals a data coordinator collected over 50 preoperative patient characteristics, intraoperative processes of care, and 22 uniformly defined postoperative adverse occurrences (including deep vein thrombosis [DVT], pulmonary embolism [PE], and death) up to 30 days after the operation. The systematic sample was performed by including the first 40 operations in each 8-day cycle per data coordinator. Risk and outcome variables were rigorously defined, and coordinators had previously completed in-depth training on all study definitions. Deep vein thrombosis was defined as, “identification of a new blood clot or thrombus within the venous system confirmed by a duplex, venogram, or CT scan. The patient must be treated with anticoagulation therapy and/or placement of a vena cava filter or clipping of the vena cava.” Pulmonary embolism was defined as “lodging of a blood clot in a pulmonary artery with subsequent obstruction of blood supply to the lung parenchyma identified with a V-Q scan interpreted as high probability of pulmonary embolism or a positive CT spiral examination, pulmonary arteriogram, or CT angiogram.” Thirty-day follow-up information was obtained through phone calls, letters, and review of clinic/hospital medical records. Regular conference calls, annual meetings, and site visits were used to maintain data reliability. Additional operations within 30 days of an included case were excluded. Patients less than 16 years old and admissions for trauma were excluded.
The ACS NSQIP database was queried for patients undergoing colorectal resections for cancer based on the primary procedure Current Procedural Terminology (CPT) code and operative International Classification of Diseases, Ninth Revision (ICD-9) diagnosis code. The primary procedure CPT codes used to identify colorectal resections are listed in the Appendix A and ICD-9 codes between 145.0 and 209.9 were used to identify cancer. The outcome analyzed was VTE up to 30-day postoperation. Venous thromboembolism was defined as DVT and/or PE as defined by the ACS NSQIP.
Venous thromboembolism occurrences were analyzed by postoperative day (POD) and by whether they occurred during the surgical hospitalization (in-hospital) or after initial discharge (post-discharge). Post-discharge VTE may have been diagnosed as part of a readmission. Multivariable forward stepwise regression (P for entry <.05, for exit >.10) was used to identify preoperative predictors of in-hospital and post-discharge VTE. SPSS statistical software version 18 was used for all analyses; P < .05 was set as the significance threshold.
Results
The database contained 21 943 colorectal cancer resections with 6213 (28.3%) coded as laparoscopic. The patients' mean age at time of operation was 66.3 ± 13.8 (standard deviation [SD]) years and 10 713 (48.8%) were female. The median length of hospital stay was 7 days (interquartile range [IQR] 5-10). In-hospital, post-discharge, and total rates of DVT, PE, and VTE are shown in Table 1 . Post-discharge occurrences accounted for 29% of DVT, 33% of PE, and 31% of VTE. The 30-day mortality rate more than tripled in patients experiencing VTE (38 of 446, 8.5% vs 529 of 21 497, 2.5%, Fisher exact P < .001).
Rates of 30-Day Deep Vein Thrombosis and/or Pulmonary Embolism in 21 943 Patients Undergoing Colorectal Cancer Resection From Over 200 Hospitals

The median time to diagnosis of VTE was 9 days (IQR 4-16). The daily risk of VTE diagnosis was about 1 per thousand VTE “survivors” starting the day after surgery. This risk remained fairly constant until POD 9. Thereafter, the risk decreases more or less steadily until POD 30. Post-discharge VTE started on POD 5 and comprised the major proportion of VTE after POD 14 (Figure 1 ). In-hospital VTE rates increased linearly from 0.8% in patients with length of stay (LOS) less than 1 week to 1.6% in patients with LOS of 3 weeks (chi-square test for linear trend, P < .001). Post-discharge VTE rates were similar in patients with LOS less than 1 week (0.6%) compared to patients with LOS greater than 1 week (0.7%, Fisher exact P not significant). In patients who experienced a post-discharge VTE, the median number of days from discharge until diagnosis was 9 (IQR 4.25-12; Figure 2 ). The 30-day follow-up available in the database would curtail somewhat the number of VTEs diagnosed 3 or more weeks after discharge.
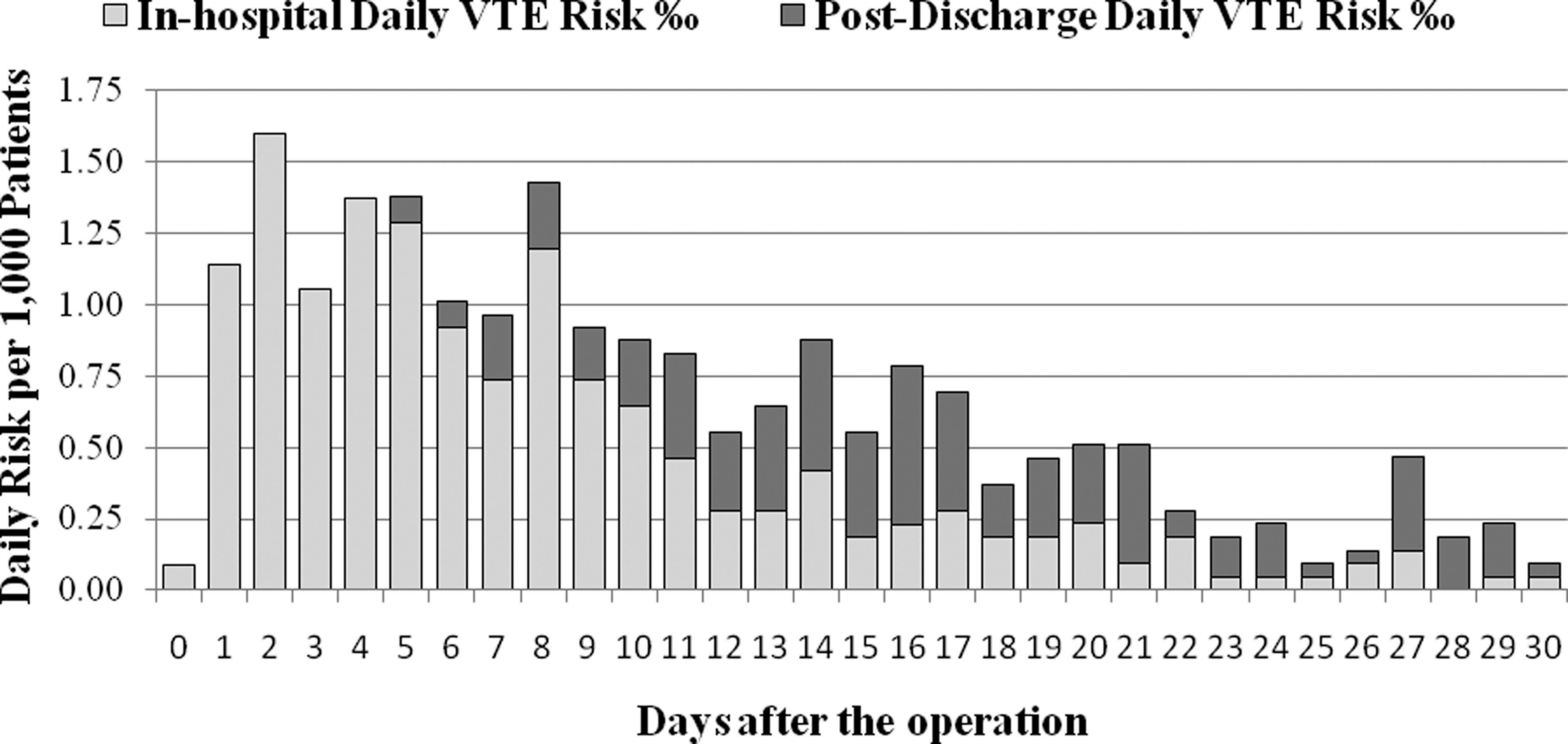
In-hospital and post-discharge venous thromboembolism in 21,943 patients undergoing colorectal cancer resection; by postoperative day per thousand survivors without VTE up to that day.
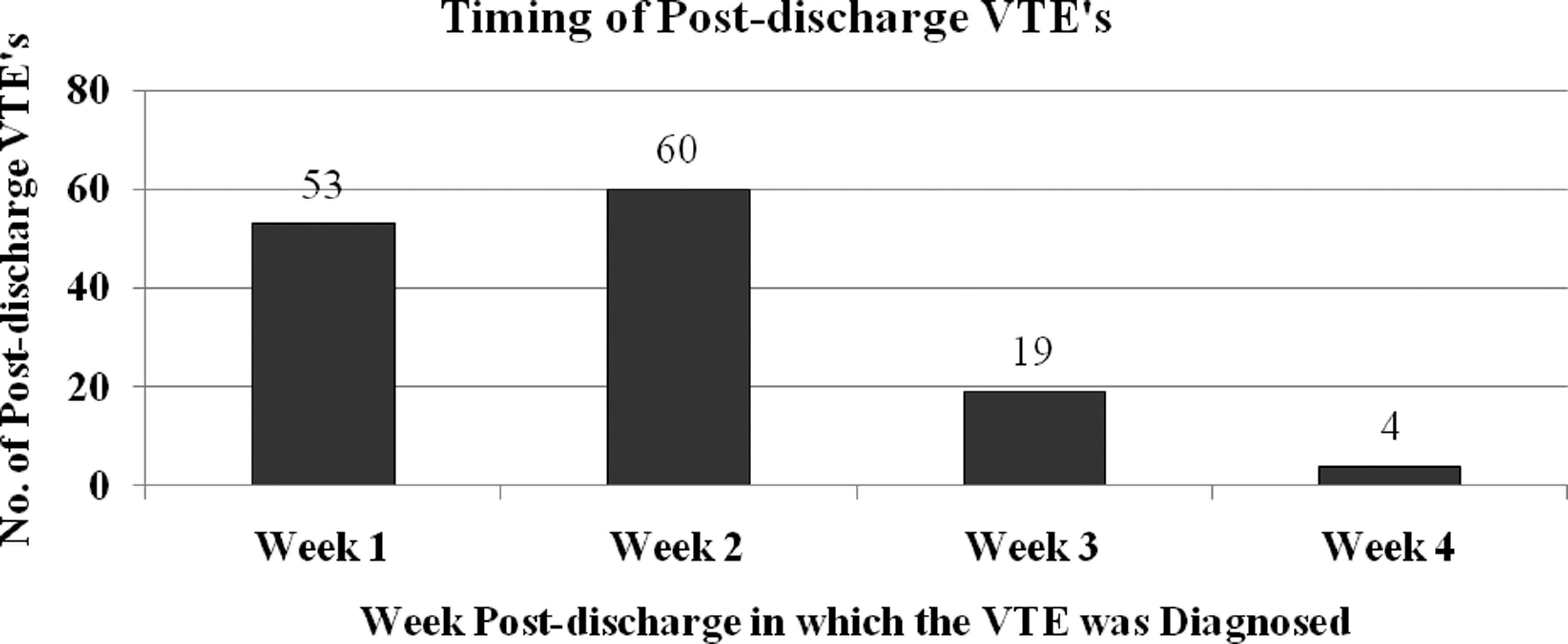
Most post-discharge VTE’s are diagnosed within 1 to 2 weeks after discharge from hospitalization for colorectal cancer resection.
Preoperative predictors of in-hospital VTE are shown in Table 2 with their odds ratios (ORs) after adjustment for the other variables noted. Our analysis confirmed several well-known risk factors. In this select group of patients with cancer, disseminated cancer, recent chemotherapy, and recent weight loss all independently conferred increased risk of VTE. Serum albumin was independently protective, and to our knowledge this has not been noted in the literature. It may be a further marker of aggressive cancer or represent a new risk factor. Obesity (body mass index greater than 35 kg/m 2 ) conferred higher risk. Asian/Pacific Islander race was highly protective while blacks were at higher risk than white race patients with adjustment for obesity. Males were at higher risk independently of stroke or coronary disease history, which were both risk factors as well.
Patient Risk Factors for In-Hospital VTE From Forward Stepwise Logistic Regressiona,b
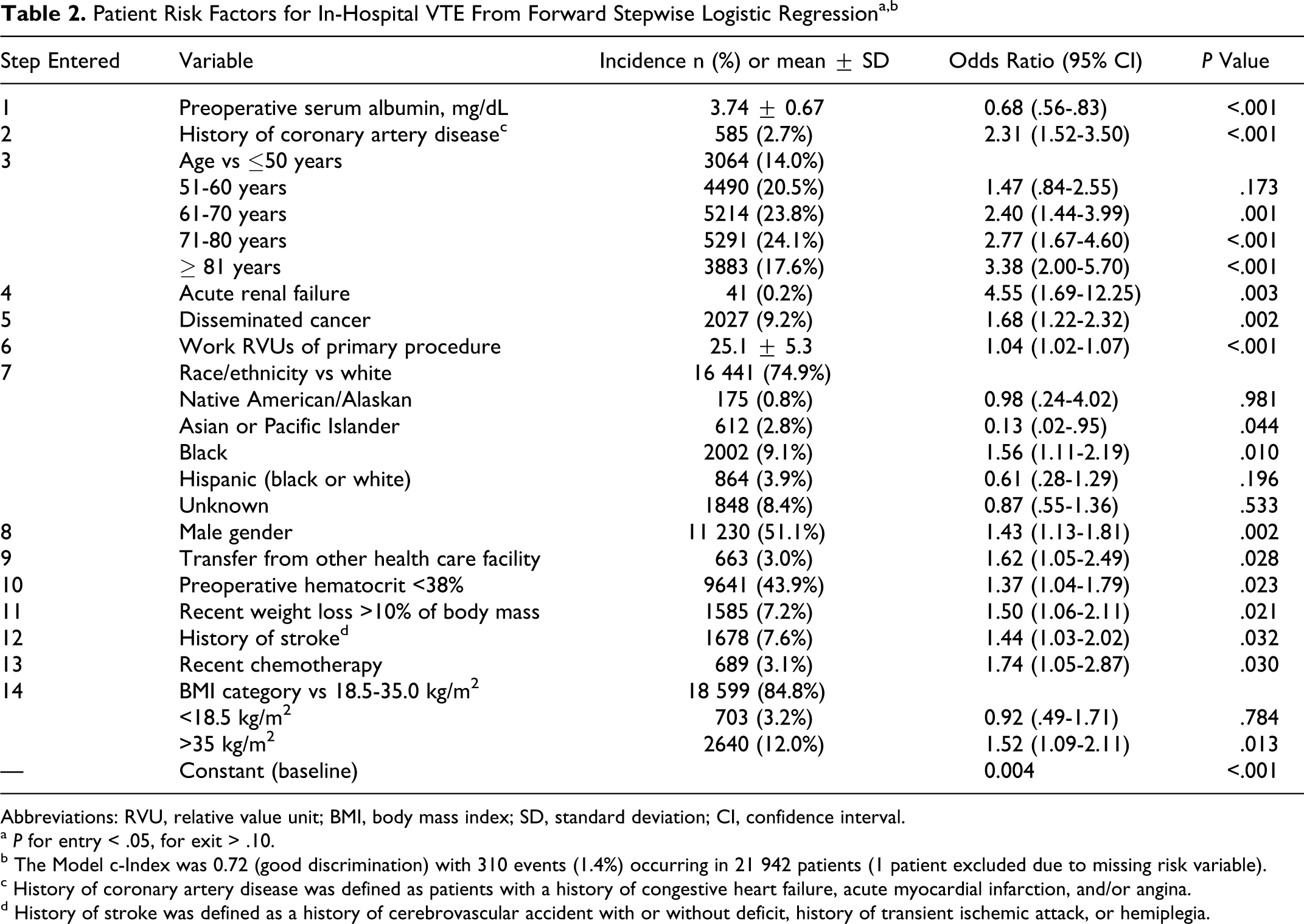
Abbreviations: RVU, relative value unit; BMI, body mass index; SD, standard deviation; CI, confidence interval.
a P for entry < .05, for exit > .10.
b The Model c-Index was 0.72 (good discrimination) with 310 events (1.4%) occurring in 21 942 patients (1 patient excluded due to missing risk variable).
c History of coronary artery disease was defined as patients with a history of congestive heart failure, acute myocardial infarction, and/or angina.
d History of stroke was defined as a history of cerebrovascular accident with or without deficit, history of transient ischemic attack, or hemiplegia.
None of the in-hospital VTE risk factors were predictive of post-discharge VTE for the 30-day follow-up period. After consideration of over 55 preoperative risk factors, only preoperative steroid use for chronic condition and systemic inflammatory response syndrome were predictive of post-discharge VTE (Table 3 ). Operative variables such as open resection, operative duration, transfusion, and wound classification were not significant predictors of post-discharge VTE.
Patient Risk Factors for Post-Discharge VTE From Forward Stepwise Logistic Regression
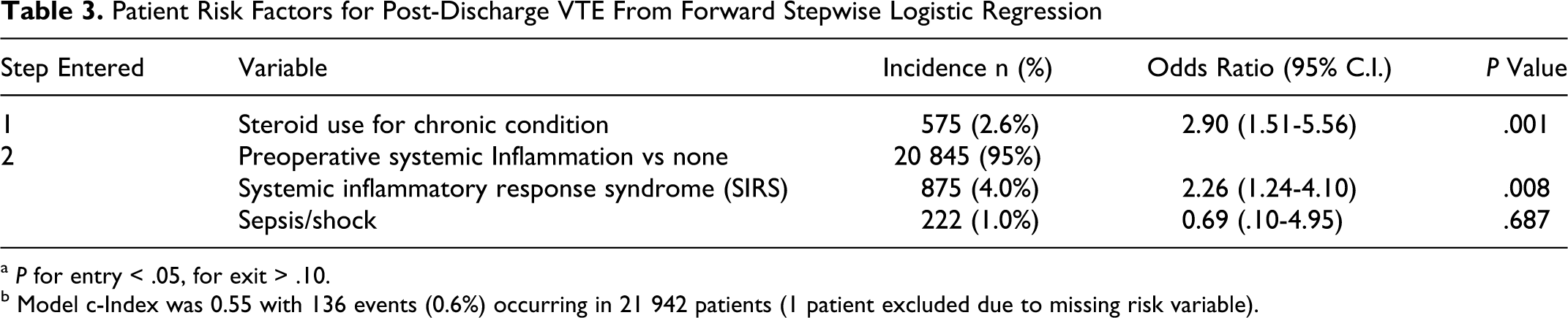
a P for entry < .05, for exit > .10.
b Model c-Index was 0.55 with 136 events (0.6%) occurring in 21 942 patients (1 patient excluded due to missing risk variable).
Discussion
Deep venous thrombosis (DVT) and pulmonary embolism (PE) are still among the most common causes of morbidity and mortality in patients despite advances in medication, awareness, and prophylaxis. Predisposing risk factors for DVT or PE may include recent surgery, prolonged immobility, the hypercoaguable states (of which one is cancer), 7 and medications such as chemotherapy. 8 Patients undergoing surgery for abdominal cancer often have many or all of these risk factors which combine for an occurrence rate of nearly 20% in some studies, despite adequate prophylaxis. 9 The ENDORSE (Epidemiological International Day for the Evaluation of Patients at Risk of Venous Thromboembolism in the Acute Hospital Care Setting) survey recently reported that 93% of patients who underwent a major surgical procedure were at risk for VTE, with only 62% receiving ACCP-recommended prophylaxis. 10 Recently, the US Acting Surgeon General issued a “call to action,” prompting investigation into pharmacologic agents and doses, as well as other physical methods for the prevention of DVT. 11 Prior to surgery, risk that is often overlooked and underestimated as DVT was found in 8% of preoperative patients in one study. 12 The risk increases sharply into the immediate postoperative period and thrombotic events have been estimated at 19% to 25% for the average untreated general surgery patient. 13 In a report by Bergqvist et al, the DVT rates were studied in 91 days post discharge, with 74% of events occurring in this period; 54% of DVT occurred in 1 month, 18% in month 2, and 15% in month 3 after discharge. 14 In patients undergoing knee or hip replacement, the risk of VTE extends beyond the usual period of hospitalization and between one third and one half of thromboembolic events occurred after the median time to hospital discharge. 1 The ACCP guidelines recommend 7- to 10-day VTE prophylaxis with low-molecular-weight heparins (LMWHs) after major abdominal surgery and state that for selected high-risk general surgery patients continuing thromboprophylaxis after hospital discharge with LMWH for up to 28 days should be considered. 3 Our data help define the high-risk population and identify risk factors for post-discharge VTE.
Many well-known risk factors for VTE were not predictive of a post-discharge diagnosis over the 30-day follow-up period, while steroid use for chronic disease and systemic inflammatory response syndrome (SIRS) were predictive. Steroid use in patients with cancer has been identified as a risk factor for VTE in a study by Wun et al 15 as well. Another well-studied risk is the inherent procoaguable state of cancer. Studying only the risk added by the cancer itself, various abdominal cancers have DVT rates in the first post-diagnosis year of 14% for pancreatic, 7.4% for stomach, and 2.3% for colon; cumulative risk in the patients with colon cancer is increased, given the probability of long-term disease. 7 In addition, metastasis increases fibrin levels, possibly further increasing the DVT rate. 16 Incidence of DVT has been linked to increased mortality in patients with cancer. 17 Chemotherapy has been proven to increase DVT incidence 18 ; the DVT rate of patients being treated with fluorouracil and leucovorin for colorectal cancer was 15%. 8 A new modality of colorectal cancer treatment, the vascular endothelium growth factor (VEGF) antibody bevacizumab (Avastin) has also been shown to increase DVT by 3% to 4% over previously used chemotherapy regimens. 19 Only 3.1% of our study population had received recent chemotherapy. The use of erythropoietin has been associated with DVT as well, with 23.8% of patients experiencing DVT, and the combination of erythropoietin and bevacizumab has been associated with a 30% rate. 20 The incidence rate of VTE is highest in the first few months after the diagnosis of cancer, and it decreases over time thereafter, the risk of VTE is higher in patients with coexisting chronic medical illnesses and development of VTE is clearly associated with decreased survival. 7
Fleming et al 21 recently reported that after colorectal surgery for cancer and noncancer patients, the incidence of post-discharge VTE is 0.47%, this is slightly lower as compared to our findings likely because we focused exclusively on patients with malignancy. We demonstrated that the risk for diagnosis of postoperative VTE is fairly constant until POD 9 and thereafter decreases gradually in this surgical cohort. Our follow-up did not extend beyond 30 days and it is possible that the risk persists well beyond that time frame; in acutely ill medical patients symptomatic VTE events occurred between days 21 and 90. 22 Investigators for the @RISTOS project reported that 40% of VTE events occurred later than 21 days after surgery. 23 Almost one third of 30-day postoperative VTE in this patient population are diagnosed after discharge from the surgical hospitalization. Together these observations indicate the risk for VTE extends further perhaps, than many clinicians have realized and this study contributes significantly to our understanding of the duration and timing of VTE risk.
There is accumulating evidence that prophylaxis practice in surgical patients is suboptimal24,25 and there is difference in practice between surgical specialties. 26 Furthermore, as hospital stay becomes shorter, patients may not receive a 7- to 10-day regimen of VTE prophylaxis. Often patients who should receive extended duration prophylaxis (certain orthopedic surgery procedures) do not receive appropriate outpatient prophylaxis. 27 A recent study by Rasmussen et al 28 demonstrated that the 4-week administration of dalteparin, 5000 IU once daily, after major abdominal surgery, significantly reduces the rate of VTE, without increasing the risk of bleeding, compared with 1 week of thromboprophylaxis.
The extent and type of prophylaxis is not available in the ACS NSQIP data set, and this is one of the limitations of our study. Also our follow-up is limited to 30 days. There is evidence that the risk for VTE may persist up to 6 months. 29 We thus cannot determine whether the prothrombotic stimulus of surgery extends for a significant period after discharge, or if the clinical symptoms of VTE take this long to develop and the diagnosis to be established. Huo et al reported that in separate meta-analyses extended-duration thromboprophylaxis with LMWH (28-45 days) was associated with significant reductions in the likelihood of symptomatic VTE compared with standard-duration thromboprophylaxis in patients undergoing major orthopedic surgery (OR = 0.38; 95% confidence interval [CI], 0.24-0.61) or major abdominal or pelvic surgery (Peto OR = 0.22; 95% CI, 0.06-0.80). 30 We do not know whether thromboprophylaxis was used during the hospital stay and whether it was discontinued after discharge for these patients. Furthermore since part of the post-discharge follow-up was via phone calls and letters, there might have been VTE cases that were missed. Nevertheless, the broad number of hospitals and large sample do allow us to state these data are representative of the current practice relative to prophylaxis and the large patient population and clinical rigor of 30-day follow-up in the ACS NSQIP data set make these observations possible and represent the strengths of this study.
Conclusion
Our study indicates that almost one third of VTE in patients undergoing abdominal operations for colorectal cancer are diagnosed after discharge, likely secondary to hypercoagulability that persists for an extended period after surgery. This is one subgroup of patients that according to the 2008 ACCP guidelines 3 should receive post-discharge prophylaxis; the optimal duration remains to be determined. Additional studies may identify other patient groups in similar risk.
Footnotes
Acknowledgments
The American College of Surgeons National Surgical Quality Improvement Program and the hospitals participating in the ACS NSQIP are the source of the data used herein; they have not verified and are not responsible for the statistical validity of the data analysis or the conclusions derived by the authors.
Appendix A
Table A1. Number of Cases Included and Percentage by Primary Procedure CPT Codea
| Primary Procedure CPT Code | Number of Cases | Percent |
|---|---|---|
| 44140 | 5245 | 23.9 |
| 44141 | 298 | 1.4 |
| 44143 | 619 | 2.8 |
| 44144 | 283 | 1.3 |
| 44145 | 2273 | 10.4 |
| 44146 | 681 | 3.1 |
| 44147 | 132 | .6 |
| 44150 | 343 | 1.6 |
| 44151 | 8 | .0 |
| 44155 | 199 | .9 |
| 44156 | 8 | .0 |
| 44157 | 41 | .2 |
| 44158 | 57 | .3 |
| 44160 | 2390 | 10.9 |
| 44188 | 203 | .9 |
| 44204 | 2814 | 12.8 |
| 44205 | 1410 | 6.4 |
| 44206 | 84 | .4 |
| 44207 | 1076 | 4.9 |
| 44208 | 153 | .7 |
| 44210 | 70 | .3 |
| 44211 | 60 | .3 |
| 44212 | 38 | .2 |
| 44213 | 42 | .2 |
| 44650 | 5 | .0 |
| 45110 | 1354 | 6.2 |
| 45111 | 384 | 1.7 |
| 45112 | 189 | .9 |
| 45113 | 50 | .2 |
| 45114 | 32 | .1 |
| 45119 | 329 | 1.5 |
| 45121 | 6 | .0 |
| 45126 | 97 | .4 |
| 45135 | 1 | .0 |
| 45136 | 8 | .0 |
| 45160 | 14 | .1 |
| 45170 | 684 | 3.1 |
| 45395 | 156 | .7 |
| 45397 | 83 | .4 |
| 45402 | 6 | .0 |
| 45499 | 18 | .1 |
| Total | 21943 | 100.0 |
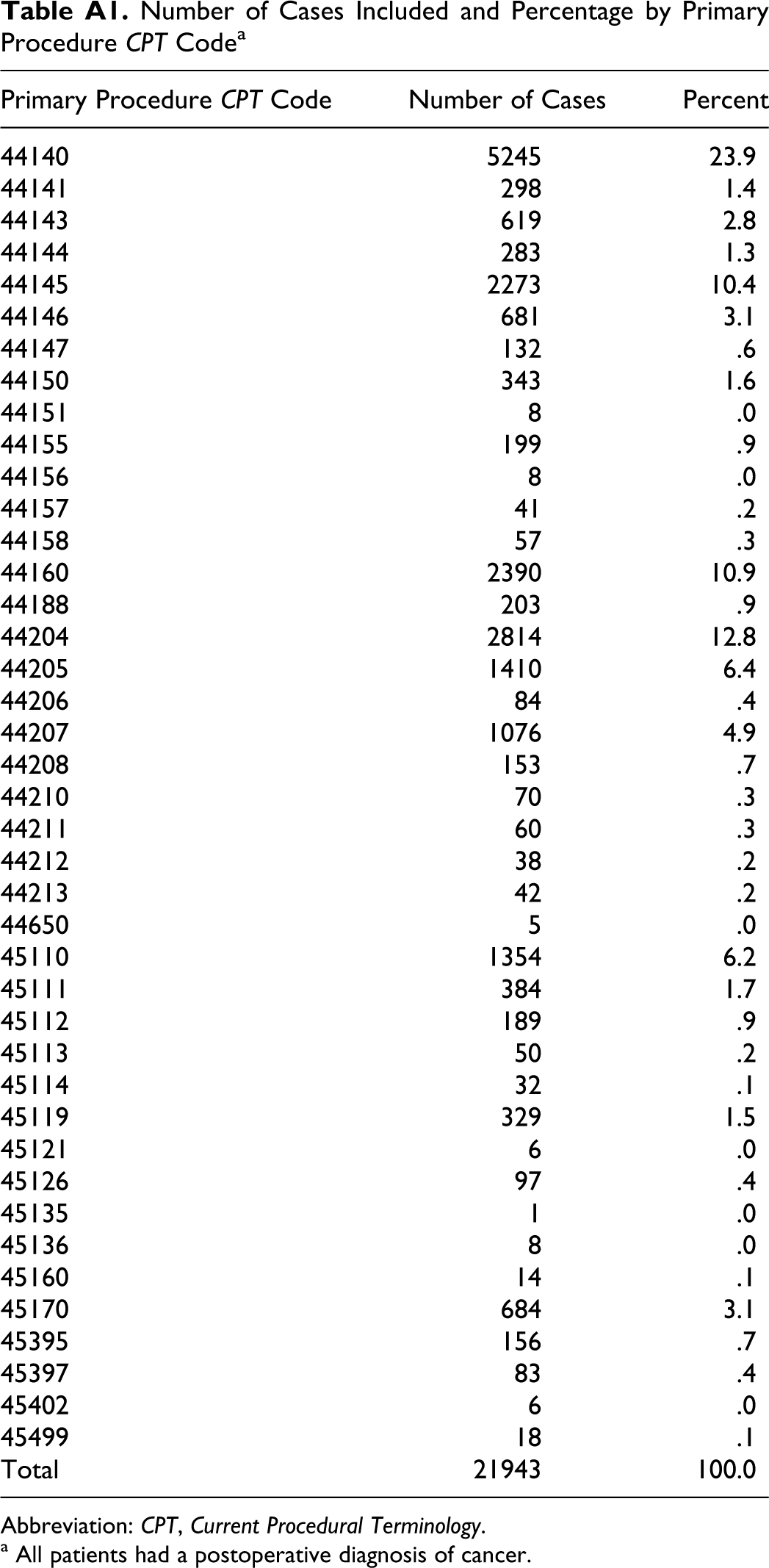
Abbreviation: CPT, Current Procedural Terminology.
a All patients had a postoperative diagnosis of cancer.
Authors’ Note
This paper was presented at the Southern Association for Vascular Surgery Annual Meeting, January 18-22, 2011, Naples, FL, USA.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.