
Abstract
The aim of the study is to investigate the association between the severity of rheumatic mitral valvular disease (RMVD) and the neutrophil–lymphocyte ratio (NLR). A total of 227 patients were enrolled in the study and divided into 3 groups. Patients in group 1 had rheumatic mitral stenosis (RMS), those in group 2 had RMVD without stenosis, and those in group 3 served as the control group. Group 1 was further divided into 2 groups, severe mitral stenosis (MS) and mild to moderate MS. The NLR was significantly higher in patients with severe MS when compared to those with mild to moderate MS (P = .002) while lymphocyte count was lower (P = .034). Using a cutoff level of 2.56, the NLR predicted severe RMS with a sensitivity of 75% and specificity of 74%. In conclusion, as an inexpensive, simple, and accessible marker of inflammation, the NLR may be useful in predicting the presence and severity of MS in patients with RMVD.
Introduction:
Rheumatic heart disease (RHD) continues to be a major health problem despite advances in diagnostic and treatment modalities. The RHD causes cardiac morbidity and mortality, especially in children and young adults in developing countries. 1,2 Mitral stenosis (MS) is a complication of RHD that leads to significant morbidity and mortality in developing countries although its prevalence has decreased in developed countries. 3
A blood marker that could discriminate patients who are at high risk to develop MS would be beneficial to decreasing the morbidity and mortality of this disease. Previous studies have shown that patients with RHD have continuous (persistent) chronic inflammation. 4 –9 Since RHD is a disease of underdeveloped countries with limited resources and technical facilities, inflammatory markers are rarely used in daily practice. Therefore, there is a need for simple, inexpensive, and easily obtainable biochemical markers that can be used in daily practice.
Recently, it was reported that the neutrophil–lymphocyte ratio (NLR) is an important marker of inflammation in several disorders, especially cardiovascular diseases 10,11 and cancer. 12
Since it has been hypothesized that the NLR may reflect ongoing inflammation, we sought to investigate the relationship between the NLR and the severity of rheumatic mitral valvular disease (RMVD).
Methods
Study Population
In all, 145 patients with RMVD who were admitted to our clinic between January 2012 and June 2013 were enrolled in the study. In all, 82 age- and sex-matched healthy participants were included in the control group. Patients with acute infection, chronic inflammatory disorders, coronary artery disease, pregnancy, diabetes mellitus, hypertension, chronic renal or hepatic disease, hematological malignancies, and those who did not undergo a blood analysis were excluded from the study. Patients with RMVD were divided into 2 groups according to the presence of MS (group 1 included patients with MS, while group 2 included patients with RMVD without stenosis). Group 3 consisted of the healthy participants (control group). Group 1 was further divided into 2 subgroups according to the degree of stenosis, which included those with severe MS and those with mild to moderate MS. Total and differential leukocyte counts were measured by an automated hematology analyzer (Abbott Cell-Dyn 3700; Abbott Laboratory, Abbott Park, Illinois). Absolute cell counts were used in the analyses.
Transthoracic Echocardiography
All measurements were performed with a commercially available ultrasound system (GE Vivid S5; Vingmed System Five, Horton, Norway) according to the recommendations of the American Society of Echocardiography. 13 Mitral valve area (MVA) was measured with the pressure half-time method, and the transmitral gradient was determined with a continuous wave Doppler in apical 4-chamber view. Criteria for the diagnosis of rheumatic MS (RMS) included MVA ≤2 cm2, the presence of commissural fusion, leaflet thickening, and alteration of the subvalvular apparatus, documented by an echocardiogram. 14 Patients having a MVA ≤1.0 cm2 were considered severe, while those with an MVA >1.0 cm2 were classified as having mild to moderate MS.
Statistical Analysis
Continuous variables are presented as mean ± standard deviation, while categorical variables are given as percentages. The Kolmogorov-Smirnov test was used to verify the normality of the distribution of continuous variables. The independent sample t test or the Mann-Whitney U test was used for the continuous variables, and the chi-square test was used for categorical variables. One-way analysis of variance or Kruskal-Wallis tests was used to evaluate comparisons between the 3 groups. Post hoc analysis was carried out by Tukey test. Correlations were assessed with the Spearman rank test. Receiver–operating characteristic (ROC) curve analysis was used to determine the optimum cutoff levels of NLR that would predict the severity of RMS, and results are shown as odds ratios with 95% confidence intervals (CIs). Statistical analyses were performed using SPSS 16.0 (SPSS Inc, Chicago, Illinois). A 2-tailed P < .05 was considered as statistically significant.
Results
A total of 106 patients were diagnosed with RMS. In all, 12 patients who did not have concomitant laboratory data, 2 patients with acute infection, 2 patients with hypertension, and 1 diabetic, 1 pregnant, and 1 patient with severe anemia were excluded from the study. A total of 227 patients (178 female, mean age 41 ± 10 years) were included in the study. After the initial evaluation, 87 patients with RMS (72 female, mean age 42 ± 12 years, range 18-69 years), 58 patients with chronic rheumatic valve disease without MS (54 female, mean age 39 ± 8 years, range 25-57 years), and 82 healthy controls (52 female, mean age 42 ± 10 years, range 19-68 years) were assessed. There were no differences between the ages and the genders of the groups. Left ventricular ejection fraction (LVEF) was within the normal range in all patients (≥55%), but it was statistically lower in patients with RMS than in the other 2 groups. The patients in group 1 (MS) had higher NLR (Figure 1), creatinine, mean platelet volume values, and higher white blood cell (WBC) and neutrophil counts, while having lower hemoglobin, hematocrit values, and lymphocyte counts than the other 2 groups. In post hoc analysis, NLR and neutrophil counts were significantly higher in group 1 (P < .001). Lymphocyte count was different only between group 1 and 3 (P = .005). Groups 2 and 3 were similar with respect to NLR level, neutrophil, and lymphocyte counts. There was no statistically significant difference between group 2 (RMVD without stenosis) and group 3 (control) in terms of WBC, neutrophil, and lymphocyte counts or NLR and LVEF values. Hematocrit and hemoglobin levels were significantly lower while the left atrial diameter was significantly higher in group 2 (RMVD without stenosis). Baseline demographic and clinical characteristics of the study patients are shown in Table 1.
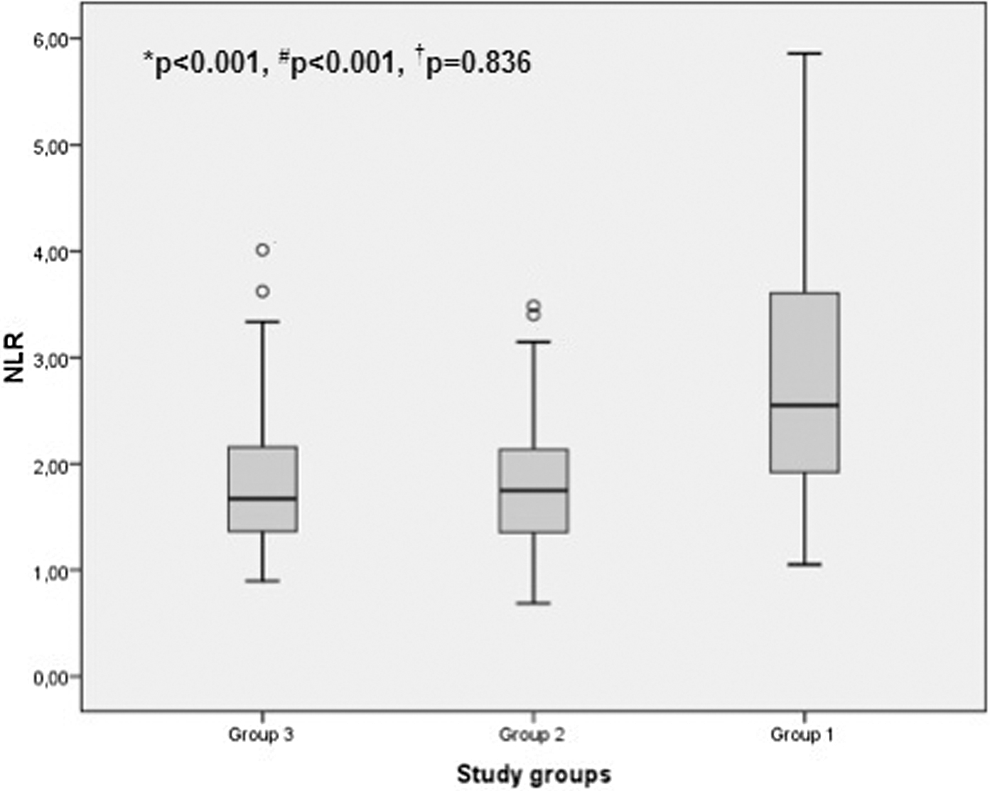
Box plot graph showing the neutrophil to lymphocyte ratios in control, rheumatic valvular disease without and with mitral stenosis, respectively (P value for *groups 1 and 2,
Baseline Demographic and Clinical Characteristics of the Study Groups.
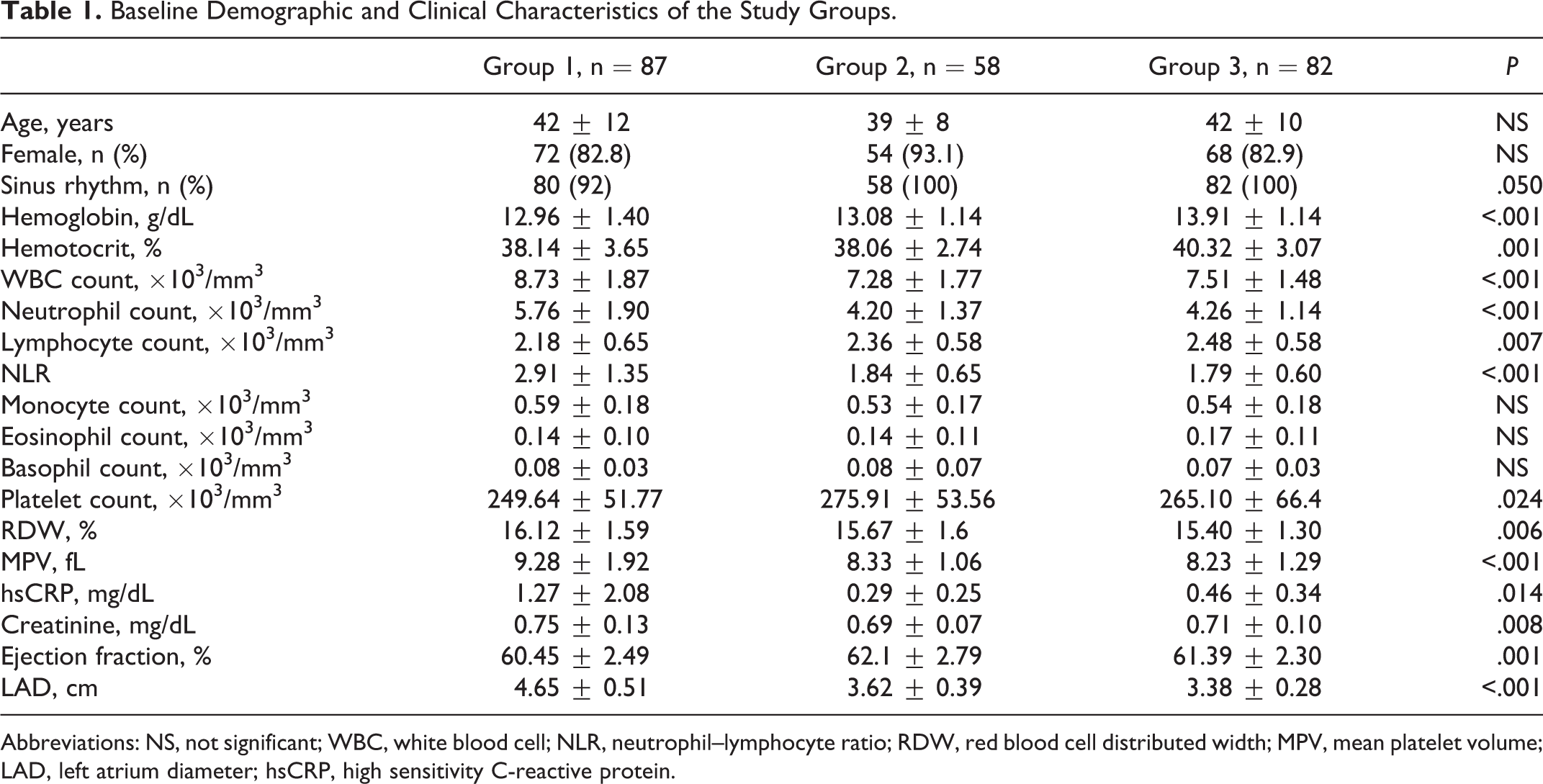
Abbreviations: NS, not significant; WBC, white blood cell; NLR, neutrophil–lymphocyte ratio; RDW, red blood cell distributed width; MPV, mean platelet volume; LAD, left atrium diameter; hsCRP, high sensitivity C-reactive protein.
Of the 87 patients with RMS, mean MVA was 1.3 ± 0.29 cm2 (range: 0.7-2.0), transmitral mean gradient was 11.51 ± 5.37 mm Hg (range: 5-27), left atrial diameter was 4.65 ± 0.51 cm (range: 3.5-6.4), and systolic pulmonary arterial pressure was 45.9 ± 16 mm Hg (range: 25-115). Atrial fibrillation was present in 7 (8%) patients.
Patients with severe RMS had significantly higher NLR levels than those with mild to moderate RMS (3.72 ± 1.35 vs 2.66 ± 1.24, z = 3.067, P = .002; respectively; Figure 2). Neutrophil and lymphocyte counts were significantly different between patients with severe RMS and those with mild to moderate MS, while the total WBC counts were similar (neutrophil count 6.43 ± 1.95 vs 5.56 ± 1.86, z = 2.038, P = .042; lymphocyte count 1.87 ± 0.66 vs 2.26 ± 0.64, z = 2.119, P = .034; respectively). Clinical and laboratory features of the RMS subgroups are shown in Table 2. Correlation analysis revealed that the NLR had a significant negative correlation with MVA (r = 0.275, P = .01).
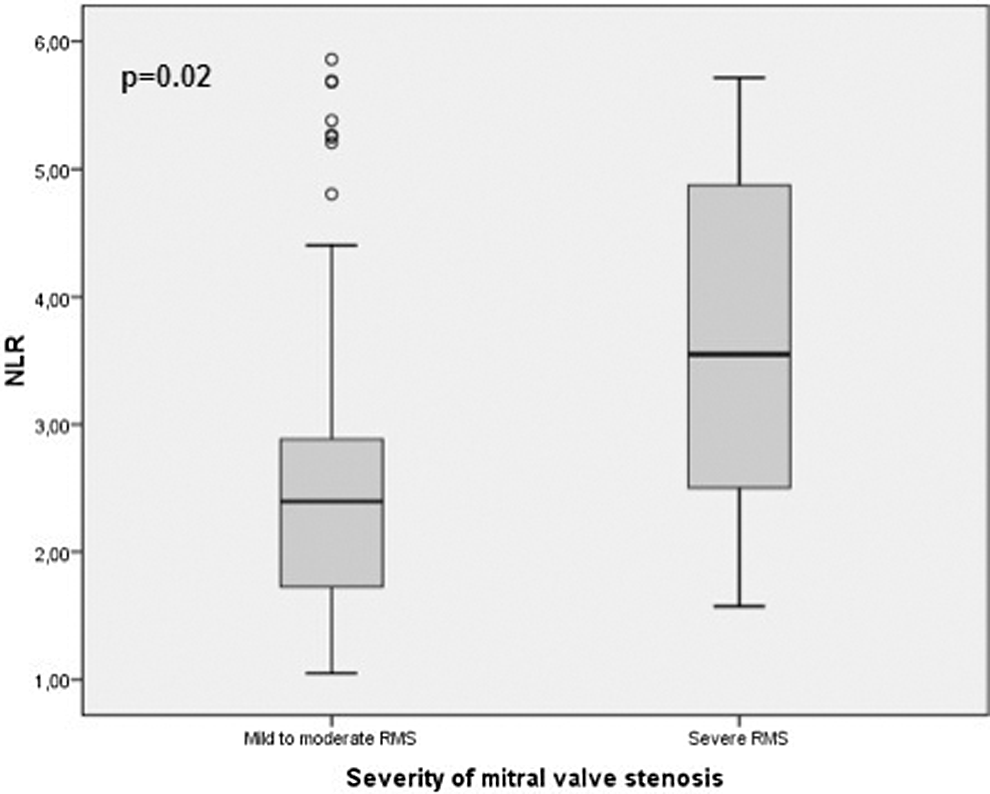
Box plot graph showing the neutrophil to lymphocyte ratios in subgroups of rheumatic mitral stenosis. RMS indicates rheumatic mitral stenosis.
Clinical and Laboratory Features of Rheumatic Mitral Stenosis Subgroups.
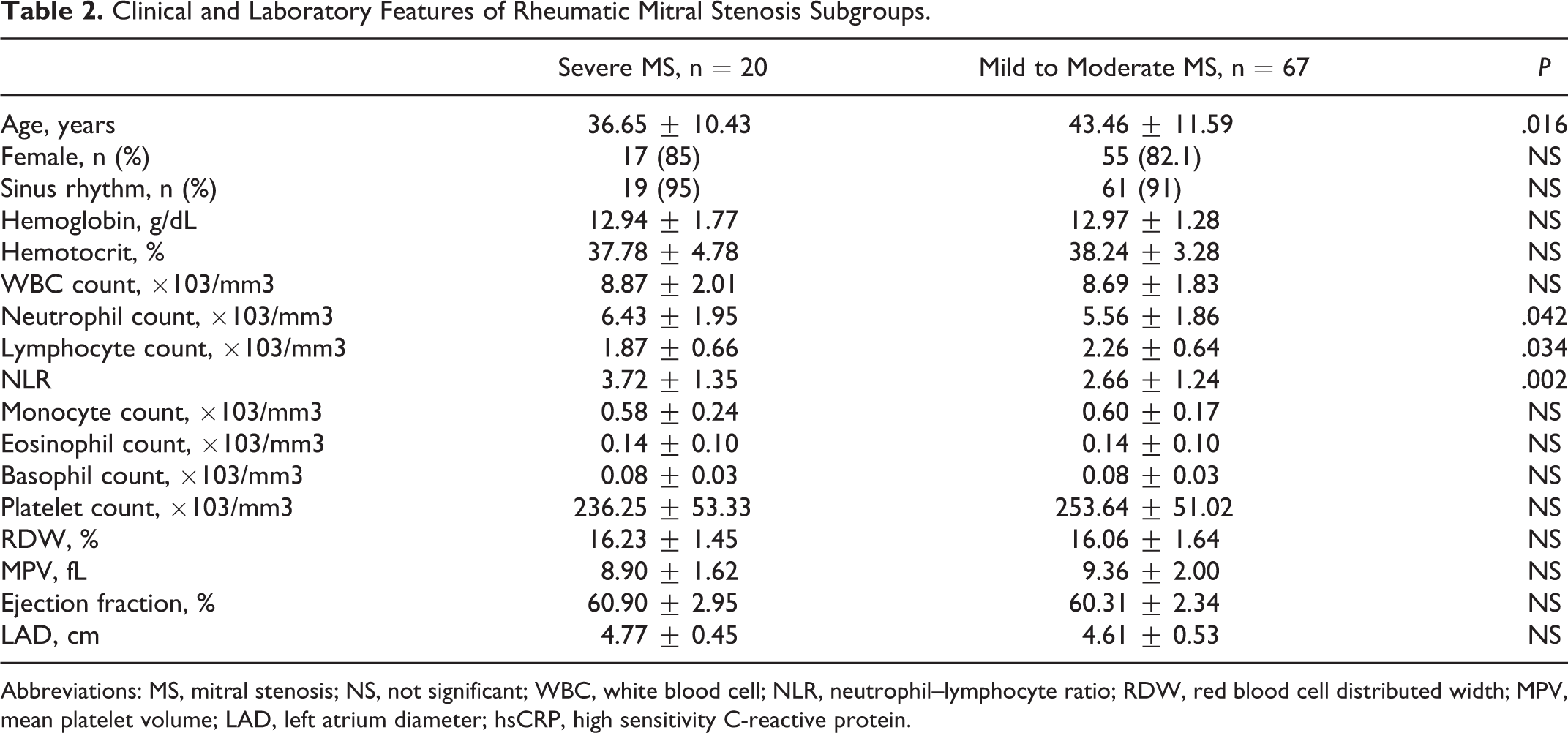
Abbreviations: MS, mitral stenosis; NS, not significant; WBC, white blood cell; NLR, neutrophil–lymphocyte ratio; RDW, red blood cell distributed width; MPV, mean platelet volume; LAD, left atrium diameter; hsCRP, high sensitivity C-reactive protein.
Using a cutoff level of 2.56, the NLR predicted severe MS with a sensitivity of 75% and specificity of 74% in patients with rheumatic valve disease (ROC area under curve: 0.81, 95% CI: 0.71-0.90; Figure 3).
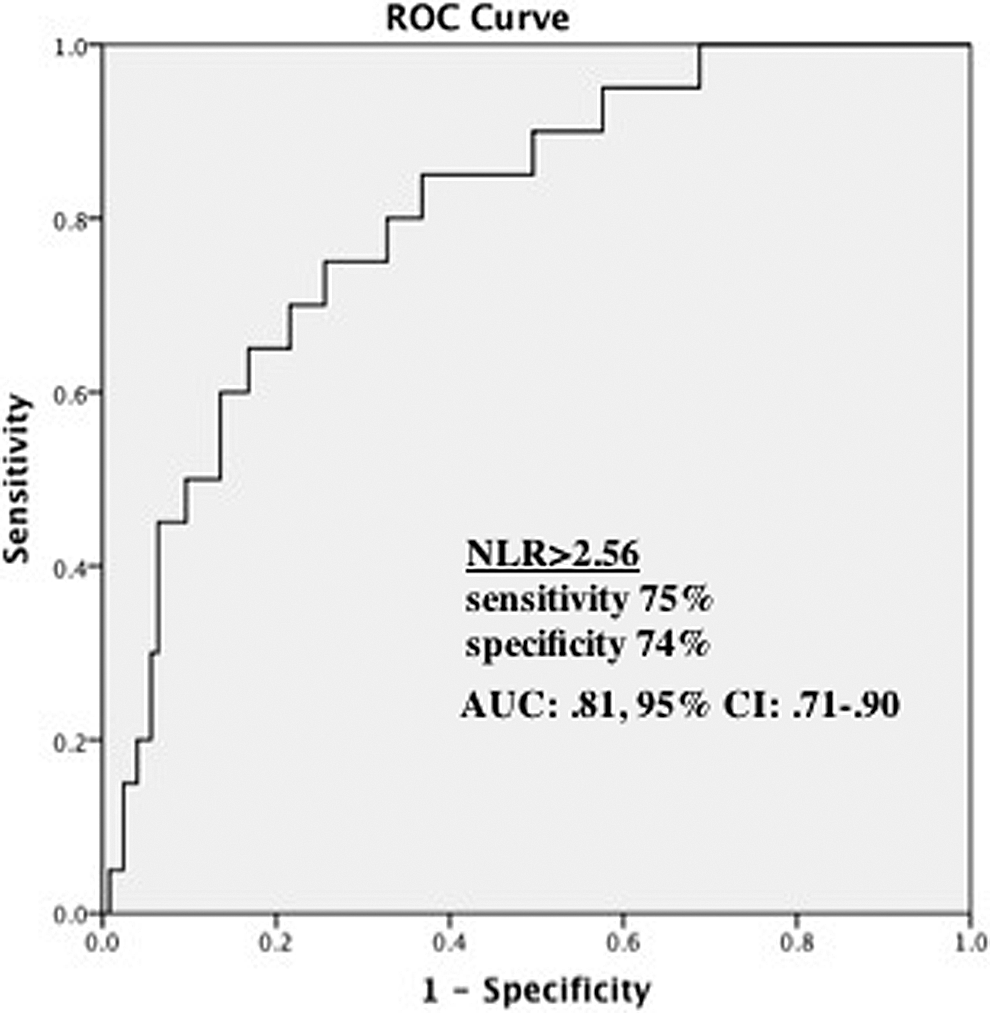
The receiver–operating characteristic (ROC) curve analysis of neutrophil to lymphocyte ratio for predicting severe mitral stenosis. AUC indicates area under curve; CI, confidence interval; NLR, neutrophil to lymphocyte ratio.
Discussion
The NLR is significantly higher in patients with RMS compared to those with RMVD without stenosis and control patients. The NLR positively correlated with the degree of stenosis, and it was significantly higher in patients with severe RMS as compared to those with mild-to-moderate stenosis. Moreover, our study showed that an NLR >2.56 predicts the presence of severe RMS with a sensitivity of 75% and specificity of 74% among patients with RMVD.
Previous reports have shown convincing evidence that there is ongoing inflammation in rheumatic valvular disease. Intralesional mononuclear cells that are secreting inflammatory cytokines have been identified in the chronic phase of rheumatic valvular disease. 6 Although there are no infectious agents in the chronic phase of rheumatic valvular disease, there is persistent inflammation that causes the destruction of the valve. 6 Similarly, evidence of active inflammation has been previously noted in pathological specimens of excised rheumatic mitral valves. 15
In a study by Golbasi et al, levels of high-sensitivity C-reactive protein (hsCRP) were higher in patients with chronic rheumatic valvular disease than in healthy participants and patients with valve replacement. 8 Similarly, in a study conducted on patients with RMS, hsCRP levels were significantly higher in patients with RMS than in the control group, and hsCRP values correlated with the Wilkins valve score and its components. 16
In a study by Davutoglu et al, patients with RMVD had increased levels of chronic inflammatory markers (plasma levels of interleukin [IL]-6, IL-8, IL-2 receptor, tumor necrosis factor α, and hsCRP) as indicators of ongoing inflammation compared with the control group. Further, their levels were associated with valve involvement, valve thickness, and the severity of subvalvular calcification. 9
In addition, hsCRP (a marker of persistent chronic inflammation) levels were higher in children with RHD compared to the control group, and hsCRP levels were correlated with the degree and severity of the valve involvement. 7 Unlike our study, which only included adults, children were included in this study, and the severity of valve involvement was determined by the degree of mitral valve regurgitation. 7
Kaya et al detected a significant positive correlation between the hsCRP and the NLR in patients with RMS. 17 In this study, only patients with RMS were included, and patients with and without spontaneous echo contrast were compared in terms of NLR. Also Turak et al found a significant relationship between the NLR and the in-hospital mortality and cerebrovascular events in patients with infective endocarditis. 18
In our study, the hsCRP assay was available only for 33 patients with rheumatic valvular disease. In accordance with the aforementioned studies, the NLR had a positive and significant correlation with hsCRP. Also, we found that the NLR was related to the degree/severity of valve stenosis. Since patients with severe MS had significantly higher NLR levels compared to those mild to moderate MS, this is an indication that the NLR may be a useful marker of the increased inflammatory status in patients with rheumatic valvular disease.
Many studies have shown that higher levels of NLR are associated with increased inflammation in various cardiovascular diseases. High NLR levels have been found to be independent predictors of the severity of coronary artery disease, 19 slow coronary flow phenomenon 20 arterial stiffness, and coronary calcium scores. 21
In a review that included more than 34 000 patients, the NLR was shown to be a simple, readily available inflammatory marker for the risk stratification of patients with acute coronary syndrome or for whom revascularization was performed. 22
Increased levels of NLR, as a marker of inflammation, have been associated with increased mortality in patients with stable coronary artery disease 23 and those undergoing coronary angiography 24 and percutaneous coronary intervention. 25 In addition, higher NLR levels were associated with an increased risk of long-term mortality in patients admitted with acute decompensated heart failure (HF). 26
In addition to other parameters used for risk stratification in various cardiovascular diseases, a recent review has shown the NLR to be a simple, easily obtainable marker of inflammation. 10 Similarly, in patients with chronic renal failure, the NLR was found to be correlated with the standard inflammatory markers hsCRP and IL-6. 27 The NLR was significantly increased in patients with pulmonary arterial hypertension, for which inflammation plays a key role in the pathophysiology. 28
The NLR was also increased in certain types of cancer in which inflammation is prominent. In a review including a large number of patients (>37 000) with various types of cancers, the NLR anticipated the clinical prognosis, and it was associated with other markers of inflammation, in particular with hsCRP. 12 Elevation in the NLR is associated with hypoalbuminemia, suggesting that the NLR may be able to demonstrate the malnutrition status of patients with cancer. 12
Decreased lymphocyte count has been associated with malnutrition and lymphopenia and is used as an indicator of malnutrition. 29 A decrease in lymphocyte count increases NLR. As rheumatic valvular disease is generally observed in underdeveloped countries, malnutrition may contribute to its development. Previously, protein energy malnutrition has been shown to be associated with rheumatic fever. 30 The weights 31 and serum albumin levels 32 of patients with rheumatic valvular disease are lower than patients without.
In our study, patients with RMS had significantly lower lymphocyte counts than those of the other 2 groups. We hypothesize that this may be due to malnutrition; and therefore, further studies should include tests to determine malnutrition status.
Mean platelet volume (MPV) was significantly higher in patients with RMS compared to those without MS. Platelet activity is known to increase as a result of the damaged valve and nonlaminar flow, and it has also been shown that increased MPV levels reflect the presence of activated platelets. 33,34
Study limitations
The most important limitation of this study is that it was a single-center, retrospective study. Using three-dimensional echocardiography to evaluate MVA would have provided a more accurate assessment of stenosis. Another limitation is that we did not simultaneously measure generally accepted markers of inflammatory and malnutrition status while measuring NLR.
Conclusion
The NLR, which is an inexpensive, readily available marker of persistent, chronic inflammation, may be useful in predicting the presence and severity of MS in patients with rheumatic mitral valve disease.
Footnotes
Acknowledgement
We are grateful to Dicle University DUBAP for their sponsorship about English editing of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.