
Abstract
Neutrophil/lymphocyte ratio (NLR) has been proposed as a prognostic marker to determine systemic inflammatory response and atherosclerosis. Our aim was to determine the relationship between NLR and development of coronary collateral circulation (CCC) in patients with stable coronary artery disease (CAD). A total of 521 consecutive patients with stable CAD who underwent coronary angiography and documented total occlusion in one of those major coronary arteries were included in this study. Levels of fasting blood glucose, white blood cell, and NLR were significantly higher in patients with poor collateral than in those with good collateral. After multivariate analysis, high level of NLR was an independent predictor of CCC together with levels of fasting blood glucose. The receiver–operating characteristic analysis provided a cutoff value of 2.75 for NLR to predict poor CCC with 65% sensitivity and 68% specificity. We demonstrated an independent association between levels of NLR and development of CCC in patients with stable CAD.
Introduction
Coronary collateral circulation (CCC) can provide an alternative source of blood supply to an ischemic myocardial area. Also, well-developed CCC can limit ischemic damage, reduce infarct size, and improve survival. 1 The heterogenecity in the degree of collateralization in patients with coronary artery disease (CAD) is not clearly established. The pathogenesis of development of the CCC is very complex, and it can be affected by many different factors. Additionally, there was a complex interrelation between new blood vessel formation and inflammation. 2 Several studies have been reported that inflammatory markers such as levels of monocytes and C-reactive protein (CRP) were related to development of CCC. 3,4 Investigators showed that systemic inflammatory response was associated with the presence of systemic atherosclerosis and development of CCC. 5 In addition, levels of white blood cell (WBC) and its subtypes (neutrophils, monocytes and lymphocytes) have been demonstrated as predictors of CAD. 6 In atherogenesis and atherothrombosis, leukocytes, especially neutrophils, play an important role. 7 Neutrophil–lymphocyte ratio (NLR) has been proposed as a prognostic marker to determine systemic inflammatory response too. 8 The NLR indicates the balance of the neutrophils (the active component of the inflammation), with the lymphocytes (the regulatory and protective component). 9 Several studies have suggested that high levels of NLR areassociated with adverse outcomes and increased cardiovascular mortality in patients with CAD. 10,11
According to the association between inflammation and CCC, in this study, our aim was to determine the relationship between NLR and development of CCC in patients with stable CAD.
Materials and Methods
Study Population
Between April 2011 and March 2013, a total of 521 (396 men and 125 women, with mean age 62 ± 11 years) consecutive patients with stable CAD who underwent coronary angiography in Adana Numune Education and Research Hospital and documented total occlusion in one of those major coronary arteries were included in this study. Patients with acute/chronic infective or inflammatory disease, chronic kidney disease (serum creatinine >2.0 mg/dL), a previous history of coronary artery bypass grafting (CABG), acute coronary syndrome within the last 3 months, severe valvular heart disease, malignancies, and congestive heart failure (with symptoms or left ventricular ejection fraction <45%) were excluded from the study. The risk factors of CAD such as age, sex, hypertension, smoking, and diabetes mellitus (DM) were recorded. The local ethical committee approved the study protocol, and informed written consent was obtained from each patient.
Coronary Angiography and Coronary Collateral Scoring
Standard selective coronary angiography was performed using Judkins technique. Coronary angiograms and collateral grading were examined by 2 experienced interventional cardiologists who were blinded to the clinical characteristics and laboratory results of the patients. Development of the CCC was graded according to the Cohen-Rentrop method, grade 0, no filling of any collateral vessels; grade 1, filling of side branches of the artery to be perfused by collateral vessels without visualization of epicardial segment; grade 2, partial filling of the epicardial artery by collateral vessels; and grade 3, complete filling of the epicardial artery by a collateral vessels. 12 Patients with grades 0 to 1 as poor CCC, and patients with grades 2 to 3 as good CCC were classified in our study. If the patient had more than 1 vessel with CCC, collateral grading was performed according to the vessel that had better antegrade or retrograde collateral.
Blood Samples and Laboratory Assay
All measurements were collected on admission and were sent to the laboratory within 30 minutes. Measurements of hematologic parameters were performed by an automatic blood counter (A Sysmex XE-2100, Symex, Kobe, Japan). Serum creatinine, alanine aminotransferase (ALT), aspartate aminotransferase (AST), and lipid profile were measured using an autoanalyzer (Roche DiagnosticModular Systems, Tokyo, Japan). The NLR was calculated.
Statistical Analysis
All analyses were performed using SPSS V 17.0 for windows (version 17.0; SPSS, Chicago, Illinois). Quantitative variables were expressed as mean value ± standard deviation for parametric variables and median and minimum–maximum levels for nonparametric variables. Comparison of parametric values between 2 groups was performed by means of independent samples t test. Comparison of nonparametric values between 2 the groups was performed by Mann-Whitney U test. Categorical variables were compared by the chi-square test. Logistic regression analysis was performed with enter method for multivariate analysis of independent predictors. The parameters that had significant P values (P < .05) and marginal insignificant P values (P < .1) were entered in the multivariate analysis. The receiver–operating characteristic (ROC) analysis were performed to determine the cutoff value of NLR in prediction poor CCC.
Results
A total of 521 patients with stable CAD (poor CCC group 295 patients and good CCC group 226 patients) were included in our study. Baseline characteristics and coronary angiographic findings are presented in Table 1. Both groups were similar in terms of age, sex, hypertension, smoking, the location of occluded vessel, and the number of diseased vessels. Compared with good CCC group, the poor CCC group had a significantly higher frequency of DM.
Baseline Characteristics and Coronary Angiographic Findings.
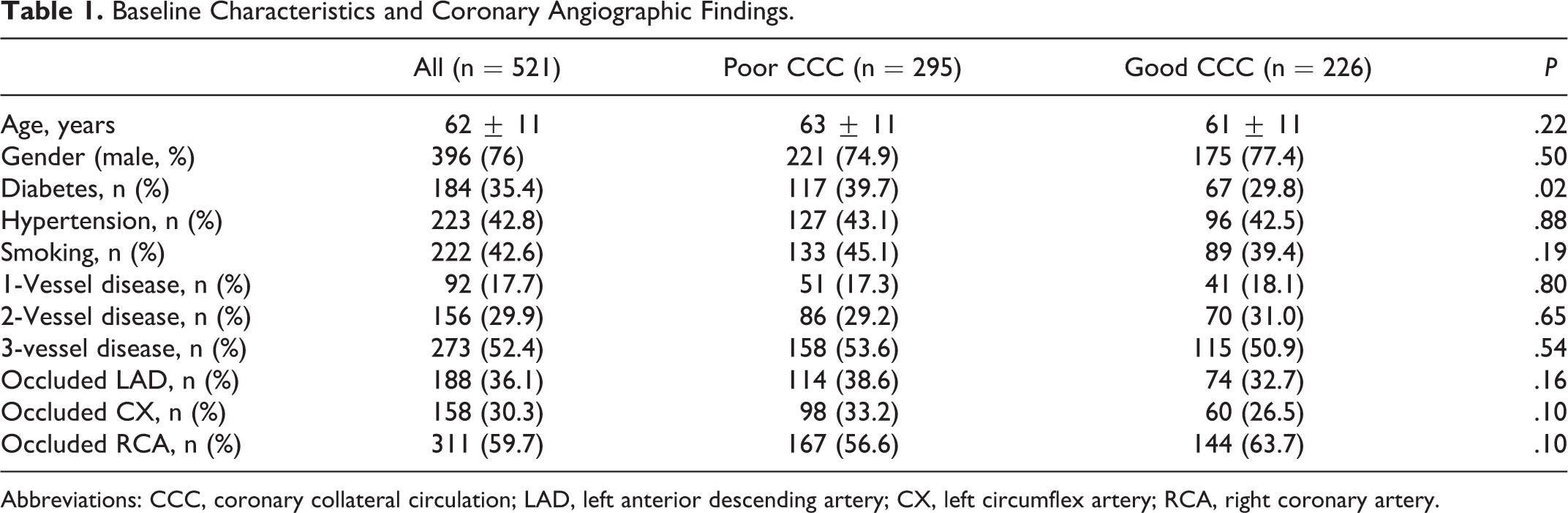
Abbreviations: CCC, coronary collateral circulation; LAD, left anterior descending artery; CX, left circumflex artery; RCA, right coronary artery.
In Table 2, levels of creatinine (Cr), ALT, AST, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and triglyceride were similar in both the groups. Levels of fasting blood glucose (P < .01), WBC (P < .01), and NLR (4.25 ± 3.2 vs 2.75 ± 1.2, P < .01) were significantly higher in patients with poor collateral than good collateral. Also, levels of hemoglobin (P = .05) and platelets (P = .05) had a marginal insignificant P value. An inverse stepwise relation was present between NLR and collateral scores (Figure 1).
Comparison of Laboratory Parameters Between Poor and Good CCC Groups.
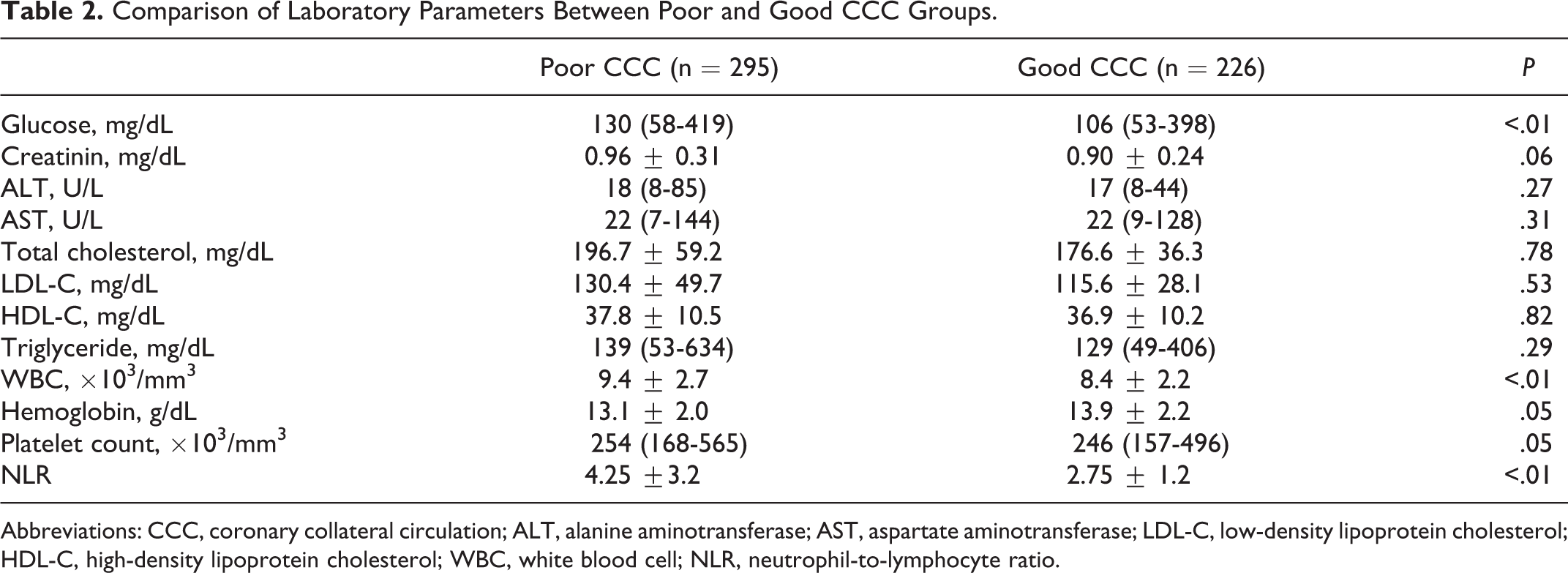
Abbreviations: CCC, coronary collateral circulation; ALT, alanine aminotransferase; AST, aspartate aminotransferase; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; WBC, white blood cell; NLR, neutrophil-to-lymphocyte ratio.
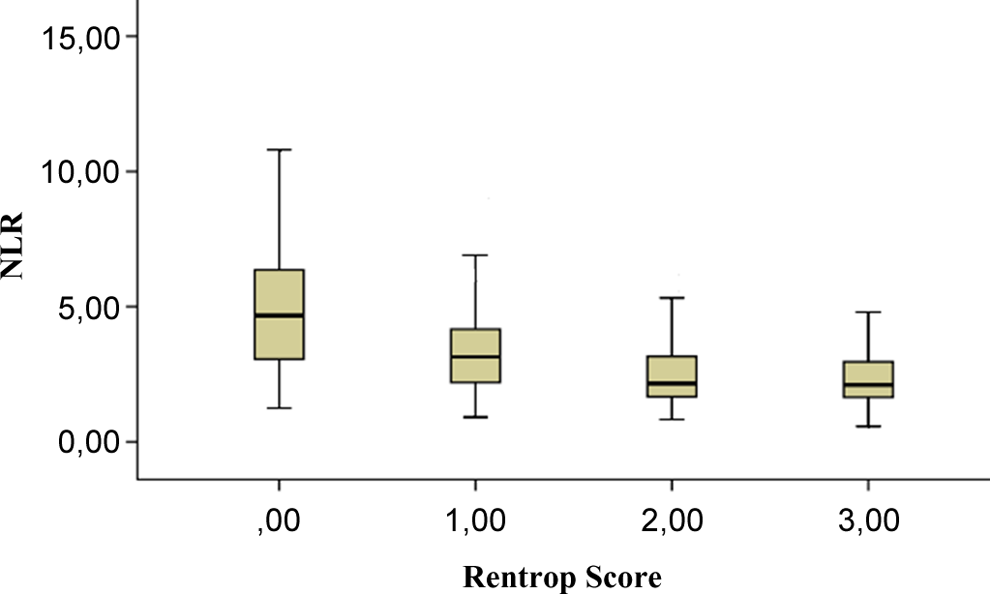
Relationship between neutrophil-to-lymphocyte ratio (NLR) and Rentrop score (error bars: 95% confidence interval [CI]).
The parameters which had significant P values (P < .05) were entered in the univariate analysis, and marginal insignificant P values (P < .1) were entered in the multivariate analysis (DM, WBC, fasting blood glucose, hemoglobin, platelets, and NLR). After multivariate analysis, high levels of NLR was an independent predictor of CCC (odds ratio [OR] 0.70, 95% confidence interval [CI] 0.62-0.80; P < .01) together with levels of fasting blood glucose (OR 0.995, 95% CI 0.991-0.999; Table 3).
Results of Multivariate Logistic Regression Analysis.
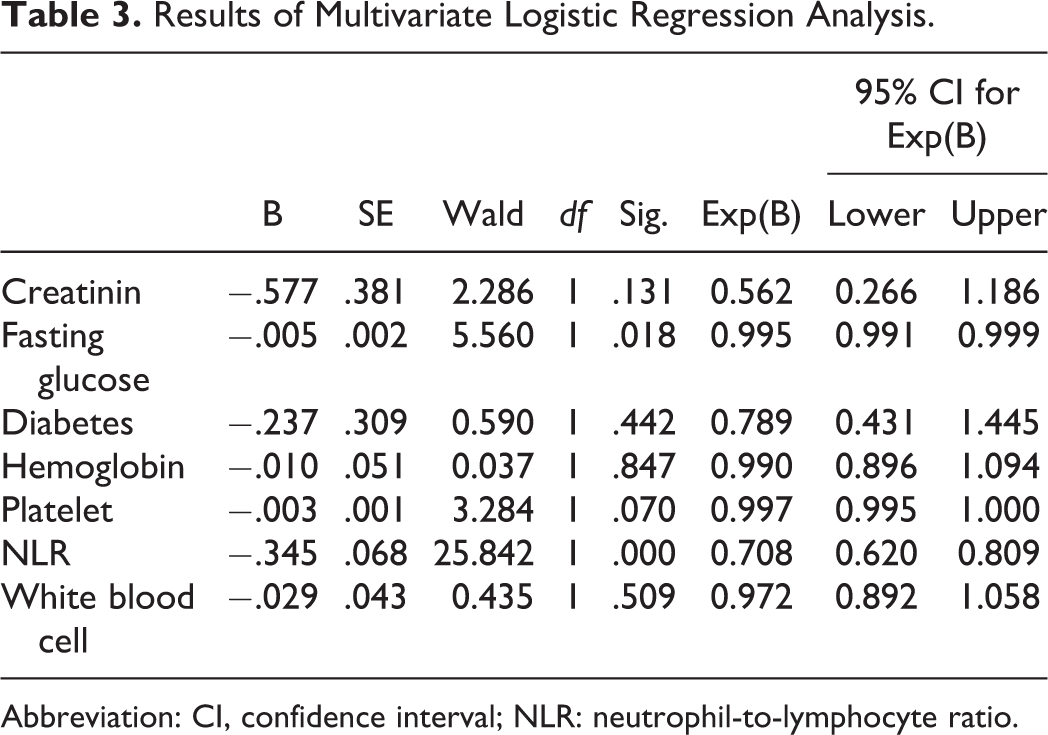
Abbreviation: CI, confidence interval; NLR: neutrophil-to-lymphocyte ratio.
The ROC analysis provided a cutoff value of 2.75 for NLR to predict poor CCC with 65% sensitivity and 68% specificity, with the area under the ROC curve being 0.714 (95% CI 0.66-0.75, Figure 2).
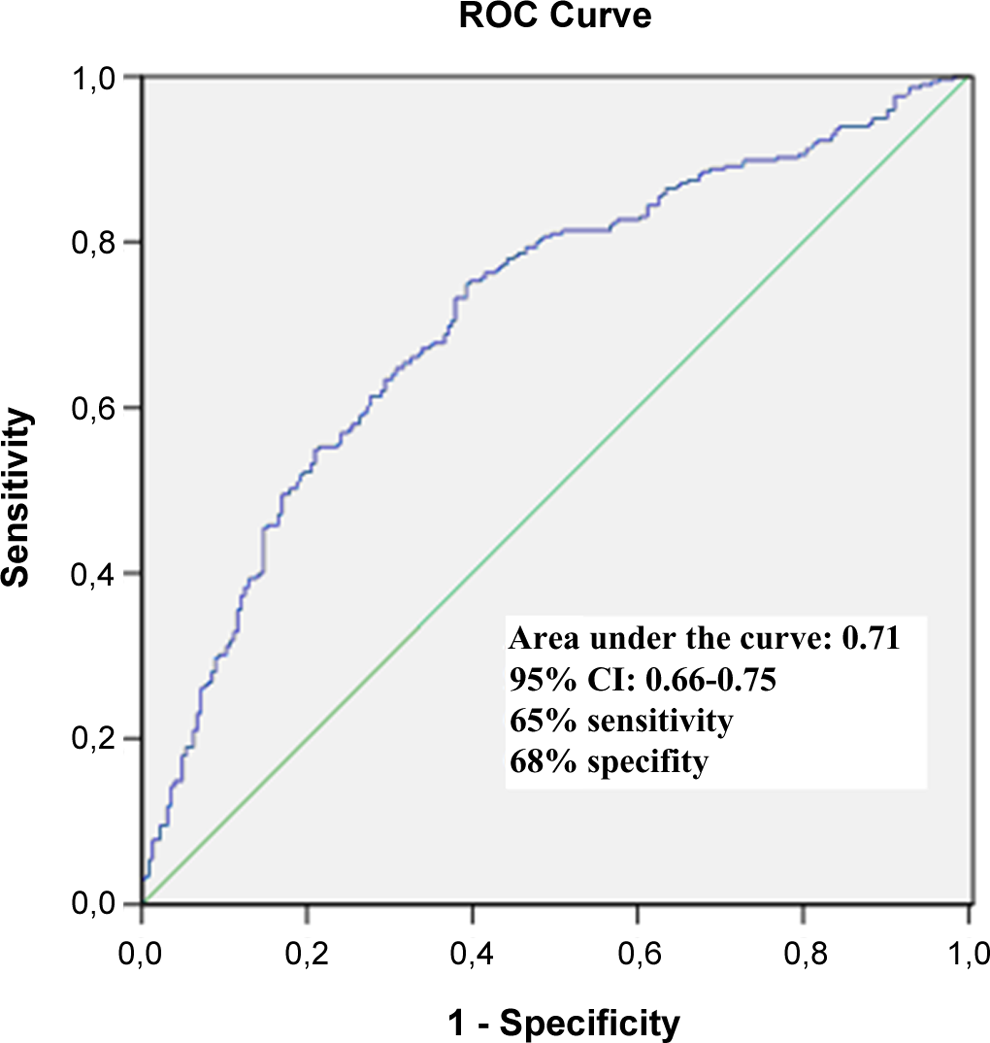
Receiver–operating characteristic curve analysis for neutrophil-to-lymphocyte ratio (NLR) for prediction of poor collateral.
Discussion
Neutrophil/lymphocyte ratio has been proposed as a new prognostic marker in patients with CAD. In our study, we demonstrated an independent association between levels of NLR and development of CCC in patients with stable CAD. Additionally, our study showed that level of NLR > 2.75 predicted poor collateral with a sensitivity of 65% and specificity of 68%.
The complex mechanisms underlying development of CCC are not well understood. Inflammation plays a central role at all stages of atherosclerosis as well as in development of CCC. 2 There was a complex interrelation between new blood vessel formation and inflammation. 2 Kerner et al reported an inverse-graded association between CRP and the presence of coronary collaterals in patients with stable angina pectoris. 4 In a study, Verma et al demonstrated that CRP directly represses NO synthesis, so CRP could inhibit angiogenesis. 13 Moreover, Schneeweis et al showed that CRP inhibited endothelial cell migration induced vascular endothelial growth factor. 14
Another markers of inflammation, such as levels of WBC and its subtypes (neutrophils, monocytes and lymphocytes), have been demonstrated as predictors of CAD. 6 High levels of neutrophil and low levels of lymphocyte were predictors of future cardiovascular events. 6,15 A higher NLR indicates a higher level of inflammation. 8 The interrelation between neutrophils and endothelium has been accused to cause increased damage to the endothelium and reported by Ott et al to platelet adhesion in patients with unstable angina. 16 Therefore, we hypothesized that the association between NLR and poor CCC could be elucidated with endothelial dysfunction and elevated inflammatory response. Several studies have suggested that high levels of NLR were associated with adverse outcomes and increased cardiovascular mortality in patients with unstable angina pectoris, non-ST-segment elevation myocardial infarction, ST-segment elevation myocardial infarction and in patients undergoing CABG, and primary percutaneous coronary intervention. 17 –20 In addition, NLR was related to the presence of isolated coronary artery ectasia and the complexity of CAD and the stent restenosis in patients with stable and unstable angina. 21,22 Kaya et al found an independent association between NLR and contrast-induced nephropathy. 11
Similar to previous studies, our study has confirmed the negative association between DM and development of CCC. Fasting blood glucose has been found as an independent predictor of poor collaterals. Kadi et al showed that coronary collateral development was impaired in patients with prediabetes when compared to patients with CAD who had normal fasting glucose level. 23 In another study, Mouquet et al demonstrated that in patients with coronary occlusion, collateral circulation was impaired in patients with metabolic syndrome (MS), and this association was partly related to fasting glycemia and to key parameters linked to insulin resistance. 24
Study Limitation
We did not evaluate inflammatory markers and other factors that contribute to the development of CCV such as highly sensitive C-reactive protein, glutathione peroxidase, nitric oxide, and vascular endothelial growth factor. Our study cannot clarify the exact mechanism for the relation between NLR and poor collaterals in patients with stable CAD and further studies are needed. There are no data about physical activity and medication of patients that may influence the development of CCC. We evaluate the significance of stenosis by visualizing with objective methods like fractional flow reserve and intravascular ultrasound.
Conclusion
High levels of NLR are associated with the development of CCC in patients with stable CAD. We suggested that NLR, an indicator of inflammatory response, might be used as a biomarker with no additional costs in patients with stable CAD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.