
Abstract
Background:
The use of flow-mediated dilation (FMD) as a surrogate indicator for the extent of coronary artery disease (CAD) remains largely unknown. We assessed FMD at the brachial artery in 89 consecutive patients undergoing coronary angiography.
Methods and Results:
Patients were classified in groups 0 to 3 according to the number of diseased vessels and the SYNTAX score was calculated. The FMD decreased significantly from groups 0 to 3 (P < .001). There was a significant linear relation between SYNTAX score and FMD (corrected r 2 = .64, P < .001). In multivariate analysis, a reduced FMD was the only significant independent predictor of the presence of CAD (odds ratio [OR] 1.78, P = .032) and of CAD severity (OR 1.85, P = .005).
Conclusion:
This study confirms that FMD is reduced in patients with CAD and that such reduction in FMD is related to the extent of the disease. Therefore, FMD at the brachial artery is likely to represent a reliable indicator of CAD burden.
Introduction
A great amount of evidences exists about the association between traditional risk factors for cardiovascular disease and endothelial dysfunction (ED). 1 –5 In addition, ED has a prognostic role when considered a marker of global cardiovascular risk. 6,7
Several techniques can be used to assess ED, from forearm plethysmography to quantitative angiography after administration of endothelium-dependent vasodilators. 8,9 Among these techniques, it has been extensively reported that flow-mediated dilation (FMD) of the brachial artery in response to postischemic reactive hyperemia, assessed with ultrasounds, is impaired in patients with cardiovascular disease risk factors, 10 reflecting both local and systemic ED. 6
Provided the need of a simple tool to physiologically test endothelial function in order to assess cardiovascular risk and response to treatment, FMD of the brachial artery is still considered the most attractive technique because it is noninvasive and allows repeated measures. 4 Yet, the role of FMD of the brachial artery in clinical practice remains to be established. 11
The correlation between impaired FMD and coronary artery disease (CAD) was demonstrated more than a decade ago in patients undergoing coronary angiography 12 and later confirmed in patients with angiographic restenosis after coronary stenting. 13 These associations support the use of FMD as a screening tool to exclude CAD in low-risk patients. 14 The FMD being an operator-dependent index without any consensus about normality range, the routine use of FMD as a surrogate marker for the extent of coronary atherosclerosis still remains largely unknown.
The purpose of this study was to explore the association between FMD measured at the brachial artery with a standardized examination protocol and current indicators 15 of the severity of CAD in a consecutive population undergoing coronary angiography for clinical reasons.
Materials and Methods
Study Population
We enrolled 89 patients consecutively admitted to our department over 3 months and undergoing coronary angiography because of stable ischemic syndrome, valvular heart disease, or cardiomyopathy. All patients consented for participation in the study, and institutional review board approval was obtained.
Coronary risk factors considered are as follows: family history (first-degree relatives with cardiovascular disease); smoking (or previous smoking within the last 5 years); diabetes mellitus (fasting serum glucose levels > 126 mg/dL or therapy with oral hypoglycemic agents or insulin); hyperlipidemia (total serum cholesterol > 220 mg/dL and/or serum triglycerides > 200 mg/dL or therapy with lipid-lowering medications); hypertension (systolic blood pressure > 140 mm Hg or diastolic blood pressure > 90 mm Hg on 2 consecutive seated measurements or therapy with antihypertensive medication).
An arbitrary score, ranging from 0 to 5 points, was built assuming 1 point for each risk factor.
Coronary Angiography
Coronary angiography was performed using a standard Judkins technique. Two expert interventional cardiologists, who were blinded to the clinical data, interpreted all angiograms independently. For the purpose of the analysis presented in what follows, patients were classified in groups 0 to 3 according to the number of diseased vessels (any stenosis >70% and >50% on the left main stem by visual estimation was considered significant); the SYNTAX score, an angiographic tool grading the complexity of CAD taking into account the number, position, and anatomical characteristics of coronary lesions, 16 was calculated for each patient. Any disagreement in SYNTAX score calculation was resolved by consensus. Finally, 2 different couples of arbitrary dichotomic variables (SYNTAX score = 0 or >0, namely, the absence or presence of CAD, and SYNTAX score ≤ or >22, representing a mild or a moderate to severe CAD 17,18 ) were assumed to further stratify the role of FMD according to the extent of CAD.
Exclusion criteria were severe obesity (body mass index [BMI] > 40 kg/m2) because of the potential cuff/arm mismatch; moderate to severe chronic kidney disease (estimated glomerular filtration rate < 60 mL/min per 1.73 m2 as assessed by the Modification of Diet in Renal Disease formula), as FMD is impaired in these patients 19 ; ongoing treatment with vasoactive drugs, such as nitrates, if they could not be withheld for at least 4 half-lives before the test; and known or newly diagnosed atherosclerotic disease of the upper limbs arteries.
Flow-Mediated Dilation Study
The FMD was studied in a quiet, temperature-controlled (20°C) room 1 day before to 3 days after coronary angiography, early in the morning, in order to minimize physiological fluctuations in endothelial function. Patients fasted for at least 8 hours before the study. An ultrasound system (ATL HDI 5000, Philips Healthcare, Best, The Netherlands) equipped with multiple-frequency (L12-5) vascular transducer and electrocardiogram (ECG) gating was used.
The brachial artery was imaged above the antecubital fossa in the longitudinal plane. A segment with clear anterior and posterior intimal interfaces between the lumen and the vessel wall was selected for continuous 2-dimensional gray-scale imaging.
A sphygmomanometric cuff was first placed on the upper arm and a baseline rest measure of brachial artery intima-to-intima diameter was acquired. Thereafter, the cuff was inflated to 50 mm Hg above systolic pressure to occlude arterial inflow for 3 minutes. Cuff was deflated subsequently and hyperemic brachial artery diameter was measured 60 seconds later.
20
The percentage variation of brachial artery intima-to-intima diameter was recorded, according to the following formula
21
:

Of note, ECG gating during image acquisition was used to measure brachial artery diameter at end diastole 22 which, in turn, was identified by the R-wave onset.
Statistical Analysis
Continuous variables are expressed as mean ± standard deviation and compared with t-test and 1-way analysis of variance (ANOVA), as appropriate; categorical variables are expressed as absolute counts and/or percentages and compared with chi-square test.
The relations between FMD and continuous or categorical variables were explored with linear and logistic regression analysis, respectively. A multivariate analysis was carried out to assess the role of FMD as independent predictor of the presence and severity of CAD in addition to traditional risk indicators (age, gender, BMI, coronary risk factors); the odds ratio (OR) and 95% confidence interval (CI) are presented.
Receiver–operating characteristic (ROC) curve analysis was performed to establish the cutoff values of FMD in patients without CAD and in patients with moderate to severe CAD, with the area under the curve (AUC) as a measurement of accuracy. Sensitivity and specificity were calculated and the cutoff was identified according to the Youden index: ([sensitivity + specificity] − 1).
A P < .05 was always requested for statistical significance. The calculations were performed using SPSS, version 20.
Results
Over the study period, 89 patients (mean age 58 ± 20 years, 65 males) were enrolled. Among them, 71 (80%) patients had an established CAD (SYNTAX score > 0) and underwent subsequent myocardial revascularization either by percutaneous coronary intervention or by coronary artery bypass grafting. In all, 25 (28%) patients had a moderate to severe CAD (SYNTAX score > 22). 17 In 18 (20%) patients, diagnostic coronary angiography did not reveal any disease (SYNTAX score = 0). Of them, 2 had dilated cardiomyopathy, 4 were patients with valvular heart disease referred before cardiac surgery, and 12 patients had undergone coronary angiography because of atypical chest pain and inconclusive noninvasive studies.
In the whole study group FMD was 8.4% ± 7.6% (range −3.4%-25.8%) and decreased significantly from groups 0 to group 3 (1-way ANOVA F =19.19, P < .001; Table 1 and Figure 1): in group 0, FMD was 16.4% ± 4.4%. In groups 1, 2, and 3, respectively, the FMD was 9.4% ± 7.3%, 9.5% ± 9.3%, and 3.9% ± 8.1% (P < .05 in all 3 groups vs group 0).
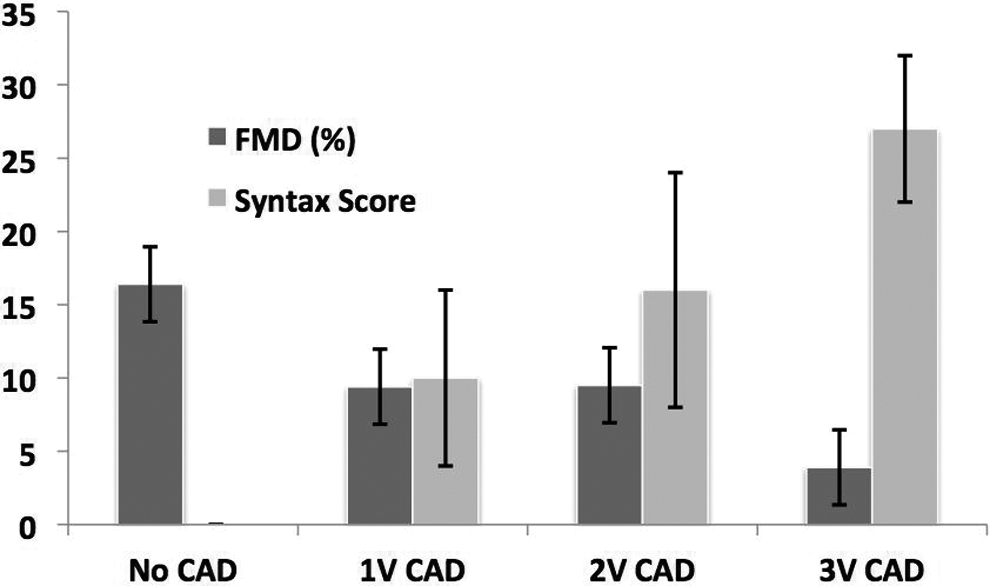
Flow-mediated dilation (FMD) and SYNTAX score (both expresses as mean ± standard deviation) according to coronary artery disease (CAD) status. FMD decreases and SYNTAX score increases according to CAD disease status (analysis of variance [ANOVA] P < .001 in both cases).
Clinical Characteristics of the Population According to CAD Status.a
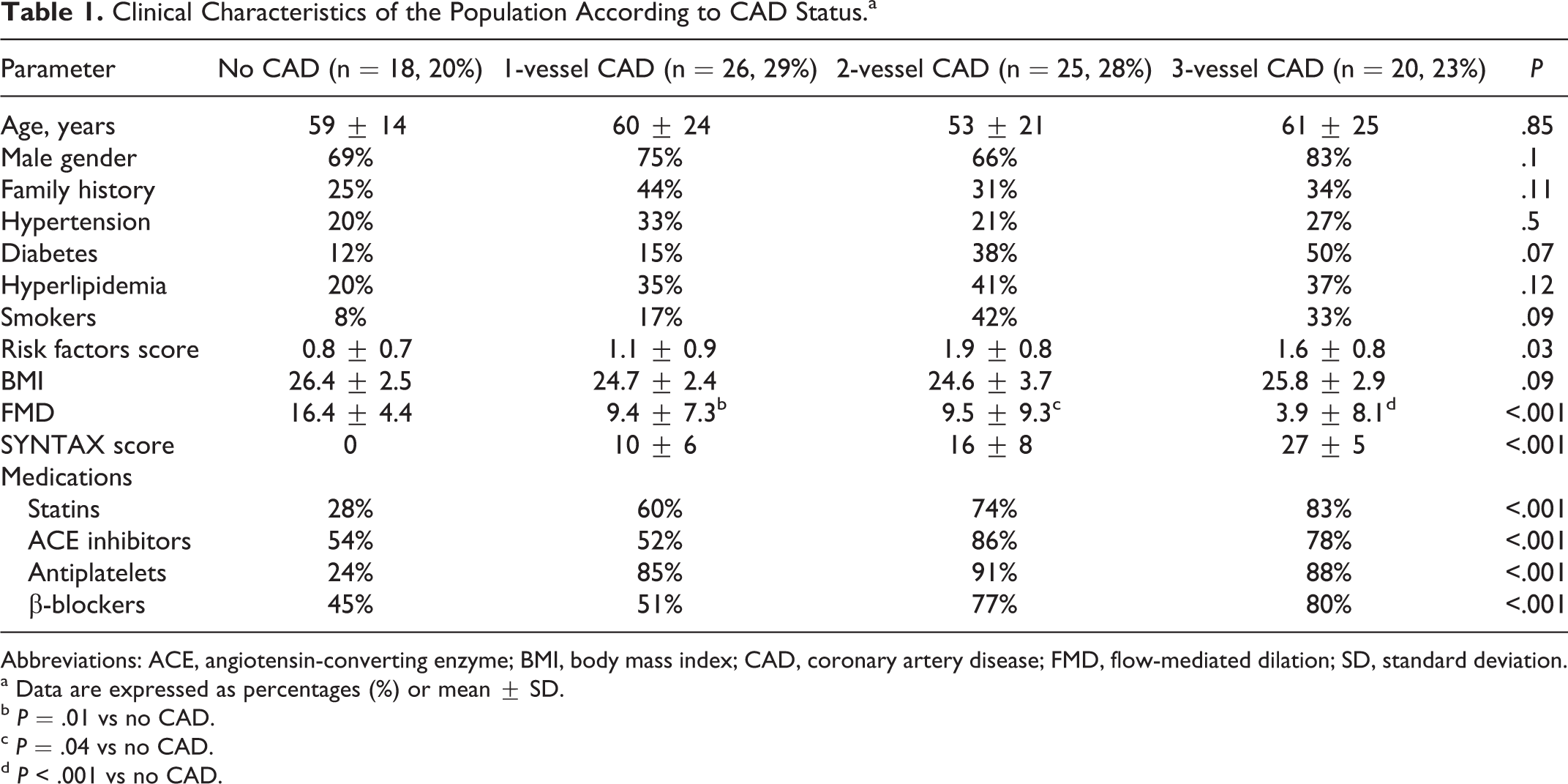
Abbreviations: ACE, angiotensin-converting enzyme; BMI, body mass index; CAD, coronary artery disease; FMD, flow-mediated dilation; SD, standard deviation.
a Data are expressed as percentages (%) or mean ± SD.
b P = .01 vs no CAD.
c P = .04 vs no CAD.
d P < .001 vs no CAD.
There was a significant linear relation between SYNTAX score and FMD (corrected r2 = 64, P < .001; Figure 2). Accordingly, reduced FMD was associated with the presence of CAD (SYNTAX score > 0) at logistic regression analysis (OR 1.61, 95% CI 1.17-2.21, P = .003) and, with ROC analysis, a cutoff FMD >12% had 89% sensitivity and 83% specificity (AUC 0.94, P < .001) to rule out CAD.
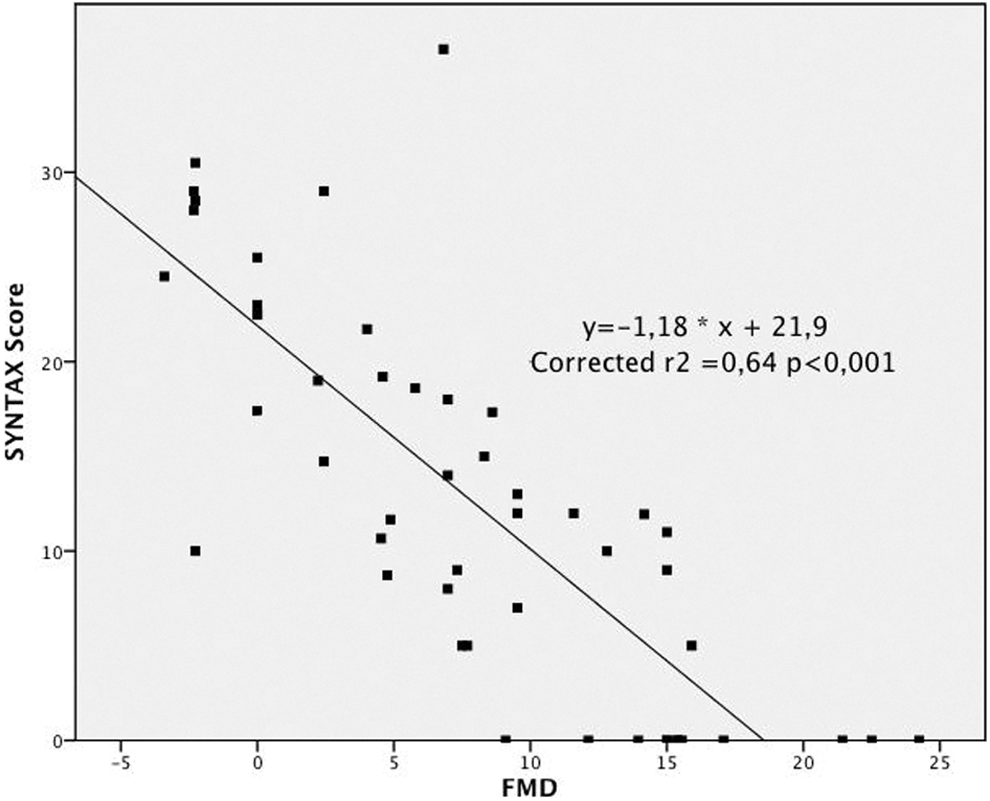
Relation between flow-mediated dilation (FMD) and SYNTAX score. A linear relation exists between FMD (%) assessed at the brachial artery and coronary artery disease (CAD) evaluated by SYNTAX score (P < .001).
In addition, reduced FMD was related even to the presence of a moderate to severe (SYNTAX score > 22) CAD (OR 1.65, 95% CI 1.20-2.27, P = .002) and in this subset of patients FMD was virtually abolished (−0.3% ± 2.9% vs 11.8% ± 6.0%, P < .001). With ROC analysis, a cutoff FMD <4% had a 91% sensitivity and 89% specificity (AUC 0.97, P < . 001) to identify moderate to severe CAD.
Finally, at multivariate logistic regression analysis a reduced FMD was the only significant independent predictor of the presence (SYNTAX score > 0) of CAD (OR 1.78, 95% CI 1.05-3.00, P = .032) and of CAD severity (SYNTAX score > 22, OR 1.85, 95% CI 1.21-2.83, P = .005).
Discussion
Evidence suggests that ED is on the causal pathway for both atherogenesis and destabilization of established plaques. Alterations in endothelial function precede the development of morphological changes and contribute to atherosclerotic lesion progression. Endothelial function assessed by FMD has been shown to be affected by cardiovascular risk factors, to be related to structural arterial disease, and to predict cardiovascular outcome, validating its use for studying the pathophysiology of arterial disease. 5 Numerous studies have also demonstrated that it is responsive to physiological and pharmacological interventions. Although a relationship between endothelial-dependent vasodilatation in the brachial and the coronary circulation exists, 23 it may not be roughly translated into a close relationship between the degree of FMD and the whole spectrum of CAD. 12,14
The main result of this study is that FMD, as assessed with ultrasounds at the brachial artery, is reduced whenever CAD is present; in other words, it confirms that systemic endothelial function reflects the propensity of arteries to develop atherosclerotic lesions 5 and ED has to be present before atherosclerotic changes in the arterial wall begin to develop. Indeed, in a large longitudinal study, impaired FMD at the brachial artery was associated with increased carotid intima–media thickness. 24 Therefore, ED is an early event in atherosclerosis and the status of systemic endothelial function may modify the association between risk factors and atherosclerosis since endothelial function is not solely affected by the individual risk factor burden. 24
A second confirmatory result is that a relation exists between the extent of the ED, expressed by FMD, and the severity of CAD, as assessed both as number of diseased vessel and as disease complexity, whenever angiographic lesion characteristics and location are considered in addition. 17 This observation adds further to the established notion that blunted systemic endothelial vascular reactivity represents an independent predictor of increased coronary risk: common underlying mechanisms are likely to account for ED at the peripheral and coronary level, highlighting the systemic nature of this phenomenon. 25
In patients with severe CAD, FMD was virtually abolished and in some cases a posttest reduction in brachial artery diameter was observed. This phenomenon likely represents the paradoxical response of the diseased endothelium to shear stress. Accordingly, it is established that in coronary circulation, whenever ED is present, vasodilator stimuli can act as vasoconstrictors 26 and that such abnormal response is associated with cardiovascular events. 27
A third point deserving to be highlighted is that FMD remained the only independent predictor of the presence and severity of CAD at multivariate regression analysis in this moderate-risk population, with a high prevalence of CAD. The interest in the use of imaging studies for subclinical atherosclerosis, on top of conventional risk factor assessment, lies in potential improvement in risk prediction for the occurrence of cardiovascular events. 28 To this purpose, erectile dysfunction is a common situation for patients with cardiovascular risk factors in which impaired endothelium-dependent vasodilation plays a central role and in which unmasking subclinical CAD might have prognostic implications. 29 Noteworthy, it had been yet reported that the added predictive value of additional screening was primarily found in asymptomatic individuals at low cardiovascular risk. 30 In addition, besides technical challenges and the need for a learning curve, 4 FMD of the brachial artery is historically limited by the lack of a range of normality. Actually, a large overlap has been reported among different populations. 31 The standardization of FMD measurement will facilitate studies in large patient populations and comparison of data from different laboratories. 32 In our study, FMD >12% was associated with the absence of CAD whereas FMD was <4% in almost all patients with severe CAD. These values, derived from a real-world population of patients with risk factors undergoing coronary angiography, need confirmation in larger populations but do not differ substantially from those previously reported. 14
Although FMD is still considered the gold standard technique for noninvasive measurement of endothelial function, it requires specialized training and high-resolution sonography equipment, which may not always be available for clinical use. Pulse Amplitude Tonometry, a recently Food and Drug Administration-approved method which is relatively inexpensive and operator independent, is increasingly being used as a reliable measure of endothelium-dependent dilation in response to reactive hyperemia. 32 None of the currently available methods for measuring endothelium-dependent dilatation satisfies all the criteria for clinical assessment of individual risk. 33 Yet, the measurement of endothelial function, whichever the testing modality, is a marker of arterial health which contains substantial prognostic information.5,6
Study Limitations
Our study enrolled a small cohort of patients undergoing coronary angiography based on a clinical indication in a single-center, real-world setting. Therefore, our observations cannot be generalized to the general population also because we have not yet applied our ROC-derived cutoff to a new validation data set. Nevertheless, the results of the present study demonstrate that the introduction of endothelial function evaluation may add a piece of information on top of that provided by the “standard” risk factors, at least in individuals with a high prevalence of CAD. Additional research in asymptomatic individuals with low to intermediate risk of CAD is needed to quantify the cost-effectiveness and impact of imaging for subclinical atherosclerosis on cardiovascular risk factor management and patient outcomes. 11
The possible confounding effect of cardiovascular medications and their interaction with risk factors also needs to be acknowledged. Although these medications may have impacted the results, the large use of antiplatelet agents, statins, and angiotensin-converting enzyme inhibitors in our patients with CAD may likely have reduced the differences across groups, possibly underestimating the role of FMD. Further, response to nitroglycerin, an endothelium-independent vasodilator, was not tested. Despite the above-mentioned limitations, our data show that endothelial function measures provide information on the presence and extent of CAD also in clinical settings. Therefore, assessment of FMD might facilitate the interpretation of the cardiovascular risk at an individual level.
Finally, we have used the SYNTAX score, among others, to quantify the extent of CAD. The SYNTAX score was developed to express the procedural complexity of coronary revascularization, 16 rather than of CAD burden, and its value to the purpose of this study may be questioned. Nonetheless, it has been demonstrated 33 that commonly used angiographic scoring systems are strongly correlated both with each other and with intravascular ultrasound-derived measures of atherosclerotic plaque burden, even in the absence of significant luminal stenosis. Therefore, it is likely that any angiographic scoring system may be used to provide meaningful assessment of CAD burden for use in both clinical practice and in research.
Conclusions
This study confirms that FMD is reduced in patients with CAD and that such reduction in FMD is related to the extent of disease. The relationship between FMD and CAD disease is evident evaluating CAD both qualitatively and by means of the SYNTAX score. Therefore, assuming FMD as an indicator of global endothelial function, FMD at the brachial artery is likely to represent a reliable indicator of the burden of atherosclerotic disease in the coronary arteries and possibly in the entire vascular system.
We will further investigate whether the use of additional hemodynamic parameters, namely, indices of resistance and flow recovery time, known as being less operator dependent, may better predict the extent of CAD when added to brachial artery diameter variations in FMD studies.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.