
Abstract
Objectives:
We aimed to investigate the relationship between the platelet-lymphocyte ratio (PLR) and coronary collateral circulation (CCC) in patients with stable angina pectoris (SAP) and chronic total occlusion (CTO).
Methods:
A total of 294 patients with both SAP and CTO were classified according to their Rentrop collateral grades as either poor (Rentrop grades/0-1) or good (Rentrop grades/2-3).
Results:
The PLR values were significantly higher in patients with poor CCC than in those with good CCC (156.8 + 30.7 vs 132.1 + 24.4, P < 0.001). In regression analysis, PLR (unit = 10) [odds ratio 1.48, 95% confidence interval (CI) 1.33 -1.65; P < 0.001] and high-sensitivity C-reactive protein were found to be the independent predictors of poor CCC. In receiver operator characteristic curve analysis, optimal cut-off value of PLR to predict poor CCC was found as 138.1, with 76% sensitivity and 65% specificity.
Conclusion:
PLR may be an important, simple, and cost effective tool predicting the degree of collateralization in patients with SAP and CTO.
Introduction
The coronary collateral circulation (CCC) has been shown to determine the survival of the myocardium upon total occlusion of the coronary arteries. 1 –3 Recently, a meta-analysis by Meier et al 4 demonstrated that patients with high degree of collateralization have a 36% lower risk of mortality than those with low degree of collateralization. However, the heterogeneity in the degree of collateralization among patients with coronary artery disease is poorly understood. 5 Inflammation which is a central factor for the initiation and progression of atherosclerosis may be implicated in the variability of the collateralization, because a complex interaction exists between inflammation and new blood vessel formation. 6 Previous studies have proven the association between elevated blood platelet count and major adverse cardiovascular outcomes. 7 –9 In contrast, a low blood lymphocyte count was associated with major adverse cardiovascular outcomes. 10 –12 Interestingly, the platelet–lymphocyte ratio (PLR) was found to be a significant inflammatory marker to predict mortality in cancer population. 13 –15 Moreover, higher PLR value emerged as a significant independent predictor of long-term survival in patients who presented with non-ST-segment elevation myocardial infarction (NSTEMI). 16 Therefore in this study, we aimed to investigate the effect of this recently defined cardiovascular risk marker, PLR, on the collateral development in patients with stable angina pectoris (SAP) and chronic total occlusion (CTO) of a major coronary artery.
Methods
Study Population
The study population consisted of 385 consecutive patients with CTO who underwent coronary angiography at our hospital. All patients had stable anginal symptoms and/or positive stress test results indicating ischemia. Clinical information including age, sex, body mass index (BMI), history of hypertension and diabetes mellitus, smoking, current medications, complete blood count, serum cholesterol, fasting glucose levels, and left ventricular ejection fraction (LVEF) values (that was calculated using a modified Simpson method) was obtained from a review of the patients’ chart. The patients were defined as hypertensive if their blood pressure was ≥140/90 mm Hg or if the individual was taking any antihypertensive medications. Diabetes mellitus was defined as the presence of a history of antidiabetic medication usage or fasting glucose level above 126 mg/dL. Patients with total cholesterol ≥200 mg/dL or triglyceride ≥150 mg/dL were considered to have hyperlipidemia. Current smokers were defined as those who had smoked for some period during the past year. Patients were excluded from the study if they had recent (within 3 months) history of acute coronary syndrome (n = 14), decompensated heart failure (n = 9), a recent history of blood transfusion (n = 4), active and ongoing infection (n = 8), chronic inflammatory or autoimmune disease (n = 4), active cancer or hematological proliferative diseases (n = 2), severe hepatic diseases (n = 2), renal failure (n = 5), and history of percutaneous coronary intervention (n = 26) or coronary artery bypass grafting (n = 17). Finally, 294 patients with both SAP and CTO were enrolled into the study. The study protocol was approved by the local ethics committee.
Blood Samples and Analyses
Results of the blood samples and analyses were obtained from the review of the patients’ chart. All blood samples were drawn at admission before coronary angiography. Hematologic indices such as hemoglobin, white blood cell, platelet counts, and mean platelet volume were measured as part of the automated complete blood count using simultaneous optical and impedance measurements (Cell Dyn 3700 Abbott Diagnostics, IL, USA). All routine biochemical tests were carried out on an automatic biochemical analyzer (Beckman Coulter AU640, Germany). High-sensitivity C-reactive protein (hs-CRP) was determined by nephelometry on an IMMAGE 800 analyzer (Beckman Coulter, CA, USA).
Coronary Angiography and Assessment of CCC
Two specialists, who were blinded to the clinic and laboratory results of the patients, read the coronary arteriographic data of each patient to assess the coronary artery lesion and CCC. Chronic total occlusion was defined as a lesion with a thrombolysis in myocardial infarction grade 0 flow within the occluded segment and angiographic or clinical evidence or high likelihood of occlusion duration ≥3 months. 17 The CCC was graded according to the Rentrop classification. 18 Grades of collateral filling from the contralateral vessel were as follows: 0 = none; 1 = filling of side branches of the artery to be dilated through collateral channels without visualization of the epicardial segment; 2 = partial filling of the epicardial segment through collateral channels; and 3 = complete filling of the epicardial segment of the artery being dilated through collateral channels. In patients with more than one collateral vessel supplying the distal region of the diseased artery, the highest collateral grade was recorded. Patients were then classified according to their collateral grades as either poor (Rentrop grades 0-1) or good (Rentrop grades 2-3). Definition of the number of coronary vessels diseased included stenosis of ≥50% of the major epicardial arteries or their main branches or both. Intra- and interobserver agreements of Rentrop collateral grades were determined from a random sample of 50 coronary angiograms (κ values were 0.925 [intraobserver] and 0.815 [interobserver] agreement; P < .001 for both].
Statistical Analysis
Statistical analysis was performed using the SPSS for Windows (version 19.0; SPSS Inc, Chicago, Illinois). Continuous variables are expressed as mean ± standard deviation; categorical variables were defined as percentages. The comparisons between the 2 CCC groups were performed using the chi-square test for categorical variables. The differences between the continuous variables were compared using the Student t test or Mann-Whitney U test where appropriate. Comparison between Rentrop grades was made using the analysis of variance. Multiple logistic regression analysis was performed to identify the independent predictors of poor CCC. Variables showing marginal associations with poor CCC on univariate testing were included in the regression analysis (P < .10). A receiver–operating characteristic (ROC) curve was constructed to determine the predictive value of PLR on poor CCC development. A P value of <.05 was considered statistically significant. Moreover, power analysis and calculations of sample size were performed before the study to detect a 20% difference in PLR values between poor and well-developed CCC, 245 patients were required to achieve power of 80% with a P value of <.05.
Results
A total of 294 patients (mean age 59.9 ± 9.7 years, 244 men) with both SAP and CTO were included in the study. In the study group, 163 of the 294 patients were found to have poorly developed CCC. Comparisons of the clinical, laboratory, and angiographic characteristics of the patients according to the collateral development are shown in Tables 1 and 2. Both the groups were similar in terms of age, gender, BMI, or LVEF. Furthermore, there was no significant difference in the cardiovascular risk profiles of the 2 subgroups, such as the presence of diabetes mellitus, hypertensive disease, smoking, or hypercholesterolemia. Compared to the patients with well-developed CCC (Rentrop grades 2 and 3), patients with poorly developed CCC (Rentrop grades 0 and 1) exhibited higher hs-CRP, platelet count, and mean platelet volume whereas lower value of absolute lymphocyte count (Table 1). Compared to the patients with well-developed CCC, patients with poorly developed CCC had significantly higher PLR values (156.8 ± 30.7 vs 132.1 ± 24.4, P < .001). Beyond this, an inverse stepwise association was present between collateral score and mean PLR values (Figure 1). The PLR values decreased with increasing Rentrop grade, with a mean PLR value of 165.6 ± 32.1, 153.7 ± 29.2, 136.5 ± 23.9, and 125.7 ± 22.6 in patients with Rentrop grades of 0, 1, 2, and 3, respectively (P for trend <.001). Also, correlation analysis showed an inverse association between hs-CRP and Rentrop score (r= −.376, P < .001) and a significant positive correlation between hs-CRP and PLR (r = .412, P < .001). Moreover, PLR (unit = 10; odds ratio [OR] 1.48, 95% confidence interval [CI] 1.33-1.65; P < .001) and hs-CRP (OR 1.58, 95% CI 1.07-2.32; P = .001) were found as independent predictors of poor CCC in multivariate logistic regression analysis (Table 3). The ROC analysis yielded a cutoff value of 138.1 for PLR to predict insufficient CCC with 76% sensitivity and 65% specificity, with the area under the ROC curve being 0.771 (95% CI 0.718-0.814, Figure 2).
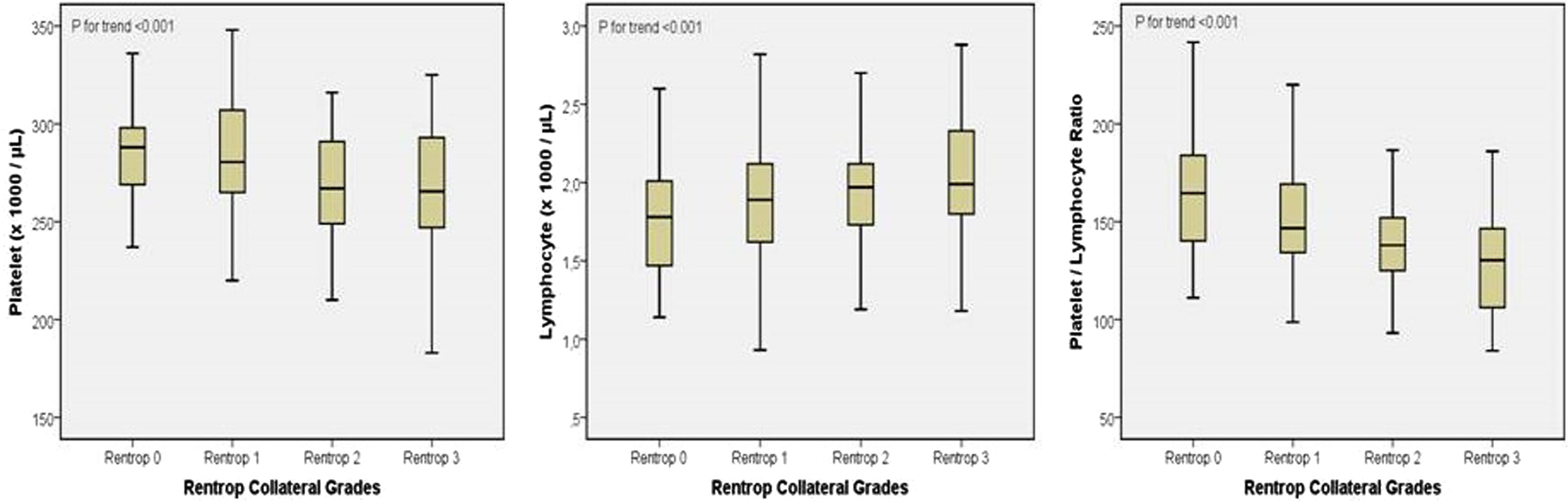
Platelet, lymphocyte, and platelet–lymphocyte ratio according to Rentrop collateral grades.
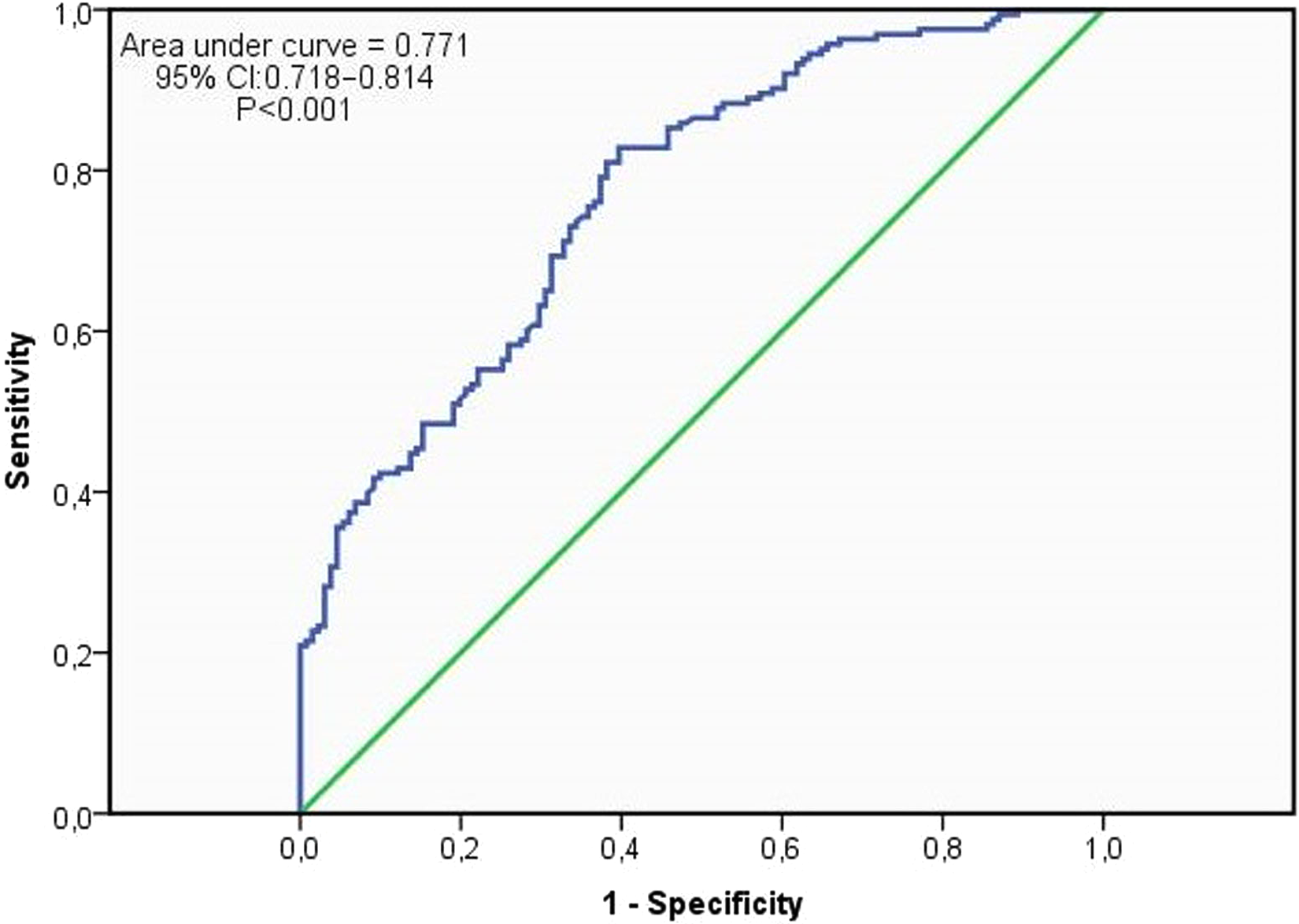
Receiver–operating characteristic curves for platelet–lymphocyte ratio in prediction of poorly developed coronary collateral circulation with high sensitivity and specificity. CI indicates confidence interval.
Comparison of the Clinical and Laboratory Properties of Patients With Poorly Developed and Well-Developed Coronary Collateral Circulation.a
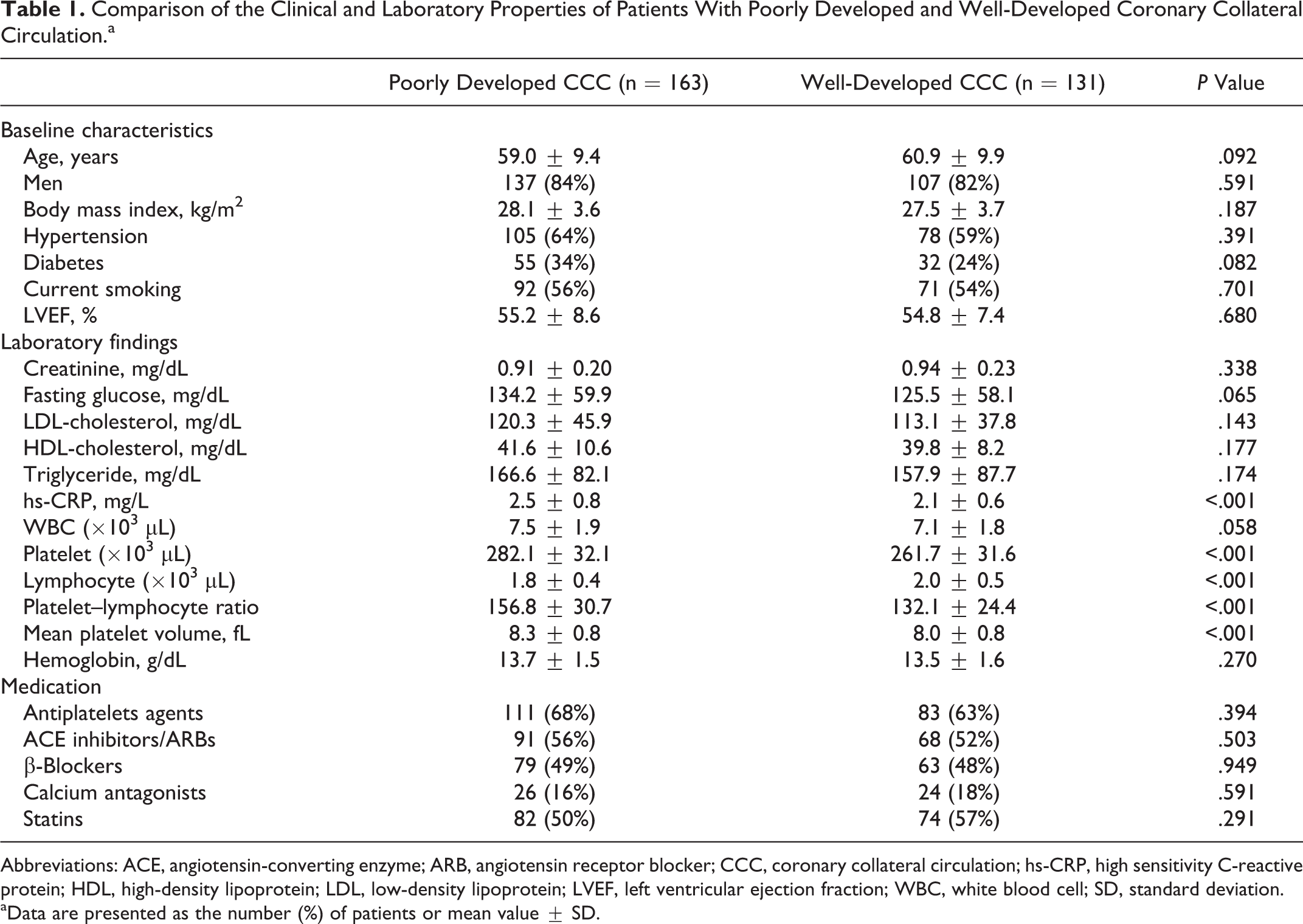
Abbreviations: ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; CCC, coronary collateral circulation; hs-CRP, high sensitivity C-reactive protein; HDL, high-density lipoprotein; LDL, low-density lipoprotein; LVEF, left ventricular ejection fraction; WBC, white blood cell; SD, standard deviation.
aData are presented as the number (%) of patients or mean value ± SD.
Coronary Angiographic Features of the Study Population.a
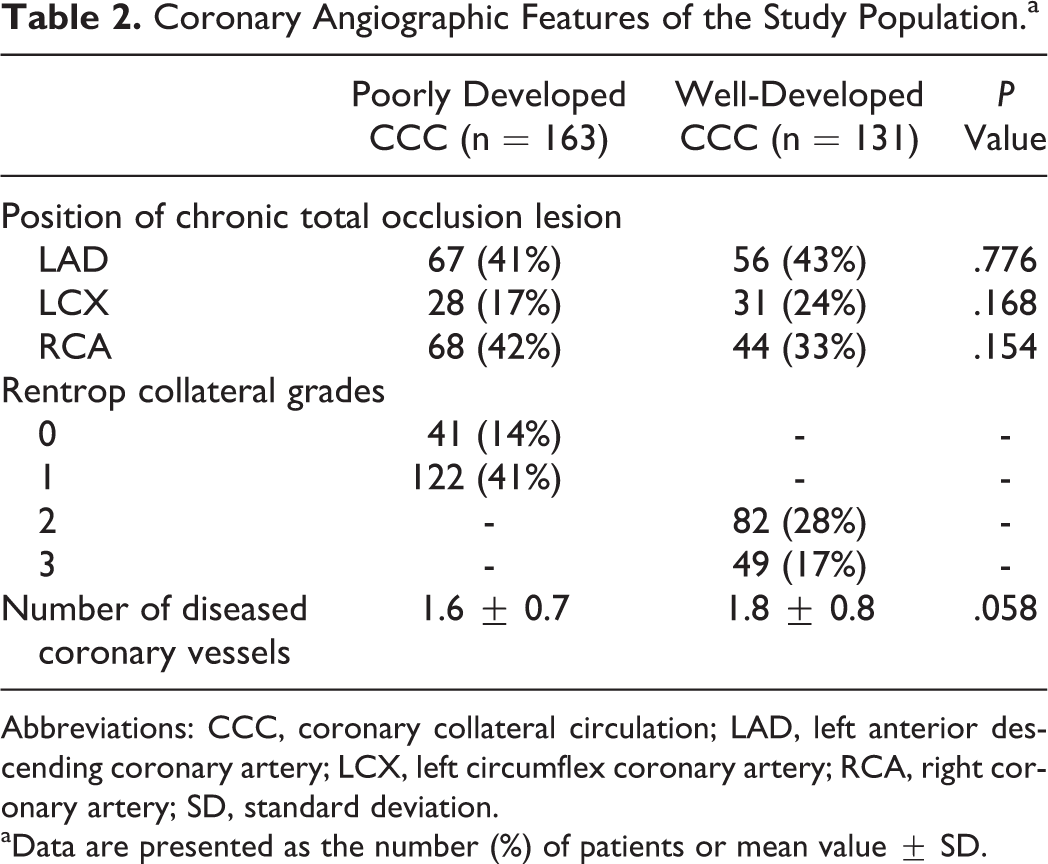
Abbreviations: CCC, coronary collateral circulation; LAD, left anterior descending coronary artery; LCX, left circumflex coronary artery; RCA, right coronary artery; SD, standard deviation.
aData are presented as the number (%) of patients or mean value ± SD.
Univariate and Multivariate Analyses of Poorly Developed Coronary Collateral Circulation.a
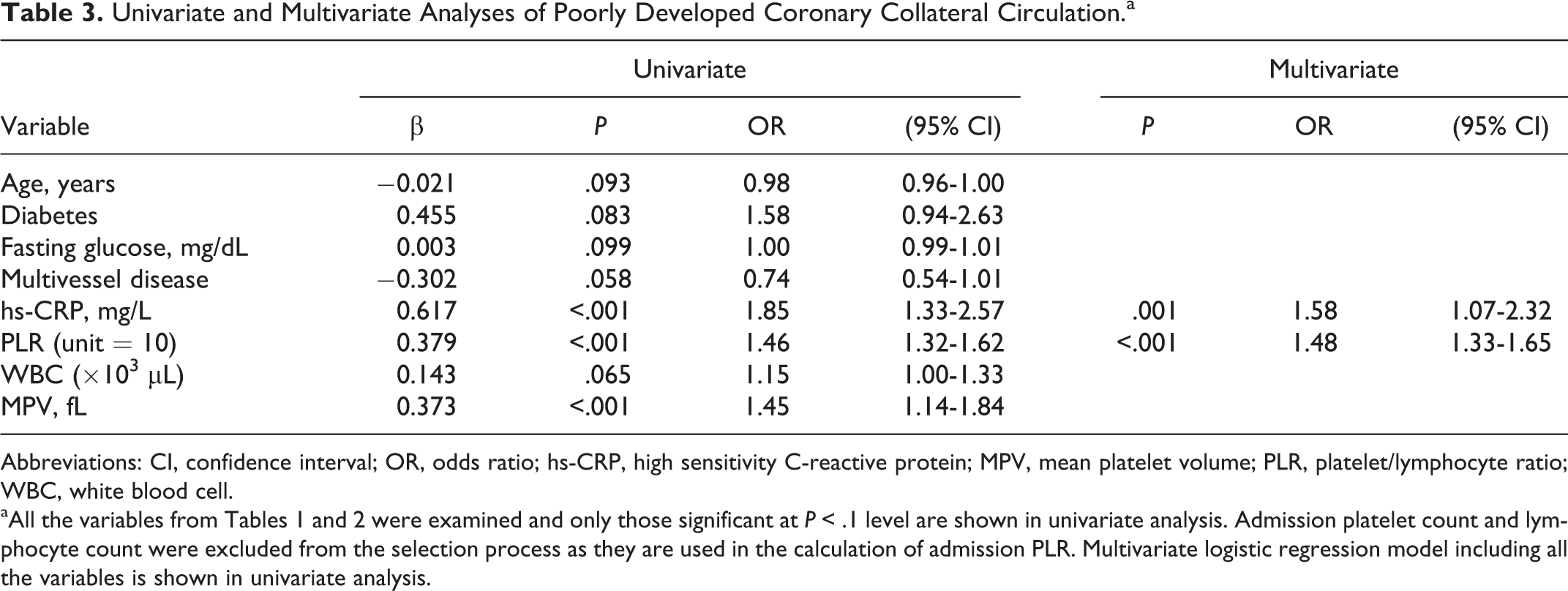
Abbreviations: CI, confidence interval; OR, odds ratio; hs-CRP, high sensitivity C-reactive protein; MPV, mean platelet volume; PLR, platelet/lymphocyte ratio; WBC, white blood cell.
aAll the variables from Tables 1 and 2 were examined and only those significant at P < .1 level are shown in univariate analysis. Admission platelet count and lymphocyte count were excluded from the selection process as they are used in the calculation of admission PLR. Multivariate logistic regression model including all the variables is shown in univariate analysis.
Stratified Subgroup Analyses
Since low lymphocyte and high platelet counts were significantly associated with a poorly developed CCC in the univariate analysis, we decided to perform a stratified analysis to investigate the superiority of PLR to individual platelet or lymphocyte count in predicting poor CCC. We compared the highest tertile of PLR (PLR > 153) with the 2 lower tertiles (PLR ≤ 153). In the subgroup with lymphocyte count ≥1.5 × 103/µL, there was a significant higher rate of poor CCC among the patients with PLR >153 (31/45 = 69%) compared to those with PLR ≤153 (77/179 = 43%), P = .002. In the subgroup of lymphocyte count <1.5 × 103/µL, the patients with PLR >153 still had a higher rate of poor CCC than patients with PLR ≤153 (85% vs 59%, P = .023). In the subgroup with a platelet count of <300 × 103/µL (n = 227), patients with PLR >153 had significantly higher rate of poor CCC compared to patients with PLR ≤153 (76% vs 42%, P < .001). This effect persisted in the subgroup of platelet count ≥300 × 103/µL (n = 67), with poor CCC 81% in highest PLR tertile versus 57% in the lower 2 tertiles (P = .029). Moreover, we evaluated the association between the highest tertile of PLR (PLR > 153 vs PLR ≤153) and received antiplatelet therapy in predicting poor CCC. The rate of poor CCC was not statistically significant between patients who received antiplatelet therapy and those without antiplatelets in the subgroups with PLR >153 and PLR ≤153 (75% vs 86%, P = .261 and 46% vs 42%, P = .634, respectively).
Discussion
Our findings indicated that a poorly developed CCC might only be predicted by high levels of PLR and hs-CRP. We also showed that the effect of PLR on coronary collateral development was independent of platelet or lymphocyte counts alone.
The functional relevance of collateral vessels in humans has been a matter of debate for many years. 19 There have been numerous investigations demonstrating a protective role of well-grown versus poorly grown collateral arteries showing smaller infarcts, 20 less ventricular aneurysm formation, improved ventricular function, 20 fewer future cardiovascular events, 21 and improved survival. 22 However, there have been conflicting reports regarding this postulated link and observed clinical outcomes. 23 –25 Similarly, we observed no differences in the LVEF according to the collateral development.
The degree of coronary artery stenoses is consistently described as positively determining the extent of coronary collateral formation. 26 We chose patients with CTO for this study so that all would have the same degree of stenoses (100%). Consequently, the effect of severity of coronary artery stenosis on collateral formation did not interfere with the results of our study. However, the development of CCC varies much among patients even with the same degree of stenosis, suggesting the contribution of other determinants in the formation of CCC. In the present study, univariate analysis showed that higher platelet count and mean platelet volume and lower value of absolute lymphocyte count were significantly associated with poorly developed CCC (Table 1).
Platelets regulate new blood vessel growth during wound healing, tumor growth, and in response to ischemia, because they contain a number of angiogenesis promoters and inhibitors. 27 Among the angiogenesis promoters found in platelets are vascular endothelial growth factor, platelet-derived growth factor, basic fibroblastic growth factor, and epidermal growth factor. 27 Furthermore, platelets contain matrix metalloproteinases that are also known to promote angiogenesis. A number of angiogenesis inhibitors are also found in platelets. Among these, angiostatin is especially important in the coronary collateral development. It has been recently reported that angiostatin plays a role in mediating the reduced coronary angiogenesis in the context of inhibition of nitric oxide synthesis, 28 and also angiostatin levels in pericardial fluid are negatively associated with collateral formation in patients undergoing coronary bypass surgery. 29 Nevertheless, thrombocytosis is commonly associated with a coronary arterial disease and has been widely reported as an adverse prognostic marker. 7 –9 It is reported that patients with pathologically increased platelet counts have an enhanced risk of thrombotic complications. 30 Furthermore platelets both initiate atherogenesis and trigger its complications. 7 Therefore, higher platelet count may play a role in both the development and the consequences of cardiovascular disease. In addition to the role in the pathogenesis of atherosclerosis, inflammation was also shown to inhibit the collateral formation mainly by affecting the endothelial function. 31 Moreover, low-grade inflammation may increase circulating platelet count 32 and mean platelet volume levels, 33 which reflect underlying inflammation, as several inflammatory mediators stimulate megakaryocytic proliferation and produce relative thrombocytosis. Therefore in this study, we have hypothesized that, although not directly but may be as a result of the inflammatory process in the atherosclerosis, higher platelet count, and larger platelets, thrombopoiesis may be related to the insufficient CCC. Also, previous reports have stated that lymphopenia is associated with the progression of atherosclerosis. Lymphocyte apoptosis in atherosclerotic lesions may result in lymphopenia, which gradually increases with atherosclerotic burden. Likewise, a low peripheral blood lymphocyte count has also been associated with poorer prognosis. 10 –12 Eventually, both thrombocytosis and lymphocytopenia correlate with the degree of systemic inflammation, and the PLR represents a novel marker incorporating both the hematologic indices.
However, to date no study has been performed on the relationship between PLR and development of CCC. In the present study, we demonstrated that an inverse stepwise association between collateral grade and mean PLR values. Also, there was a significant positive correlation between hs-CRP and PLR. And importantly, they were independent predictors of poor CCC in multivariate logistic regression analysis. These findings are in line with previous reports emphasizing the relation between inflammation and development of coronary collaterals. 34 –36 Since there was no significant difference in the cardiovascular risk profiles (eg, diabetes and blood cholesterol levels) between the 2 subgroups, the present study may suggest that the subclinical inflammation rather than other metabolic factors may be the dominant characteristic leading to poor collateral development. In the subgroup analysis, we showed that the effect of PLR on coronary collateral development was independent of platelet or lymphocyte counts alone. The superiority of PLR to either individual lymphocyte or platelet counts can be explained by the PLR which represents a novel marker incorporating 2 inversely related predictors and immune pathways and may also have higher stability compared to the individual platelet or lymphocyte counts, which could be altered by many physiological and pathological conditions.
Our study has some limitations. First, the cross-sectional design of our study makes it difficult to comment on the causal relationship of PLR and poorly developed CCC. Also, the qualitative evaluation of collaterals with Rentrop may underestimate the collateral formations; however, a recent study 3 reported a good correlation between angiographic and functional methods for the assessment of collaterals in patients with SAP. Being a retrospective study, spot laboratory parameters rather than follow-up values are also among limitations of our study.
In conclusion, for the first time in the literature, we showed the relationship between the PLR and coronary collateral development. We have demonstrated that PLR with an optimal cutoff value of 138.1 predicts insufficient CCC with a sensitivity of 76% and a specificity of 65%. The PLR may be an important, simple, and cost-effective tool predicting the degree of coronary collateralization in patients with SAP and CTO.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.