
Abstract
There is considerable uncertainty related to the thromboembolic risk after laparoscopic cholecystectomy. Patients with pulmonary embolism (PE), deep venous thrombosis (DVT), or venous thromboembolism (VTE) at hospital discharge following laparoscopic cholecystectomy were identified from the Nationwide Inpatient Sample. From 1998 through 2009, 4 107 430 laparoscopic cholecystectomies were performed. The in-hospital prevalence of PE was 0.15%, DVT was 0.40%, and VTE was 0.53%. The prevalence of PE increased from 0.04% in patients aged 21 to 30 years to 0.31% in patients aged 71 to 80 years. Deaths due to in-hospital PE were 780 (0.02%) of the 4 107 430 laparoscopic cholecystectomies. The rate of death increased with age. The prevalence of VTE following laparoscopic cholecystectomy is low and fatal PE is rare. The risk of VTE increased with age, as did the risk of death in those who had PE. These data may be useful in assessing the use of thromboprophylaxis in patients undergoing laparoscopic cholecystectomy.
Introduction
There is considerable uncertainty related to the thromboembolic risk after laparoscopic procedures. 1 The American College of Chest Physicians in 2004 and 2008 recommended against the use of routine thromboprophylaxis for patients undergoing entirely laparoscopic procedures who do not have additional thromboembolic risk factors, other than early and frequent ambulation. 1,2 The American College of Chest Physicians in 2012 described laparoscopic cholecystectomy as “a relatively low-risk procedure.” 3 For patients at “very low risk” of venous thromboembolism (VTE) undergoing general and abdominal–pelvic surgery, no specific pharmacologic or mechanical prophylaxis was recommended other than early ambulation. 3 For patients at “low risk” of VTE, mechanical prophylaxis, preferably with intermittent pneumatic compression, was recommended. 3 The European Association for Endoscopic Surgery recommended intraoperative intermittent pneumatic compression for prolonged laparoscopic procedures. 4 The Society of American Gastrointestinal Endoscopic Surgeons in 2007 recommended patient-specific prophylaxis depending on the number of risk factors. 5 Recommended prophylaxis ranged from none to intermittent pneumatic compression or pharmacologic prophylaxis. 5
In view of uncertainty related to thromboembolic risk, we assessed the database of the Nationwide Inpatient Sample (NIS) to obtain an estimate of the prevalence of in-hospital deep venous thrombosis (DVT), pulmonary embolism (PE), and VTE (PE and/or DVT) following laparoscopic cholecystectomy.
Materials and Methods
From 1998 through 2009, patients with PE, DVT, or VTE following laparoscopic cholecystectomy at discharge from short stay hospitals were identified from the NIS, Healthcare Cost and Utilization Project, and Agency for Healthcare Research and Quality throughout the United States. 6 The NIS contains data of 5 to 8 million hospital stays from about 1000 hospitals and is designed to approximate a 20% sample of US nonfederal, short-term hospitals. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes were used to identify patients (Table 1).
The. ICD-9-CM Codes Used.
Abbreviation: ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification.
Statistical Methods
Linear regression analyses were used to calculate slopes of the curves using InStat version 3.0 (Graph Pad software, San Diego, California). The 95% confidence intervals were also calculated using GraphPad Software.
Results
From 1998 through 2009, 4 107 430 laparoscopic cholecystectomies were performed in short-term nonfederal hospital in the United States. The number of laparoscopic cholecystectomies increased from 302 770 in 1998 to 373 940 in 2009 (Figure 1).
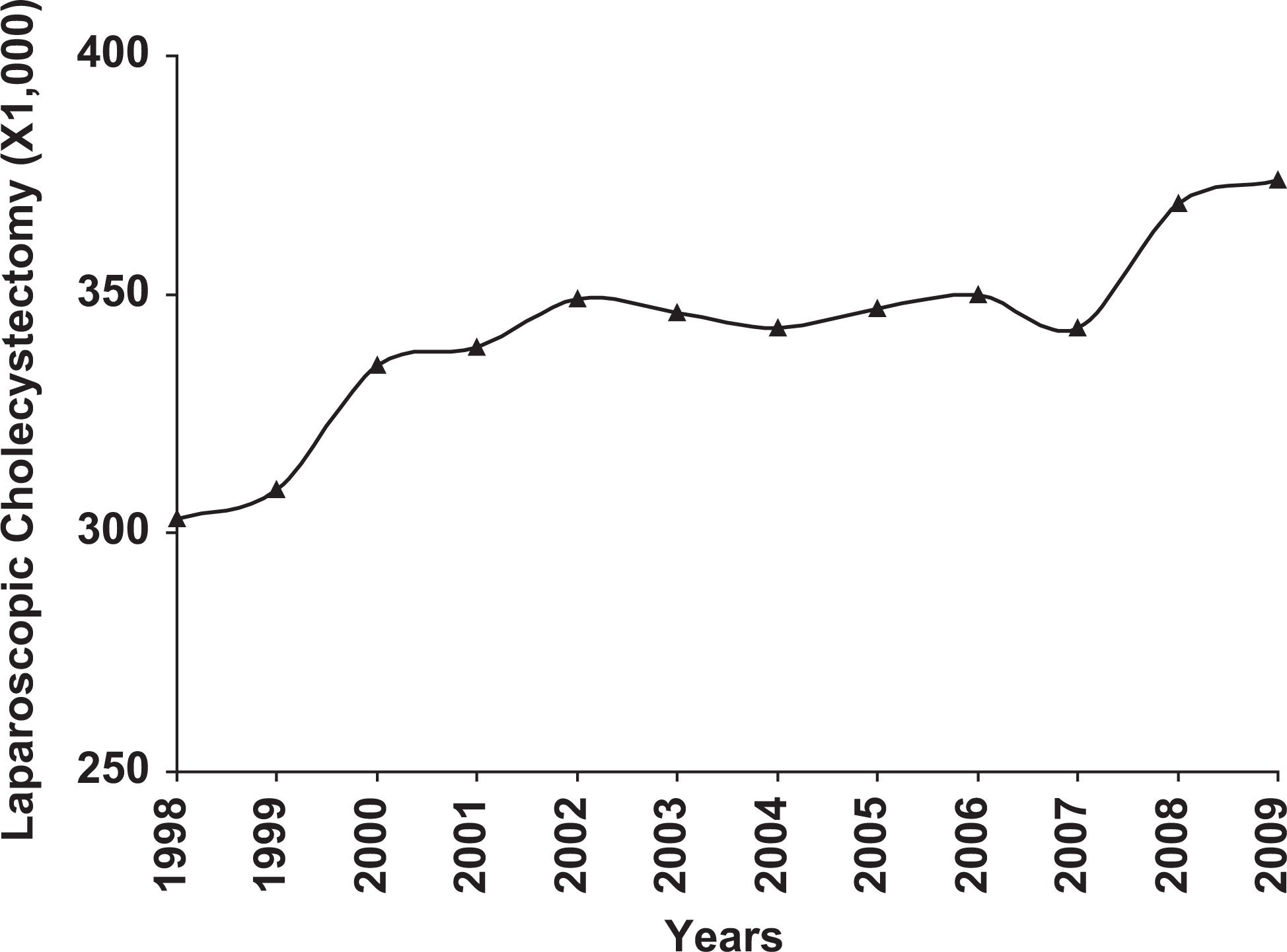
Number of laparoscopic cholecystectomies performed in short hospital stays, in the United States, from 1998 through 2009. The number of procedures increased from 302 770 in 1998 to 373 940 in 2009.
Most (68%) of the patients were white. Females comprised 70%. Age was 52 ± 20 years (mean ± standard deviation [SD]). Length of stay in 95% of patients was 6 ± 4 days (mean ± SD; median = 6, range 1-11 days).
The prevalence of in-hospital PE was 5960 (0.15%) of 4 107 430 and that of DVT was 16 610 (0.40%) of 4 107 430. The prevalence of VTE (PE and/or DVT) was 21 630 (0.53%; Table 2). The incidence of PE, DVT, and VTE increased from 1998 to 2006 (Figure 2). Both DVT and VTE showed the most prominent increase.
In-Hospital PE, DVT, and VTE Following Laparoscopic Cholecystectomy.a
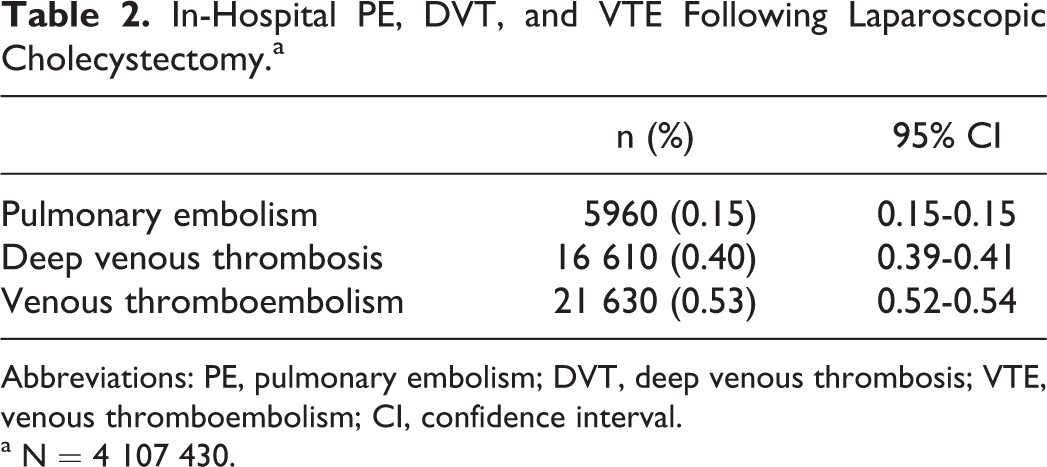
Abbreviations: PE, pulmonary embolism; DVT, deep venous thrombosis; VTE, venous thromboembolism; CI, confidence interval.
a N = 4 107 430.
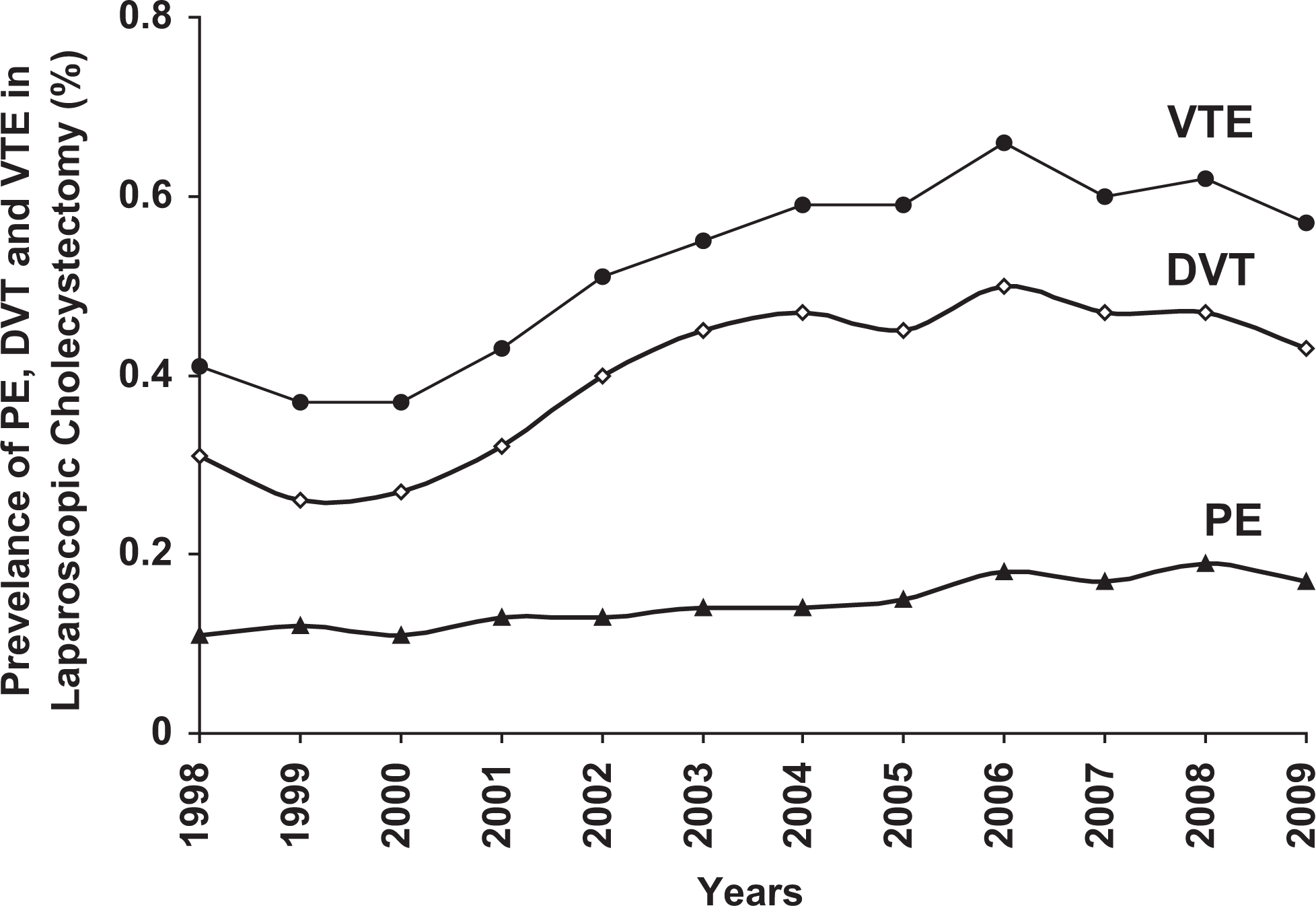
Prevalence of pulmonary embolism (PE), deep venous thrombosis (DVT), and venous thromboembolism (VTE) following laparoscopic cholecystectomy from 1998 through 2009. From 1998 through 2006, DVT increased at a greater rate than PE (0.031 DVT/year vs 0.007 PE/year). PE: r = .9188, P = .0005. DVT: r = .9230, P = .0004. VTE: r = .9493, P = .0001. After 2006, the prevalence of PE and VTE did not change significantly, and DVT tended to decrease (P = .0561).
The prevalence of PE, DVT, and VTE was age related (Figure 3). The prevalence of PE increased from 0.04% in patients aged 21 to 30 years to 0.31% in patients aged 71 to 80 years. The prevalence of DVT increased from 0.13% in patients aged 21 to 30 years to 0.66% in patients aged 71 to 80 years. The prevalence of VTE increased from 0.17% in patients aged 21 to 30 years to 0.90% in patients aged 71 to 80 years.
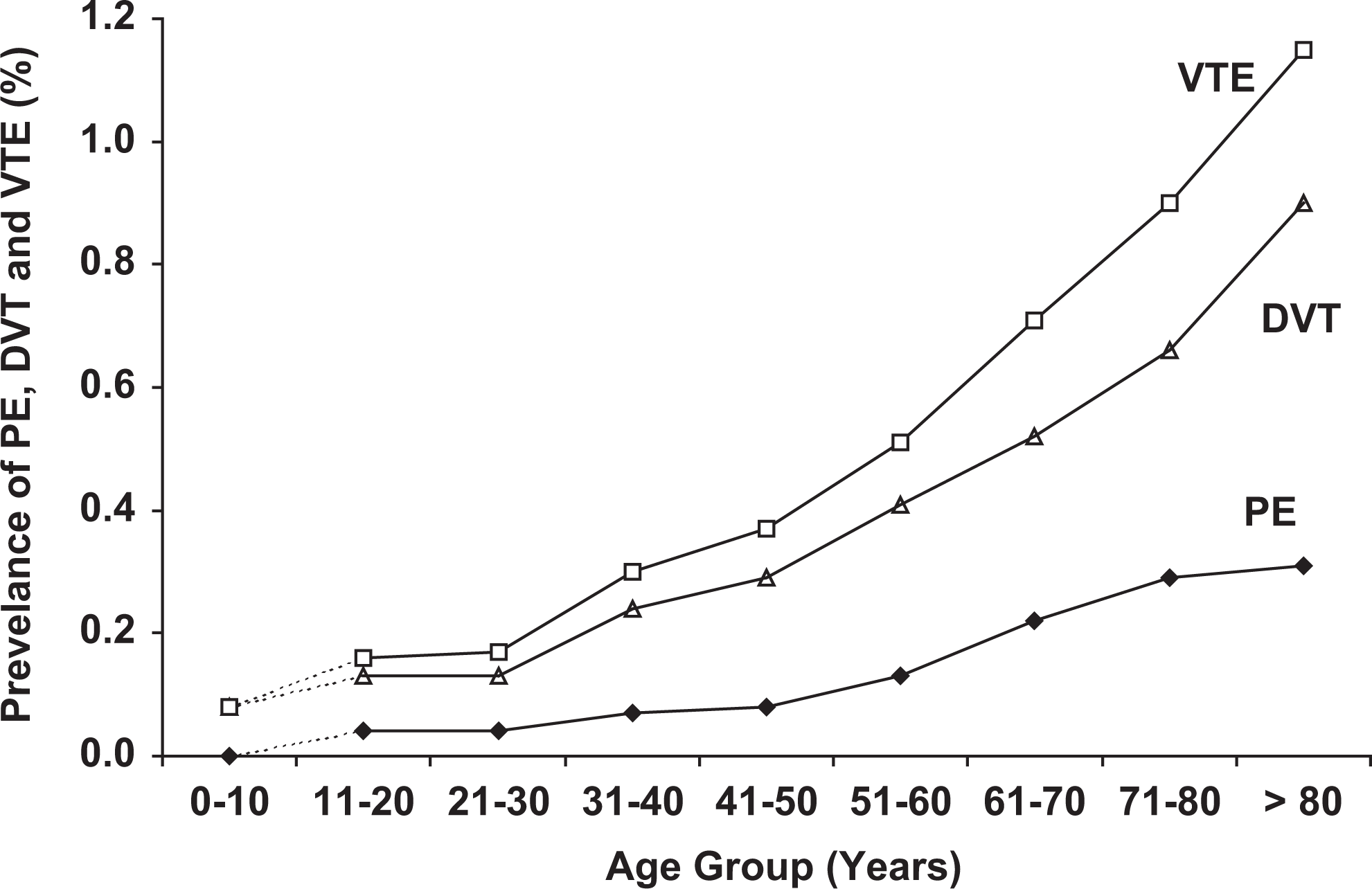
Prevalence of pulmonary embolism (PE), deep venous thrombosis (DVT), and venous thromboembolism (VTE) according to 10-year age groups. Broken lines indicate sparse data in patients aged 10 years or younger. The prevalence of DVT increased more with age than PE (0.11 DVT/10 years of age vs 0.04 PE/10 years of age). PE: r = .9579, P = .0002. DVT: r = .9678, P < .0001. VTE: r = .9724, P < .0001.
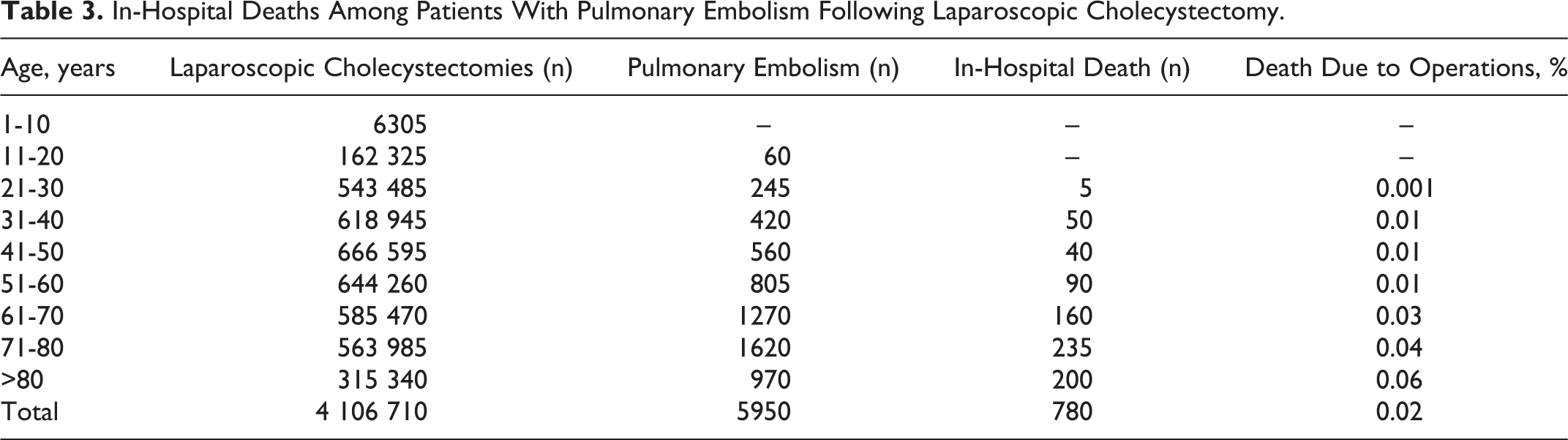
There were 780 (0.02%) all-cause in-hospital deaths among patients with PE following 4 107 430 laparoscopic cholecystectomies. The rate of death in patients with PE increased prominently with age (Table 3).
In-Hospital Deaths Among Patients With Pulmonary Embolism Following Laparoscopic Cholecystectomy.
Discussion
Among the 4 107 430 patients who underwent laparoscopic cholecystectomy, in-hospital PE occurred in 0.15%, DVT in 0.40%, and VTE in 0.53%. The incidence of PE, DVT, and VTE increased from 1998 to 2006. The prevalence of PE, DVT, and VTE is strongly age dependent. Older age has been described as one of the independent risk factors for VTE in patients undergoing laparoscopic cholecystectomy. 3,5,7,8
Most investigations of ≥40 patients showed PE in 0% to 0.2% of patients 8 –15 but 0.4% has also been reported 16,17 (Table 4). Regarding DVT, most reported 0% to 0.03% symptomatic DVT, 9 –12,14,20 although one investigator reported 1.7%. 13 Regarding VTE, most studies reported 0% to 0.2% 7,9 –12,14,19 but 0.36% and 1.7% were also reported 13,21 (Table 4). Pharmacologic antithrombotic prophylaxis appeared to show little impact on the prevalence of VTE 7,9,12,14 (Table 4). There was an increased risk of bleeding in those who received anticoagulant prophylaxis. 7 Fatal PE was not reported following laparoscopic cholecystectomy 9 –17,18 (Table 4), but we observed in-hospital PE-associated death in 0.02%.
Published Data on PE, DVT, and VTE Following Laparoscopic Cholecystectomy: Investigations of ≥40 Patients.
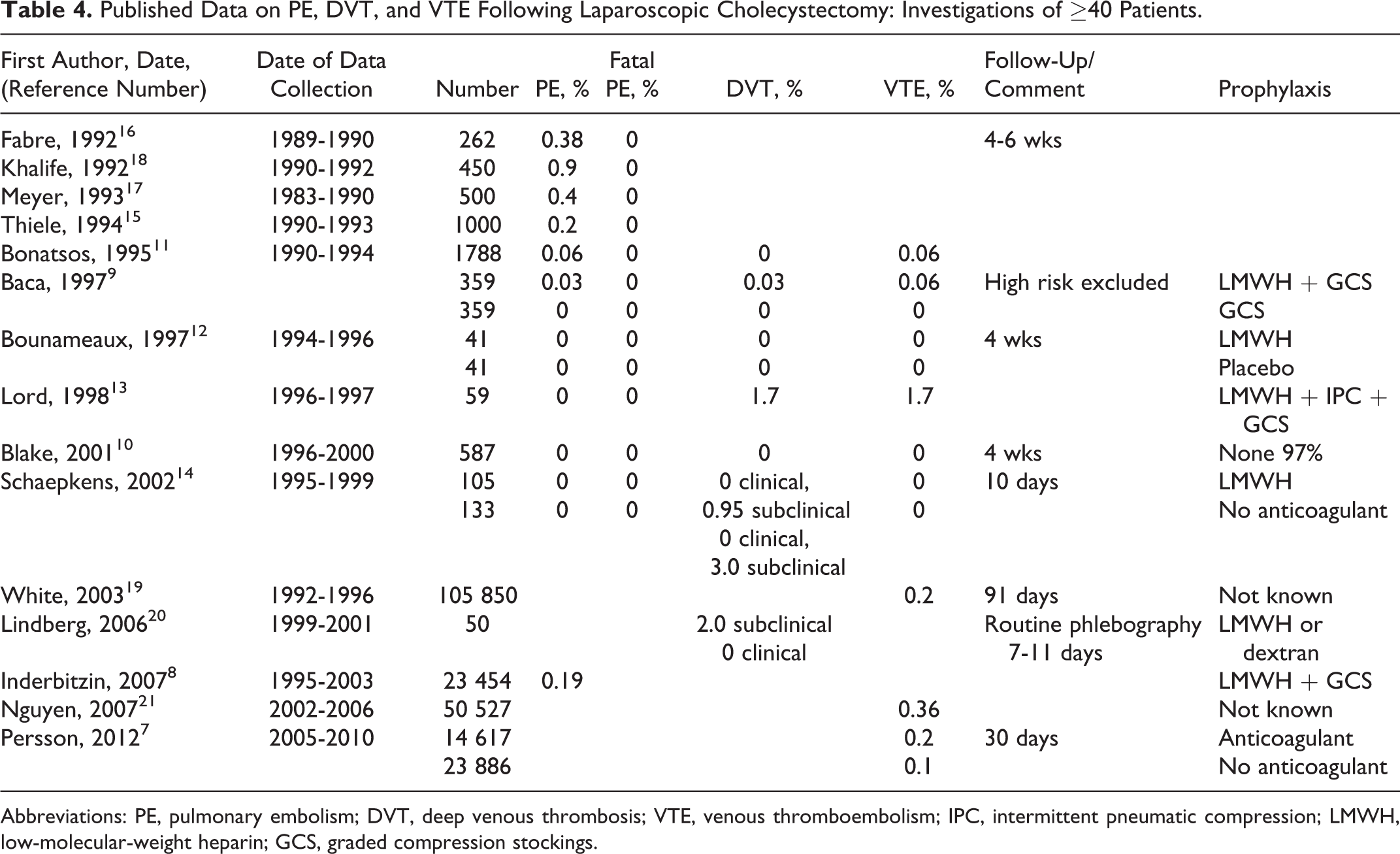
Abbreviations: PE, pulmonary embolism; DVT, deep venous thrombosis; VTE, venous thromboembolism; IPC, intermittent pneumatic compression; LMWH, low-molecular-weight heparin; GCS, graded compression stockings.
Pathophysiological factors that may lead to VTE following laparoscopic cholecystectomy include obstruction to venous outflow during surgical pneumoperitoneum and activation of the coagulation system. Decreased blood velocity or decreased venous outflow in the femoral veins during surgical CO2 pneumoperitoneum was observed by several 22 –28 but not all investigators. 29 Graded compression stockings reduced or abolished decreased blood velocity in one 26 but not in another investigation. 25 Similarly, intermittent pneumatic compression reduced or abolished decreased blood velocity in one 28 but not in another investigation. 27 Several investigations showed markers of postoperative hypercoagulability. 30 –37 One investigation showed no hemostatic changes in blood draining the lower limbs. 38 More sizeable changes in coagulation activation were observed in the elderly patients. 33 Perioperative changes in blood coagulation during laparoscopic cholecystectomy were smaller than during open cholecystectomy, 34,35 and changes were no greater than observed following low-risk surgery. 36
Strengths of these data are the huge number of patients with data obtained over 11 years from all regions of United State, all ethnicities, both genders, and all age groups. The similarity of our results with the results of a population-based study in California 19 attests to the robustness of the data. A weakness is that no follow-up information is available. Total VTE that we report would have been higher if the follow-up data were available. In the absence of follow-up, the prevalence of VTE in this study is probably underestimated. Another weakness is no information on antithrombotic prophylaxis. It is likely, however, that most did not receive prophylaxis with anticoagulants based on the recommendations of American College of Chest Physicians and the recommendations of the European Association for Endoscopic Surgery. 1,2,4 Many may have received graded compression stockings or intermittent pneumatic compression. Data on clinical rates of bleeding, spontaneous or in patients receiving pharmacological thromboprophylaxis, are not known. Risk factors for VTE and information on previous VTE are unknown. We cannot exclude the possibility that in some patients a VTE may already have been present before surgery. The method used for the diagnosis of VTE is not reported. It is not known whether the diagnosis was clinical or objectively confirmed by a radiological test.
Regarding the sensitivity of coding for PE, review and reabstraction of a sample of Medicare hospitalizations from late 1986 and early 1989 showed that 92% of codable cases for PE were on the abstract. 39 Throughout the United States, a 0.4% prevalence of PE in hospitalized patients ≥20 years of age, based on the National Hospital Discharge Survey's use of ICD-9 codes, 40 was similar to or the same as the incidences of PE (0.3% to 0.4%) in individual investigations. 41 –43 Regarding the discharge codes for DVT, 92% of the 198 coded cases of idiopathic DVT were valid. 44
In conclusion, the prevalence of in-hospital VTE following laparoscopic cholecystectomy is low and fatal PE is rare. Based on the guideline recommendations against anticoagulant prophylaxis unless patients have additional risk factors, it is likely that most patients we report did not receive anticoagulants. The risk of VTE following laparoscopic cholecystectomy increased with age, as did the risk of death in those who had PE. These data may be useful in assessing the use of thromboprophylaxis in patients undergoing laparoscopic cholecystectomy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.