
Abstract
We describe annual incidences and 6-month postoperative patterns of clinical venous thromboembolism (VTE) in 9078 patients undergoing major joint surgery in a Scandinavian hospital. In cohort I (1989-1999), low-molecular-weight heparin thromboprophylaxis for 7 to 10 days was uniformly introduced, 5-week thromboprophylaxis becoming routine after total hip replacement (THR), partially applied after hip fracture surgery (HFS), but not used after total knee replacement (TKR) thereafter (2003-2011; cohort II). Mean annual VTE incidence was lower in cohort II than in cohort I after THR and HFS but not after TKR. In cohort I, the cumulative VTE incidence increased sharply during the first 5 postoperative weeks in all groups, subsequently plateauing up to 6 months postsurgery. In cohort II, this incidence remained low and stable during 5 weeks post-THR, rising gradually up to 6 months, with a comparable but less pronounced pattern following HFS but not TKR. In conclusion, the VTE risk after major joint surgery seems to persist after 5- and 1-week prophylaxis in patients undergoing hip surgery and TKR, respectively.
Keywords
Introduction
Until now, the efficacy of antithrombotic agents for the in-hospital (10-14 days) and out-of-hospital (up to 35 days) prophylaxis of venous thromboembolism (VTE) after major orthopedic surgery has been principally appraised on the basis of trials using the surrogate variable of subclinical deep vein thrombosis as the main outcome. 1,2 However, the clinical relevance of this surrogate outcome has long been questioned. 3,4 The main criticism is that venographic screening may reveal small calf thrombi that dissolve spontaneously and are clinically unimportant, the rates of clinical VTE then being much lower. 3,4 Consequently, some surgeons consider recommendations based on such trials 1,2 to be clinically irrelevant and have challenged the statements of thromboprophylaxis guideline committees. 5,6
The focus has now switched from subclinical deep vein thrombosis to clinical events, that is, patient-important outcomes. 7 Based on the data from recent studies reporting low rates of postoperative clinical VTE, the American College of Chest Physicians has downgraded its recommendation to protect patients undergoing hip surgery beyond the hospitalization period (up to 35 days) from strong 1 to weak. 8 Considering that the latest improvements in the management of orthopedic patients have resulted in much shorter hospital stays, some authors even advocate that thromboprophylaxis should be limited to this brief hospitalization period (2-4 days). 9
To determine whether the recommendation to extend thromboprophylaxis beyond hospital discharge is valid in clinical practice, real-life data are needed. Using data extracted from a prospective regional registry, 10 –12 we analyzed over a 22-year period (1989-2011) the annual incidence of objectively confirmed clinical VTE after major lower limb joint surgery and the evolution of postoperative (up to 6 months postsurgery) patterns of occurrence of venous thromboembolic events in relation to the change in thromboprophylaxis recommendations around the millennium shift.
Materials and Methods
Patients
The Department of Medical Imaging, Vestre Viken Hospital Trust, Drammen Hospital, Norway serves a mixed urban and rural population of approximately 270 000. Patients with suspected deep vein thrombosis or pulmonary embolism are referred for radiological assessment to our department, which is the only imaging center for the satellite hospitals and general practitioners in the region covered by this central hospital. Data on clinical venous thromboembolic events occurring up to 6 months after surgery have been prospectively entered in a registry database at our hospital since 1989. 10 –12 Fatal events were not recorded in our registry, since they mainly occurred outside the hospital, with low rates of postmortem examination. This analysis was based on anonymous data extracted from the registry and approved for publication by the Regional Data Protection Officer.
In total, 10 672 patients were entered in the registry from 1989 until the end of 2011, of whom 5028 had undergone total hip replacement (THR), 1571 total knee replacement (TKR), and 4073 hip fracture surgery (HFS). Two cohorts of patients were considered. The first (cohort I) covers the period from 1989 to 1999, the second (cohort II) spanning the years 2003 to 2011. The years 2000, 2001, and 2002 (corresponding to 839 patients undergoing THR, 443 patients undergoing HFS, and 312 patients undergoing THR) were arbitrarily excluded from the analysis for the reasons explained subsequently.
Thromboprophylaxis
From 1989 onward, low-molecular-weight heparins were gradually introduced for VTE prophylaxis after major orthopedic surgery. By the second half of the 1990s, all patients undergoing major joint surgery were routinely receiving such prophylaxis for about 7 to 10 days (including after discharge if the hospitalization period was shorter than 7-10 days). At the Drammen hospital, thromboprophylaxis was administered subcutaneously, as dalteparin (Fragmin, Pfizer, Oslo, Norway) 5000 IU anti-Xa once daily or enoxaparin (Clexane/Lovenox, Sanofi-Aventis, Lysaker, Norway) 40 mg once daily, starting 12 hours before surgery in patients undergoing elective THR and TKR and shortly after hospital admission in emergency patients with hip fracture. Graduated compression stockings were not routinely applied.
The 3-year interval including 2000, 2001, and 2002 was considered as a transition period, during which a new low-molecular-weight heparin prophylaxis regimen was introduced in the view of accumulating evidence showing a benefit of extending this prophylaxis from about 7 to 10 days after THR surgery to 5 weeks postsurgery. 13 –16 The decision was taken to implement this regimen as hospital policy in all patients with hip replacement. Similar extended prophylaxis trials in patients undergoing TKR or HFS were lacking at that time. Short-term low-molecular-weight heparin protection for about 7 to 10 days therefore remained the local recommendation for these 2 groups. However, a shift in the surgical management of dislocated femoral neck fractures started shortly after 2002, when the standard practice of nailing these fractures was gradually replaced by prosthesis implantation. This change in surgical procedure was accompanied by the prescription of low-molecular-weight heparins for 5 weeks rather than 7 to 10 days in some patients undergoing HFS. The switch to longer prophylaxis was based on extrapolation of contemporary practice in patients undergoing prosthesis implantation in the context of elective surgery for osteoarthrosis as well as on emerging evidence of the benefit of extended thromboprophylaxis after HFS. 17 Based on this hospital policy, it is assumed that in cohort II (1) almost all patients undergoing hip replacement surgery received extended 35-day thromboprophylaxis, (2) almost all patients undergoing knee replacement surgery received the same duration of thromboprophylaxis as those in cohort I (ie, for 7-10 days), and (3) an intermediate proportion of patients undergoing HFS received extended 35-day thromboprophylaxis.
Diagnosis of VTE
In the early years of the register, patients with suspected deep vein thrombosis were investigated primarily by venography, whereas in more recent years, compression B-mode ultrasonography with routine examination of the deep, superficial, and common femoral and popliteal veins was used. If no thrombosis was seen on ultrasonography, supplementary venography was performed.
Pulmonary embolism was originally confirmed by chest x-ray in combination with ventilation perfusion lung scan. From 1996, spiral computed tomography took over, being superseded 4 years later by multislice computed tomography.
Statistical Analysis
Data on elective THR, TKR, and emergency HFS were analyzed separately.
The outcomes of interest were the annual incidence and postoperative (within 6 months) pattern of occurrence of objectively confirmed clinical (symptomatic) VTE. The annual incidence and timing of venous thromboembolic events in the 3 surgical groups were analyzed in terms of descriptive statistics. The annual incidence was expressed as the number of patients diagnosed each year and as the percentage of the total number of patients operated in each group. Trends in the annual incidence of VTE were determined by fitting lines through the data points using the locally weighted scatter plot smoothing function integrated in the statistical software. Comparisons of cohort I versus cohort II were expressed as risk ratios with corresponding 95% confidence intervals. P values of .05 or less were considered statistically significant. The Kaplan-Meier method was used to estimate the cumulative incidence rates of clinical VTE, starting from the day of surgery and continuing up to 6 months postoperation. Time-to-event estimates for the 2 cohorts were compared using the log-rank test. Hazard ratios (HRs) and corresponding 95% confidence intervals were calculated.
Statistical analyses were performed by the team’s professional statistician (AHP), using the software PASW Statistics 18 (IBM, Armonk, New York).
Results
Overall, 9078 patients underwent major lower limb joint surgery during the 2 periods analyzed, of whom 4189 underwent THR, 1259 TKR, and 3630 HFS. The mean age was 74.6 years, and women outnumbered men 2.3-fold (6334 vs 2744).
The first cohort, covering the period from 1989 to 1999, comprised 1950 patients undergoing THR, 542 patients undergoing TKR, and 2129 patients undergoing HFS. The second cohort, spanning the interval from 2003 to 2011, consisted of 2239 patients undergoing THR, 717 patients undergoing TKR, and 1501 patients undergoing HFS. Baseline characteristics by type of surgery and cohort are presented in Table 1.
Baseline Patient Characteristics.
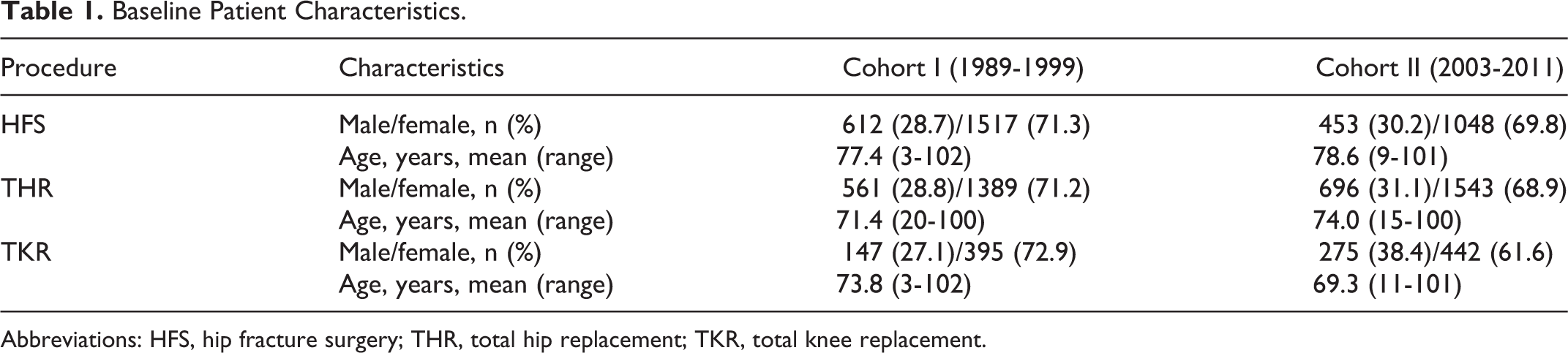
Abbreviations: HFS, hip fracture surgery; THR, total hip replacement; TKR, total knee replacement.
Long-Term Annual Incidence of Nonfatal Clinical VTE
From 1989 to 2011, a decrease in the annual incidence of objectively confirmed nonfatal clinical VTE was noted, falling from 4.6% to 1.2% in patients undergoing THR, from 6.3% to 2.5% in patients undergoing HFS, and from 7.7% to 0.0% in patients undergoing TKR (Figure 1; Table 2).
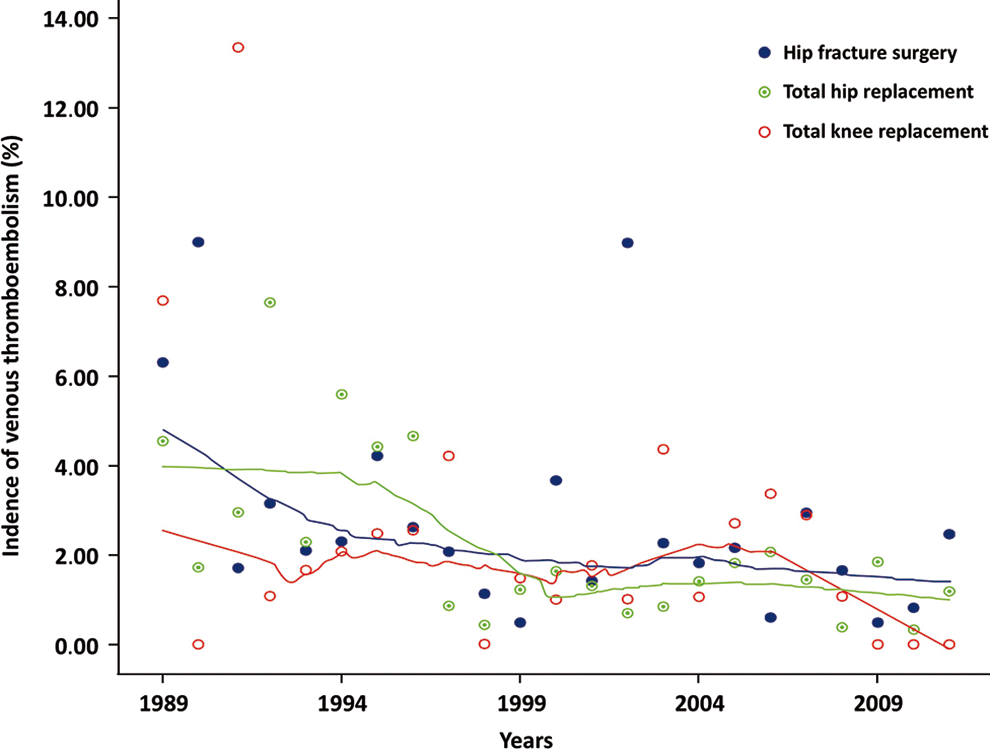
Annual incidence of clinical venous thromboembolism from 1989 to 2011. Circles represent annual incidence rates of objectively confirmed clinical venous thromboembolic events. Lines represent overall trends of the annual incidence rates of these events, as estimated by locally weighted scatter plot smoothing regression.
Annual Incidence of Clinical Venous Thromboembolism From 1989 to 2011.
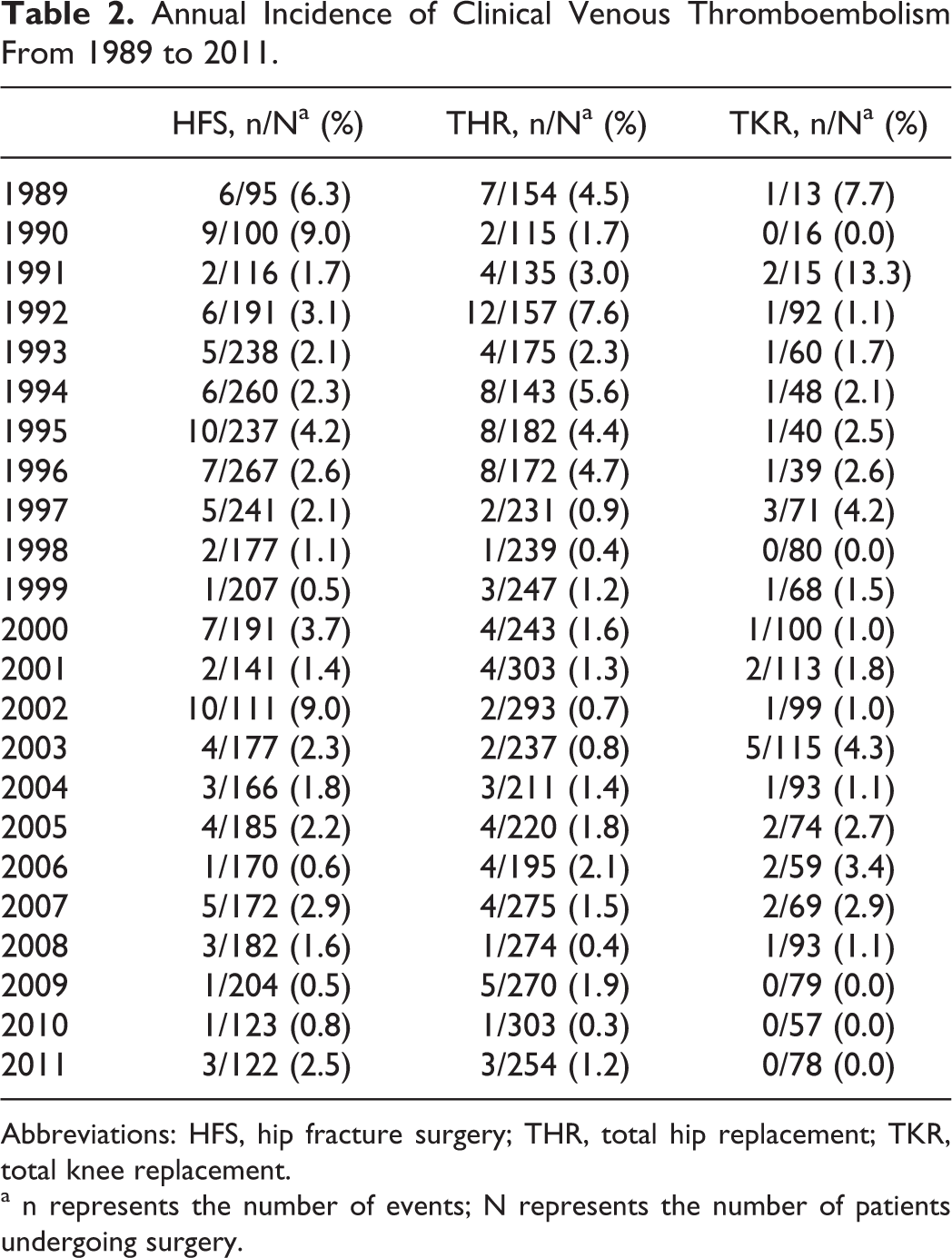
Abbreviations: HFS, hip fracture surgery; THR, total hip replacement; TKR, total knee replacement.
a n represents the number of events; N represents the number of patients undergoing surgery.
Comparison of the 2 cohorts showed that the mean annual incidence of nonfatal clinical VTE was statistically significantly lower in cohort II (2003-2011) than in cohort I (1989-1999) with regard to patients undergoing THR (1.2% vs 3.0%; P < .001) and patients undergoing HFS (1.7% vs 2.8%; P = .03; Table 3). No significant difference between the 2 cohorts was observed among patients undergoing TKR (1.8% in cohort II vs 2.2% in cohort I).
Mean Annual Incidence of Clinical Deep-Vein Thrombosis, Pulmonary Embolism, and Venous Thromboembolism in Cohorts I and II.
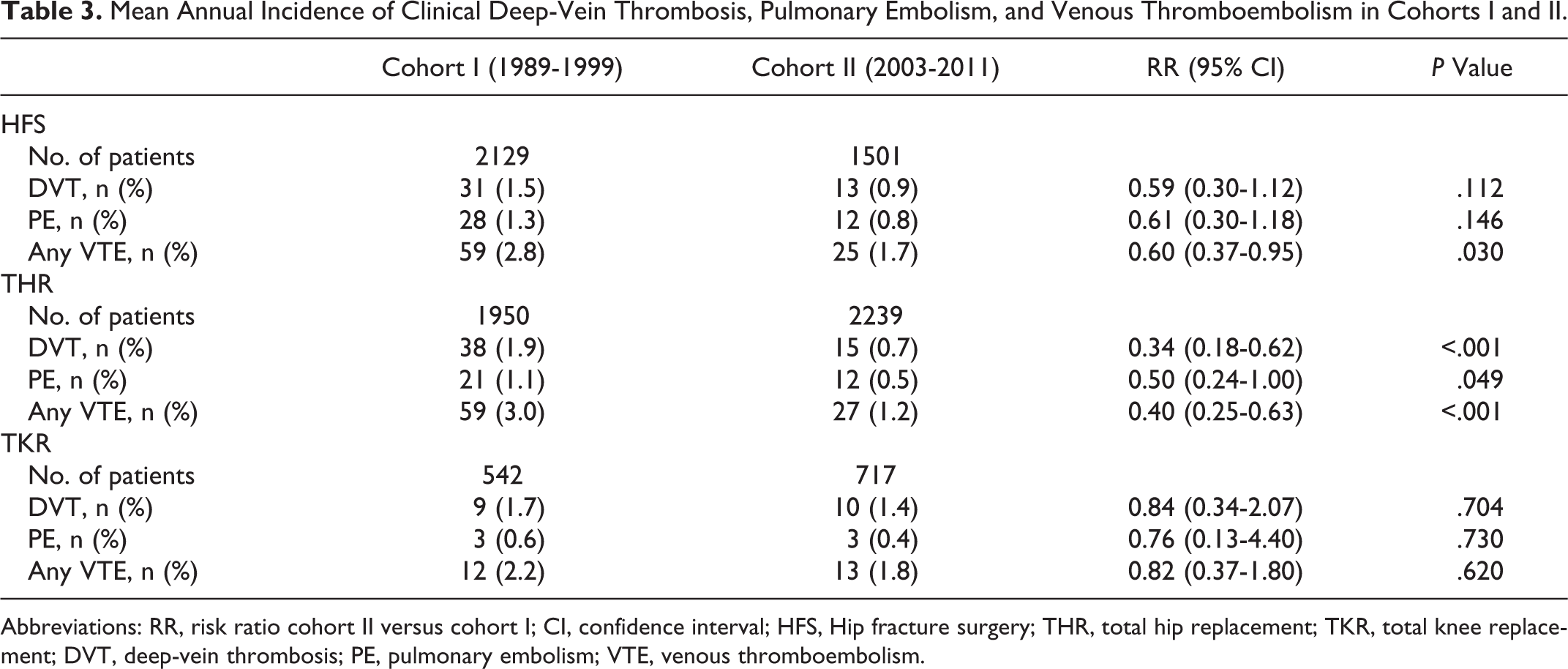
Abbreviations: RR, risk ratio cohort II versus cohort I; CI, confidence interval; HFS, Hip fracture surgery; THR, total hip replacement; TKR, total knee replacement; DVT, deep-vein thrombosis; PE, pulmonary embolism; VTE, venous thromboembolism.
Changes in the Pattern of Occurrence of Nonfatal Clinical VTE Up to 6 Months Postsurgery
During the first period (cohort I), a marked increase in the cumulative postoperative incidence of objectively confirmed nonfatal clinical venous thromboembolic events was seen within the first 30 to 40 days (about 5 weeks) postsurgery in all 3 groups, subsequently tending to plateau for up to 6 months after surgery (Figures 2 –4).
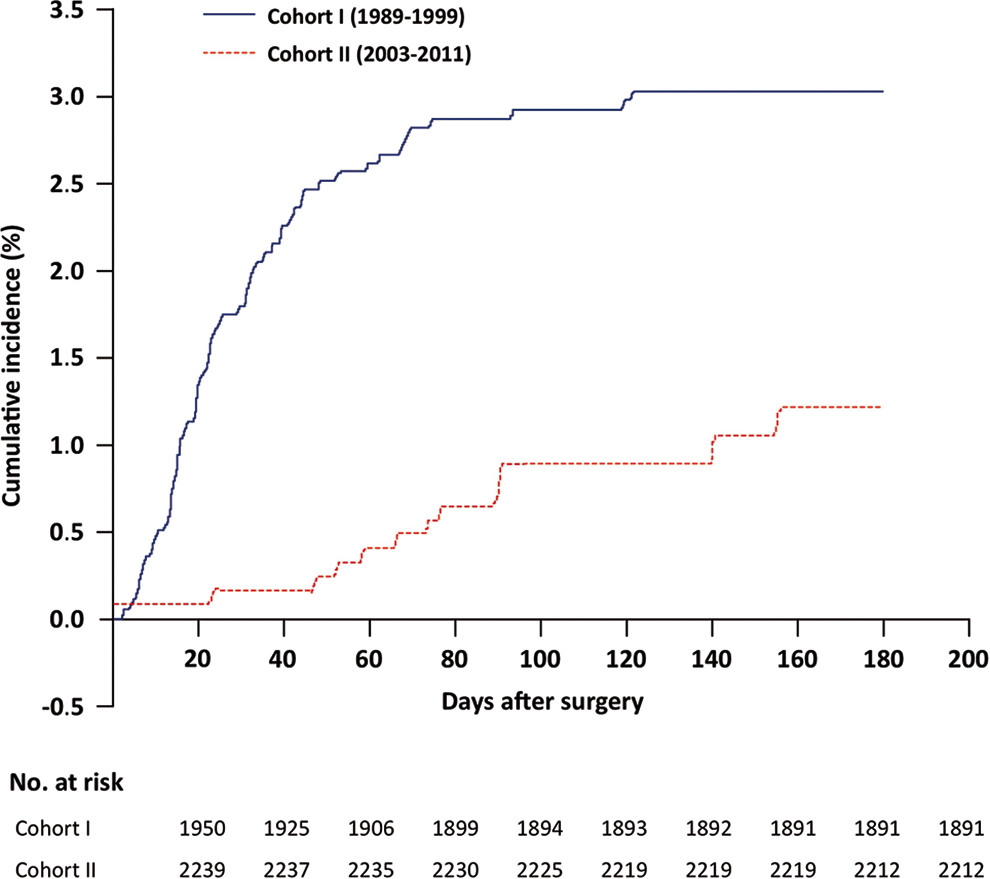
Cumulative incidence of clinical venous thromboembolism up to 6 months after total hip replacement surgery in cohorts I and II. Solid blue line: cohort I (1989-1999); dashed red line: cohort II (2003-2011).
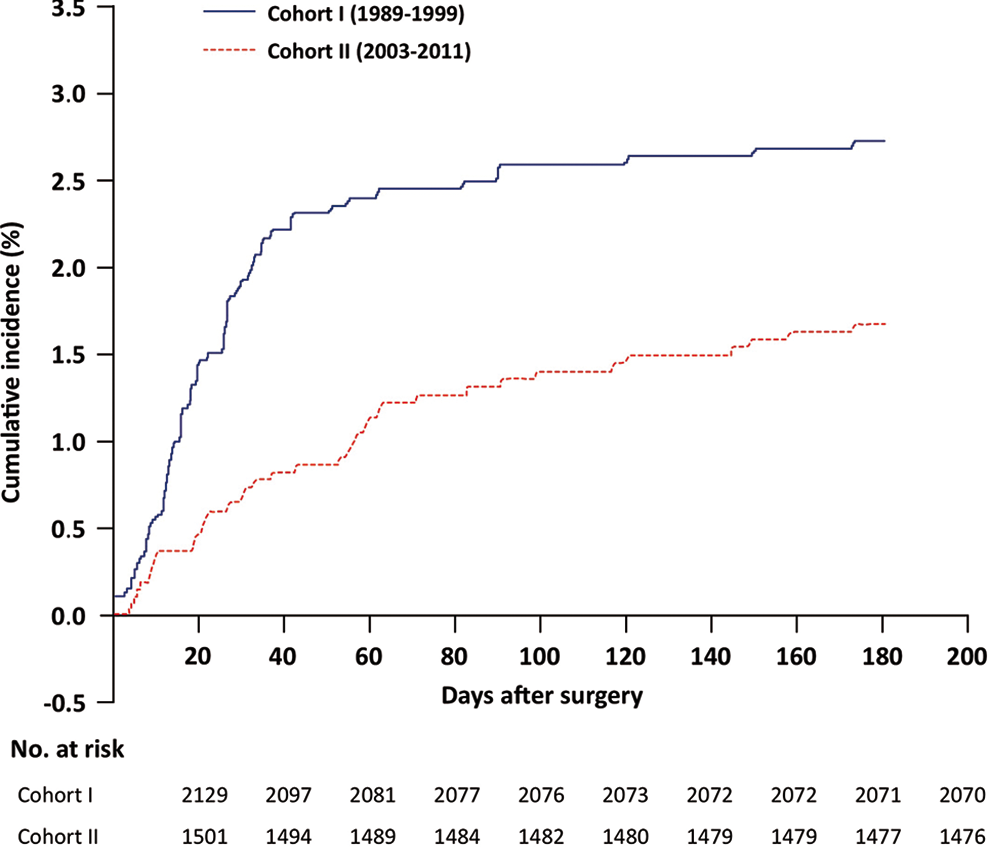
Cumulative incidence of clinical venous thromboembolism up to 6 months after hip fracture surgery in cohorts I and II. Solid blue line: cohort I (1989-1999); dashed red line: cohort II (2003-2011).
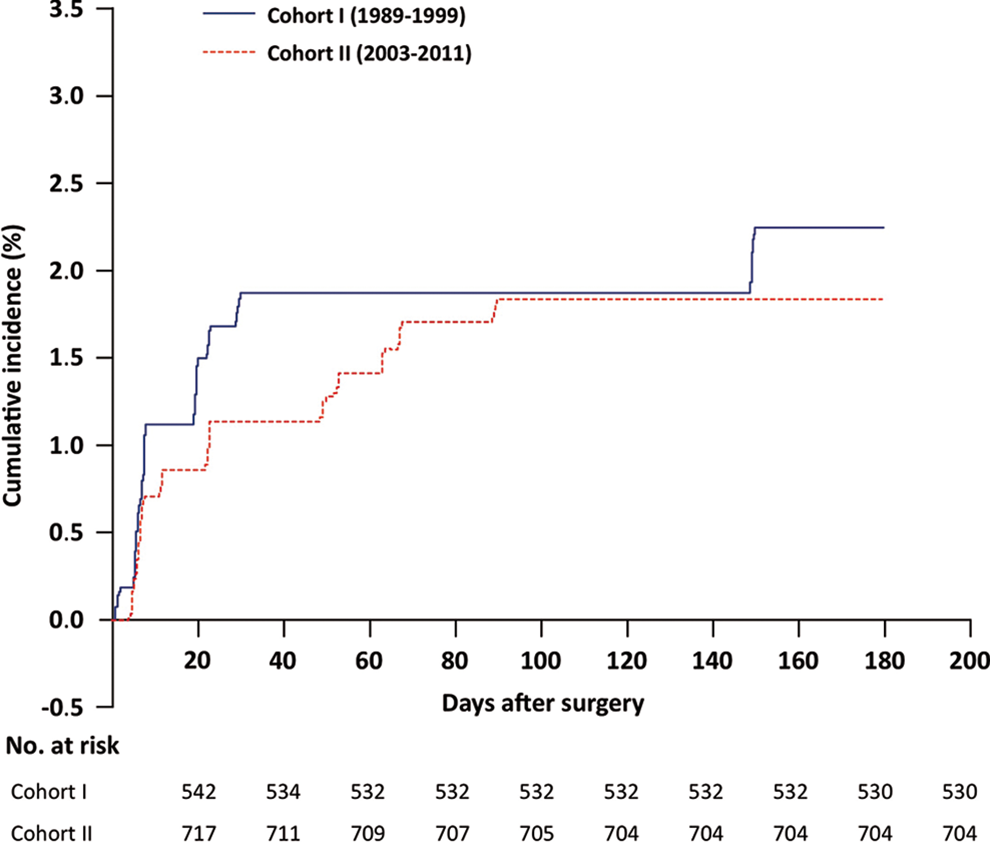
Cumulative incidence of clinical venous thromboembolism up to 6 months after total knee replacement surgery in cohorts I and II. Solid blue line: cohort I (1989-1999); dashed red line: cohort II (2003-2011).
During the second period (cohort II), the pattern differed according to the type of surgery. In patients undergoing THR, the cumulative incidence of nonfatal clinical VTE remained low and stable until about 5 weeks after surgery, when it started to gradually rise, reaching a plateau about 3 months postsurgery (Figure 2). The 6-month cumulative incidence of nonfatal clinical VTE was statistically significantly lower in cohort II than in cohort I (HR: 0.436, 95% confidence interval: 0.281-0.676; P < .001). A comparable, though less pronounced phenomenon was observed in cohort II following HFS (Figure 3): the cumulative incidence increased moderately up to about 2 to 3 months postsurgery to reach a plateau, parallel to that seen in cohort I. As observed in patients undergoing THR, the 6-month cumulative incidence of nonfatal clinical VTE was statistically significantly lower in cohort II than in cohort I (HR: 0.582, 95% confidence interval: 0.362-0.936; P = .026). Following TKR surgery, the 2 cohorts showed only slightly different patterns of increasing cumulative postoperative incidence of VTE, reaching nearly the same terminal plateau (HR: 0.816, 95% confidence interval: 0.373-1.789; P = .613; Figure 4).
Discussion
This long-term cohort study showed a decrease in the annual incidence of symptomatic, nonfatal VTE over more than 2 decades in patients having undergone THR and HFS. In contrast, this incidence remained stable in patients undergoing TKR, except for a final drop that is difficult to interpret considering the small number of patients and events recorded. The mean annual incidences observed in the first cohort are close to those reported in randomized or observational studies of short-term thromboprophylaxis after total hip (1.7%-4.3%) or knee (1.4%-2.4%) replacement, 13,18 –20 and HFS (2.7%). 17 In the second cohort, the mean annual incidence observed in patients undergoing THRis likewise in the range of those reported in similar patients receiving extended thromboprophylaxis (1.3%-2.3%). 13,21,22 However, the mean annual incidence in patients undergoing HFS was higher than those reported in other studies in such patients protected for 5 weeks after surgery (0.3%-1.34%). 17,23
We believe that these findings are mainly related to improvements in thromboprophylaxis management in our region during the 22-year study period. During the first decade, low-molecular-weight heparin prophylaxis for about 7 to 10 days was gradually implemented in all groups. The introduction of a 5-week prophylaxis regimen in patients undergoing THR coincided with a drop to a low-stable annual incidence of symptomatic, nonfatal VTE. A similar pattern was observed in patients undergoing HFS, though the decrease was less pronounced, probably because thromboprophylaxis duration was initially left to the surgeons’ discretion. Extended thromboprophylaxis was implemented only later, and partially, after the switch from fracture repair by nailing to prosthesis implantation. No decline in the annual incidence of symptomatic, nonfatal VTE was seen in patients undergoing TKR, probably because the thromboprophylaxis regimen remained unchanged in this setting.
It could be argued that increasing use of regional anesthesia, improvement in surgical techniques and early mobilization, 9,24 more liberal use of concomitant drugs such as aspirin and statins, inclusion of patients in more healthier condition over time, and use of ultrasonography in cohort II rather than venography in cohort I might explain some of the decline in VTE incidence observed in our study. However, we believe that these factors are marginal as (1) they should also have led to a drop in the incidence of VTE after TKR, which was not observed in our study; (2) studies investigating temporal trends in the prevalence of comorbidities all showed that patients undergoing hip replacement or TKR tended to be increasingly sick irrespective of whether the average age of the patients operated was increasing or decreasing 25 –28 ; (3) the benefit of early mobilization and regional anesthesia in reducing the risk of VTE has never been reliably demonstrated 6 ; (4) ultrasonography is commonly acknowledged to have a sensitivity comparable to that of venography for confirming symptomatic deep vein thrombosis; furthermore, if no thrombosis was seen on ultrasonography, supplementary venography was performed; (5) several other contemporary observational studies failed to demonstrate such a decline after total hip replacement surgery 29 or TKR surgery 30 –32 , despite gradual improvements in perioperative patient management; Danish investigators suggested that this was principally due to the lack of compliance with guidelines for postdischarge thromboprophylaxis while at the same time the duration of hospitalization continuously declined during the study periods. 29,31 Finally, our results agree with those of a retrospective analysis of a US database showing that in patients undergoing THR and TKR, the incidence of VTE was strongly associated with the duration of thromboprophylaxis. 33
In our study, the impact of thromboprophylaxis duration on the risk of nonfatal clinical VTE was also revealed by the pattern of the 6-month cumulative postoperative incidence of events. Patterns similar to those seen in patients undergoing THR and TKR in our first cohort, receiving short-term prophylaxis, had already been reported showing, as in the present study, that the risk of VTE persists for about 3 months and 1 month, respectively. 18,20 A recent investigation based on the data from the Danish Hip Arthroplasty Registry showed that the risk of symptomatic VTE following THR was substantial within 90 days after surgery and even persisted up to 1 year postsurgery (although the absolute risk was small) compared with the general population. 34 Data on patients undergoing HFS have been previously reported only from our Scandinavian registry, evidencing a rapid postoperative increase in cumulative risk, which persisted for more than 3 months. 12 To the best of our knowledge, patterns similar to those seen in patients undergoing hip surgery in our second cohort have never been reported before. In patients undergoing THR, the 5-week prophylaxis regimen was associated with a stable low cumulative postoperative incidence of nonfatal clinical VTE that tended to increase when prophylaxis ended, suggesting that this was stopped too early while patients were still at risk. In patients undergoing HFS, the cumulative incidence of events in cohort II was substantially lower than in cohort I but still higher than in cohort II of patients undergoing THR, probably because a 5-week prophylaxis regimen was less consistently applied in this group. In contrast, the patterns of the postoperative cumulative risk of events were almost the same in the 2 cohorts of patients undergoing TKR, a finding consistent with the use of similar thromboprophylactic regimens in these cohorts.
Our study has the potential limitations inherent to retrospective analyses (although the data were recorded prospectively). In addition, the rates of VTE are probably underestimated as (1) fatal postsurgical pulmonary embolism was not recorded but may have occurred both in and outside hospital and (2) in the early years of the observation period, pulmonary embolism was diagnosed only on the basis of high-probability lung scans, so patients with intermediate probability were excluded, likely resulting in further underestimation of the actual rates in cohort I. Finally, we did not address the issue of the impact of thromboprophylaxis on overall mortality, 13,35 –39 as we believe this question is beyond the scope of the present study and warrants a specific investigation matching our database with the National Death Register. The strengths of our study, besides its very long duration, are that perioperative management strategies, and anticoagulant regimens were homogeneous across all patients; moreover, all thromboembolic outcomes were objectively confirmed in a single-imaging department, all patients in the region being readmitted to the same radiological unit, without any selection. Thus, we believe our findings provide valid estimates of the risk of symptomatic, nonfatal VTE and reflect clinical practices over a long period.
In summary, the findings of this 22-year longitudinal cohort study support the efficacy of extended thromboprophylaxis in reducing the risk of symptomatic, nonfatal postoperative VTE after major joint surgery. However, the data also show that the risk seems to persist after 5- and 1-week prophylaxis in patients undergoing hip surgery and TKR, respectively. Pending availability of biological markers enabling identification of patients still at risk and individualized thromboprophylaxis regimens, our data suggest that 3-month protection following THR and HFS and about 1-month protection after TKR seem reasonable practice to prevent such events for all patients, with the exception of those at increased bleeding risk. Nevertheless, prior to recommendation of such a strategy, its favorable benefit–risk ratio needs to be demonstrated for each drug individually.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.