
Abstract
Spontaneous intracerebral hemorrhage (sICH) represents a devastating clinical event with high mortality and morbidity rates. Only few patients with sICH are treated with neurosurgical evacuation of the hematoma, and the majority of them need only a good conservative medical approach. The goal of medical treatment is to avoid secondary neurological and systemic complications. Venous thromboembolism (VTE) represents one of the most feared complications of sICH, and it is a potential cause of death. The balance between the benefit of VTE prevention and the risk of hematoma enlargement and/or rebleeding with the use of pharmacologic thromboprophylaxis remains controversial because of the lack of consistent evidences in the literature. The efficacy of mechanical prophylaxis is also uncertain. Consequently, until now there are no clear guidelines and scientific evidences available for physicians in this field. The aim of this review is to analyze the available literature and guidelines about pharmacological VTE prophylaxis in patients with nonsurgical sICH.
Keywords
Background
Spontaneous intracerebral hemorrhage (sICH) results from the rupture of blood vessels in the brain. 1 Radiologic evidence of ICH at the time of stroke is present in 10% to 15% of all the patients with stroke. 2 The incidence of sICH is 24.6/100.000 people/year worldwide (range 1.8-129.6/100.000 people/year), 3 and it is estimated that more than 2 million of about 15 million strokes worldwide are sICH, each year. 2 In the last decades, hospital admissions for sICH are increased by 18%. 4 The sICH mortality rate approaches 40% at 30 days and 60% at 1 year of the event, 3 with half of the deaths occurring in the first 2 days. 2
One third of patients during the first 24 hours from sICH presentation show a substantial increase in the volume of the hematoma; in 66% of them, the enlargement becomes evident in the first hour from symptoms onset.1,5–8 Pathophysiologically, hematoma growth seems to be caused by continuous bleeding from the initial site or by additional bleeding from adjacent damaged vessels.1,5– 9 Various predisposing factors have been associated with hematoma enlargement, including previous use of antithrombotic or anticoagulants drugs, blood systolic hypertension, alcohol abuse, irregularly shaped hematomas and spot signs, hypofibrinogenemia, decreased levels of prothrombin, diabetes mellitus, and liver diseases. Hematoma enlargement is associated with poor prognosis; therefore all efforts aimed to limit this growth are of vital importance.1,2,5–19
Venous thromboembolism (VTE), encompassing pulmonary embolism (PE), and deep vein thrombosis (DVT) represents one of the most feared medical complications of ICH. In more than 90% of the cases, emboli originate in the lower limbs. 20 Patients with neurological injury or neurosurgery are highly susceptible to this complication, especially after the first week of hospitalization, with associated mortality as high as 60%. 21 In this population, the reported incidences of VTE range from 18% to 50% for DVT and from 0.5% to 5% for PE, but the rates have reached 25% in autopsy series.22–29 Patients with sICH are at increased risk of VTE complications,25,26 and this risk was reported to be up to 4-fold higher than in patients with acute ischemic stroke. 30 A review of a database encompassing more than 1.6 million patients with sICH revealed that symptomatic VTE occurs in 2% of patients with sICH, with PE occurring in around 0.7% and DVT in 1.3% of patients, 27 whereas small case series reported symptomatic VTE rates ranging from 31 0.5% to 13%. Incidence of asymptomatic DVT assessed by a routine investigation has been reported as high as 75% in patients with residual hemiplegia not receiving thromboprophylaxis. 32 Pulmonary embolism-related mortality occurs in about 5% of patients with sICH. 28
Few studies have analyzed specific risk factors for VTE in sICH. Advanced age, female sex, obesity, prolonged immobilization, leg paralysis, lobar localization, larger diameter of ICH, score ≥12 in National Institute of Health Stroke Scale, and withholding of previously ongoing oral anticoagulant treatment (OAT) have all been associated with a higher risk to develop VTE.33–36 Emergent reversal of anticoagulation is considered standard treatment for the management of OAT-related ICH, with the use of prothombin complex concentrates (PCCs), fresh frozen plasma, recombinant activated factor VII (rFVIIa), and vitamin K1 (VK1). 37 However, the incidence of VTE following these interventions has been reported to increase, especially for PCC and rFVIIa; much recent evidence of literature demonstrate a 5% VTE rate following rFVIIa and 0.7% to 1.9% thromboembolic events following 3 or 4 factors PCCs.38,39
When VTE events occur in patients with sICH, both anticoagulants and caval filters should be taken into account, but unfortunately, these choices could be at high risk of adverse events, and mortality and morbidity burden could be superior to the risks associated to sICH. 40
Based on these observations, it becomes clear that the prevention of VTE should become a major goal in the management of patients with sICH. However, the most effective prophylactic strategies, namely anticoagulant drugs, are potentially associated with an increased risk of intracranial rebleeding, and safer alternative physical strategies such as graduated compression stockings (GCSs) and/or intermittent pneumatic compression (IPC) may be inadequately effective in this setting. Unfortunately, there is scant information from clinical trials and recommendations from guidelines that may be of little help to the practicing clinician. The applicability to the patients with sICH of current recommendations on VTE prophylaxis in similar settings, such as neurosurgery or posttraumatic intracranial hemorrhage, remains unclear. Our objective is, therefore, to carry out an exhaustive literature review to assess all available evidences and to explore what we currently know about pharmacological prophylaxis in the clinical scenario of nonsurgical sICH.
The VTE in Neurosurgery and in Patients With Traumatic Intracerebral Hemorrhage
In neurosurgery ICH patients, meta-analyses have demonstrated that pharmacological thromboprophylaxis with unfractioned heparin (UFH) or low-molecular-weight heparin (LMWH) is effective and relatively safe.41– 43 It was estimated that for every 1000 patients receiving pharmacological prophylaxis with either UFH or LMWH, 91 symptomatic or asymptomatic VTE events could have been avoided at the cost of 7 sICHs. 41 Current recommendations for VTE prophylaxis in neurosurgical ICH patients include the use of IPC postoperatively, with or without concomitant GCS (grade 1A); low dose UFH started perioperatively (grade 2B) or LMWH started postoperatively (grade 2A). 44
Concern also exists for VTE prophylaxis after traumatic ICH. Only 1 small quasi-randomized clinical trial has compared anticoagulant prophylaxis versus IPC in patients with intracranial hemorrhage following trauma. 45 Because of the small sample size, the study was inconclusive substantially reporting neither benefit nor harm with the use of anticoagulant. 37 All other studies suggesting a favorable efficacy to safety profile of pharmacologic prophylaxis with LMWH had no control groups and their results should be interpreted with great caution.46–48 It is therefore of no surprise if surveys on clinical practice patterns of VTE prophylaxis in this setting show that the fear for hematoma progression limits the use of pharmacological strategies in the patients with traumatic ICH. 49
The Management of VTE Risk in the Patients with Nonsurgical sICH
The same uncertainty applicable to VTE prophylaxis in surgical and traumatic ICH applies to the patients with nonsurgical sICH, for whom the indication and timing of anticoagulant prophylaxis also remains controversial, and most of the patients receive safer physical methods. The lack of adequate evidences to drive clinicians through these difficult decisions requires a careful individual assessment of the risks and benefits of prophylactic strategies. It should be remarked in this context that the randomized clinical trials aimed to evaluate the role of pharmacological prophylaxis in ill medical patients, such as MEDENOX, PREVENT, ARTEMIS, and PREVAIL with LMWH and fondaparinux, have excluded patients with recent sICH 50–53 as well as those with new oral anticoagulants such as MAGELLAN with rivaroxaban 54 and ADOPT with apixaban. 55
Mechanical prophylaxis with GCS and/or IPC has been shown to be effective in surgical patients for the prevention of VTE and is considered the first choice in patients with contraindications to pharmacological prophylaxis. 44 Little evidences have been available over the last years on the efficacy of mechanical prophylaxis in patients with stroke and these have demonstrated the failure of GCS in reducing the occurrence of DVTs and deaths when compared with placebo;56–58 whereas in the association of IPC with GCS, the 2 strategies resulted in a significant reduction in the rate of VTE compared with GCS alone (16.9% vs 4%). 59
Studies on VTE Pharmacological Prophylaxis in Patients With sICH
Articles search strategy is described in Box 1. From 319 articles emerged from searching process, we selected 9 articles reporting data of clinical studies that analyzed the effectiveness and safety of pharmacological prophylaxis in sICH.60–68 Figure 1 shows the articles selection process and Table 1 summarizes characteristics of the selected studies.
Search strategy
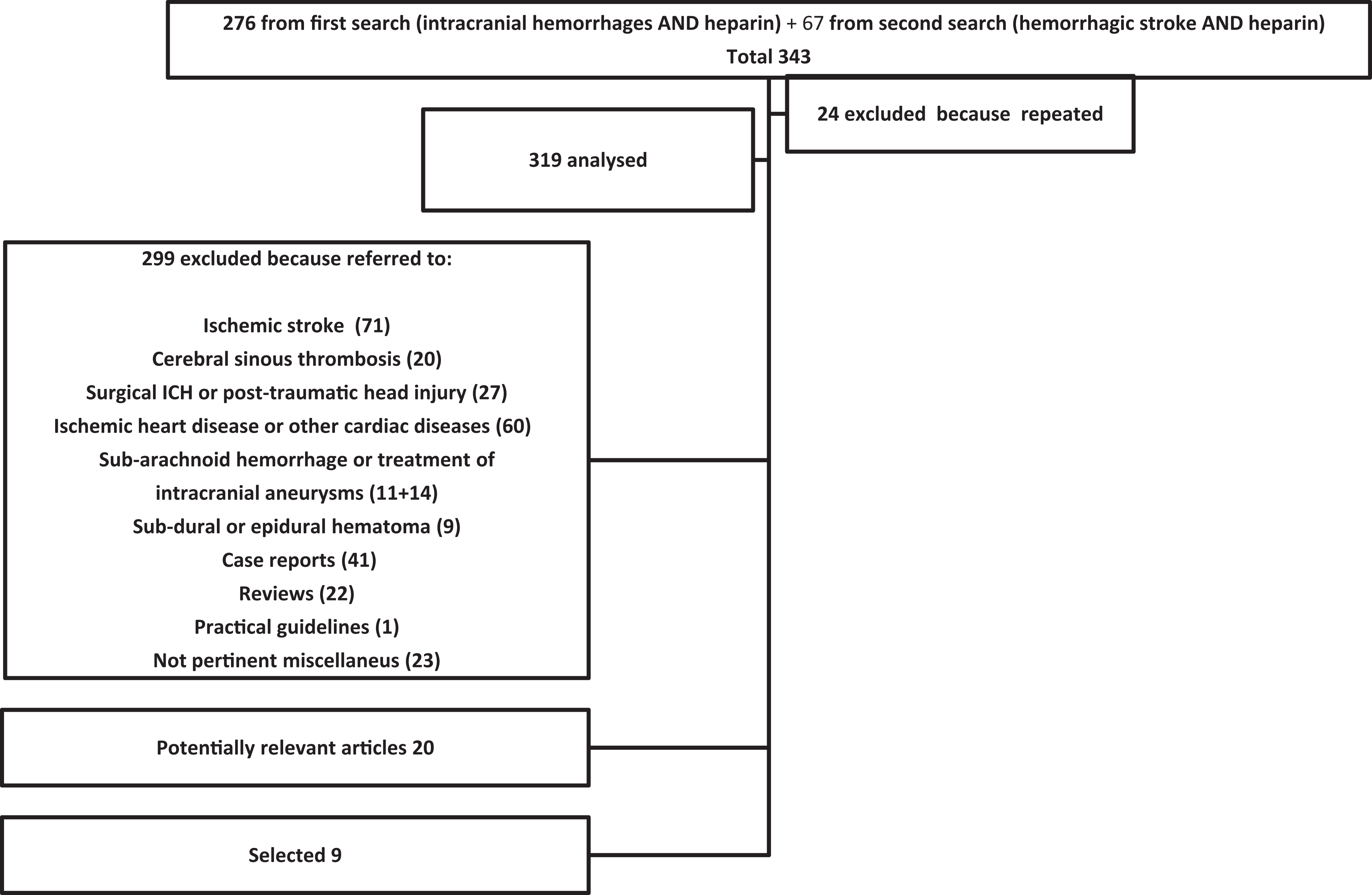
PubMed articles selection process.
Summary of Studies Aimed to Evaluate Pharmacological VTE Prophylaxis in Patients With ICH
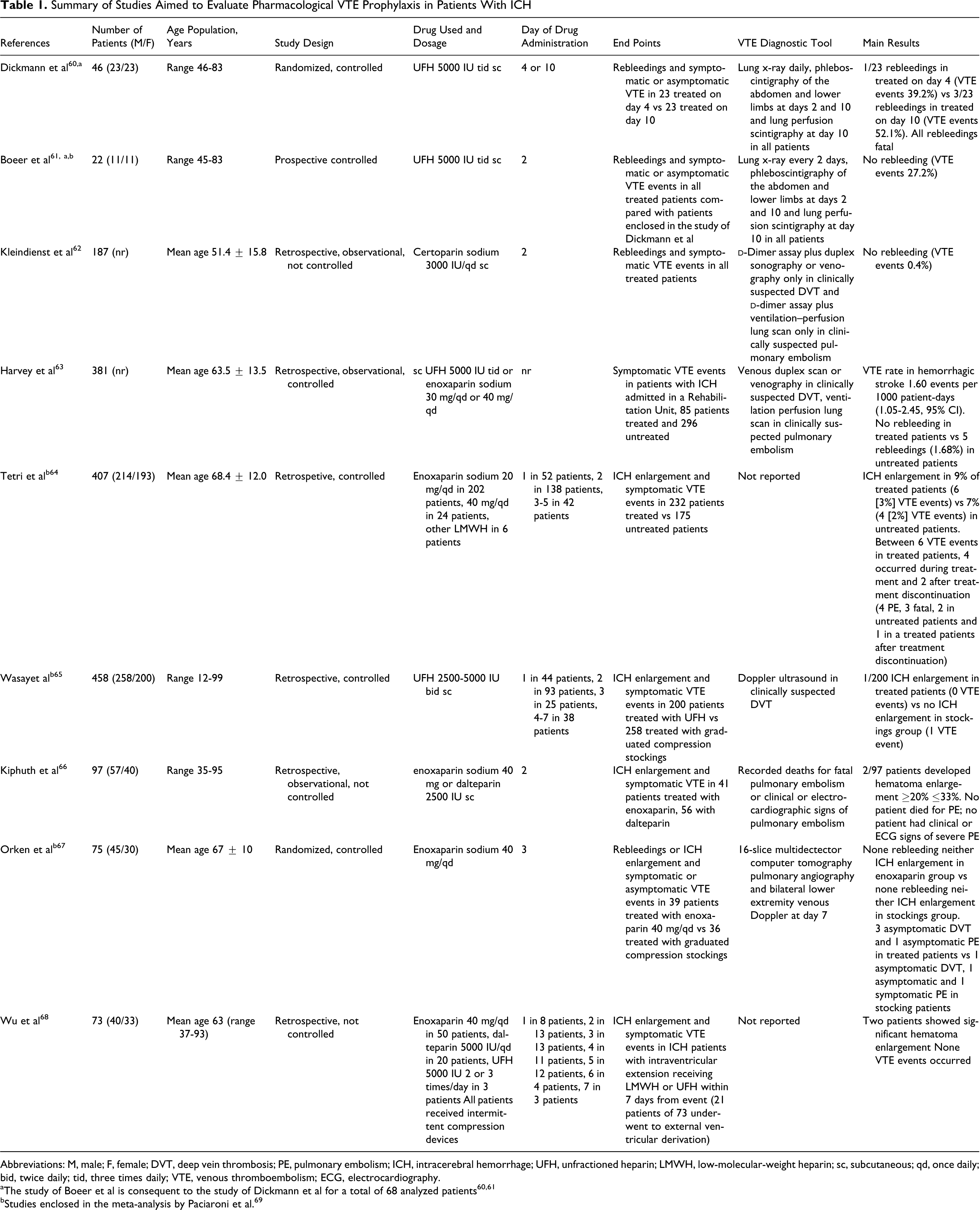
Abbreviations: M, male; F, female; DVT, deep vein thrombosis; PE, pulmonary embolism; ICH, intracerebral hemorrhage; UFH, unfractioned heparin; LMWH, low-molecular-weight heparin; sc, subcutaneous; qd, once daily; bid, twice daily; tid, three times daily; VTE, venous thromboembolism; ECG, electrocardiography.
aThe study of Boeer et al is consequent to the study of Dickmann et al for a total of 68 analyzed patients60,61
bStudies enclosed in the meta-analysis by Paciaroni et al. 69
Overall, 1746 patients with sICH were included. Three of these studies are randomized controlled trials, but 1 is partially a duplicate with the addition of 22 new patients to 46 patients enrolled in the previous study.60,61,67 Six are retrospective cohort studies,62–66,68 3 of which are with a control group.63–65 Although the outcomes varied across the studies, most included ICH enlargement,64–68 rebleedings,60–63 and all included VTE events.60–68 The UFH was used in 5 studies and60,61,63,65,68 LMWH in 6 studies.62–64,66–68 Of the 981 patients who received pharmacological prophylaxis, 654 (66.6%) were started on treatment within 48 hours and 958 (97.6%) patients received pharmacological prophylaxis within the first week from hospital admission. The VTE was systematically detected in all the patients using diagnostic tools in only 3 studies,60,61,67 whereas it was researched only in clinically suspected patients in other 3 studies.62,63,65 In the study of Kiphuth et al, only the documented deaths for fatal PE or clinical or electrocardiophic signs of PE detected by reviewing data records were considered as VTE episodes. 66 Finally, 2 studies did not report the diagnostic tools used for VTE diagnosis.64,68
In the studies by Dickmann et al and Boeer et al, UFH 5000 IU was administered 3 times daily and started after 48 hours from sICH onset, resulting to be safe (no rebleeding) and more effective than the same treatment started between days 4 and 10.60,61 However, the observed VTE rate was very high with this drug regimen (range 27.2%-52.1%). In the study by Wasay et al, low dose UFH resulted effective and safe regardless of the day of initiation, with a VTE rate 65 of 0%. Overall, these studies seem to suggest the safety of pharmacologic prophylaxis event when started early, that is within 48 to 72 hours.61,62,64– 68 However, no study could show a clear advantage in efficacy when pharmacologic prophylaxis was compared with mechanical devices.65,67
Recently, Paciaroni et al 69 carried out a meta-analysis of controlled studies performed in this setting.61,64,65,67 This study found that the use of UFH and LMWH results in a significant reduction in the risk of symptomatic and asymptomatic PE (risk ratio 0.37, 95% confidence interval [CI]: 0.17-0.80), with no effect on the risk of symptomatic and asymptomatic DVT (relative risk [RR] 0.77, 95% CI: 0.44-1.34, P = .36) and no effect on the risk of all-cause mortality (RR 0.76, 95% CI: 0.57-1.03). Of interest, pharmacologic prophylaxis was also not associated with a significant increase in the risk of any hematoma enlargement (RR 1.42, 95% CI: 0.57-3.53). 69 However, the authors underlined that no definite conclusions could be drawn from the results of their analysis because of a low quality of included studies and an insufficient statistical power.
After the publication of this meta-analysis, Wu et al published a study on the safety of pharmacological prophylaxis in patients with sICH with or without intraventricular bleeding. 68 This study showed that both LMWH and UFH were effective in reducing the risk of VTE (any VTE) and safe with respect to hematoma enlargement both when administered within 48 hours and when administered within 4 days. 68
Current Guidelines
Several guidelines from the United States and Europe have addressed the issue of VTE prophylaxis in the patients with sICH.2,30,70– 78 Of course, all recommendations are uniformly based on poor levels of evidence, reflecting the need for more rigorous and better designed clinical studies. For example, American College of Chest Physicians (ACCP) VIII Edition, European Stroke Initiative, American Heart Association/American Stroke Association, and the most recent American College of Physicians guidelines are based on the studies of Dickmann et al and Boeer et al published in 1988 and 1991, respectively, and enrolling only 68 patients.2,30,60,61 Table 2 summarizes the recommendations provided by several practice guidelines. In February 2012 ACCP IX Edition guidelines were published. Compared with previous VIII Edition, new ACCP guidelines encloses the study of Orken et al 67 for pharmacological prophylaxis and take in account CLOTS I trial for mechanical prophylaxis.
Summary of Available Guidelines of VTE Prophylaxis in ICH a
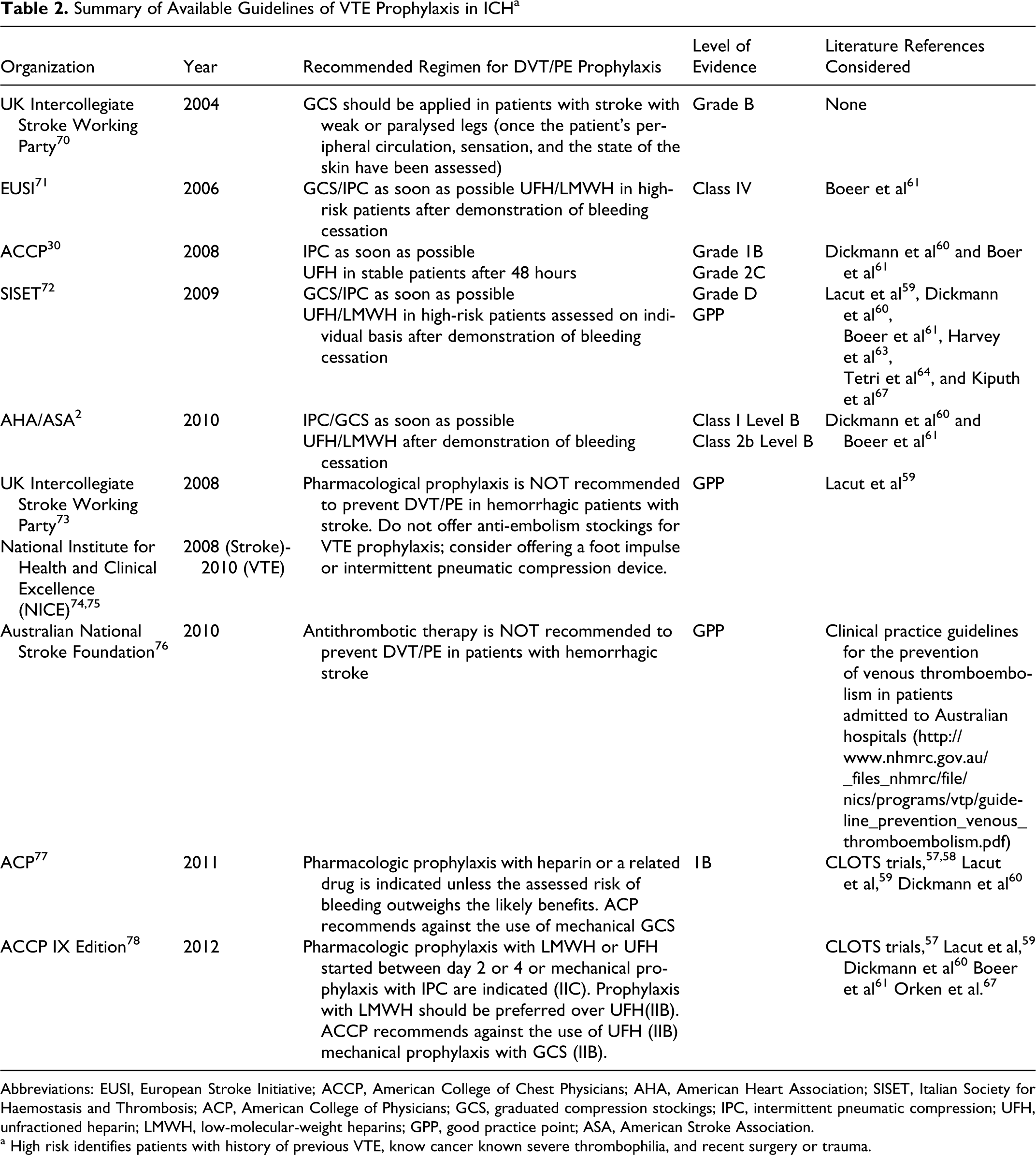
Abbreviations: EUSI, European Stroke Initiative; ACCP, American College of Chest Physicians; AHA, American Heart Association; SISET, Italian Society for Haemostasis and Thrombosis; ACP, American College of Physicians; GCS, graduated compression stockings; IPC, intermittent pneumatic compression; UFH, unfractioned heparin; LMWH, low-molecular-weight heparins; GPP, good practice point; ASA, American Stroke Association.
a High risk identifies patients with history of previous VTE, know cancer known severe thrombophilia, and recent surgery or trauma.
All guidelines available before 2011 substantially agreed on the role of mechanical prophylaxis in patients with sICH to prevent VTE and suggested to start their application as soon as possible. Guidelines published after 2010 agree to avoid GCS as the only one strategy for VTE prophylaxis. When mechanical prophylaxis is chosen, it should be based on IPC, alone or in combination with GCS. Of course, there is a greater caution when recommending pharmacological prophylaxis and this recommendation is not shared by all guidelines especially those published before 2011. In general, it is suggested to consider the use of pharmacological strategies for patients at high risk of VTE, but only when patient stabilization is documented and at least after 48 hours, which means after demonstration of bleeding cessation.
Conclusions
Literature evidences clearly show that the patients with nonsurgical sICH are at high risk of VTE. When VTE occurs, treatment strategies including the use of vena cava filters and therapeutic dose anticoagulant drugs expose patients to high risks of adverse events and may substantially modify patients’ outcomes in terms of morbidity and mortality. Therefore, it is crucial to provide patients with the best available prophylactic strategies (in terms of safety and efficacy) in order to avoid what is a highly preventable disease. Unfortunately, what are the optimal strategies for VTE prevention in this setting remain unclear. Pharmacologic prophylaxis may be necessary for some patients, but the optimal timing of initiation is unknown. The efficacy of combined mechanical prophylaxis also remains to be convincingly proven. Thus, randomized controlled trials are highly warranted.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article