
Abstract
Background:
Elevation of factor VIII is associated with higher risk of large vessel arterial occlusions including stroke.
Methods:
Factor VIII levels were examined in consecutive patients with acute ischemic stroke (AIS) presenting to a single center between July 2008 and May 2012. Factor VIII levels exceeding the laboratory reference range were considered elevated (>150%).
Results:
Factor VIII level was elevated in 72.4% (84 of 116) of the patients. Elevated factor VIII level was more frequent in blacks, diabetics, and patients who were anemic. Patients with elevated factor VIII had higher median baseline National Institute of Health Stroke Scale (NIHSS; 5 vs 2, P = .0295) and twice the frequency of neuroworsening (21.4% vs 9.4%), but discharge NIHSS and modified Rankin Scale were similar in the groups.
Conclusions:
High factor VIII level was found in the majority of tested patients with AIS. Several baseline differences were found between patients with normal and high factor VIII levels, but no differences were identified in outcome.
Keywords
Introduction
Factor VIII, a protein involved in the coagulation cascade, promotes the formation of thrombin and fibrin when activated. 1 Elevated levels of factor VIII have been associated with an increased risk of venous thromboembolism as well as recurrent thrombotic events, with the risk increasing as the factor VIII level increases. 2 –4 Previous work has shown higher factor VIII levels in association with many risk factors for stroke including, black race, diabetes, advancing age, higher body mass index, and non-O blood groups. 5 –8
Elevated factor VIII has been described in association with stroke secondary to cerebral venous thrombosis and paradoxical embolism from deep venous thrombosis. 9,10 Since mean factor VIII levels trend down over the course of treatment for venous thrombosis, 11 it could be argued that factor VIII may simply be an acute phase reactant. Previous work has described factor VIII as an acute phase reactant, a phenomenon likely mediated by interleukin 6, which upregulates factor VIII synthesis in times of inflammation. 12 However, persistently elevated levels have been documented even years after an event 13 and after adjusting for a known acute phase reactant (ie, C-reactive protein [CRP]), patients with venous thrombosis have higher factor VIII levels compared to healthy matched controls. 14
The Atherosclerosis Risk in Communities Study showed that factor VIII activity was elevated in patients who later developed coronary artery disease and ischemic stroke 15,16 ; the association with ischemic stroke was independent of other traditional vascular risk factors. 16 Additional studies have reported increased incidence of ischemic heart disease and mortality from cardiac events in patients with elevated factor VIII levels. 17,18 Despite previous work on heart disease and factor VIII, very little has been reported regarding factor VIII levels in the acute phase of ischemic stroke.
The purpose of this study was to investigate the relationship between factor VIII and acute ischemic stroke (AIS). We aimed to identify patient characteristics associated with elevated factor VIII levels in the acute phase of stroke and determine whether elevated factor VIII levels were associated with stroke severity, stroke etiology, or early outcomes. We hypothesized that elevated factor VIII levels would be associated with other markers of inflammation, disease severity, and worse functional outcomes.
Methods
We retrospectively evaluated factor VIII levels in patients who presented to our center between July 2008 and June 2012. Data were collected by trained abstractors, blinded to factor VIII level, via chart review. Patients were identified from our prospective stroke registry and included in the study if they were patients with AIS, 18 years of age or older, and admitted to the stroke service. Patients were excluded if thrombolytic (ie, intravenous tissue plasminogen activator) was administered. Serial neurologic evaluations were performed by a member of the Stroke Program or a neurology resident. Following the initial assessment, patients underwent computed tomography scan and other imaging studies as needed. Laboratory evaluation for possible underlying hypercoagulable state was ordered at the discretion of the treating physician, typically as part of a panel screening for arterial hypercoagulable conditions (eg, antiphospholipid antibodies, lupus anticoagulant, homocysteine, and factor VIII) in patients whom, after routine vascular and cardiac imaging, would otherwise have cryptogenic etiology. In our center, factor VIII level is included in a panel of labs devised to assess for causes of arterial hypercoagulability. This panel is routinely checked in patients with ischemic stroke who are considered young (<55 years old) and have a paucity of traditional vascular risk factors, recurrent stroke despite adherence to a secondary stroke prevention regimen, or prior history of unprovoked deep venous thrombosis, since this sample is more likely to have an underlying hypercoagulable state.
Patients were divided into 2 groups, those with normal factor VIII levels (50%-150%) and those with elevated (>150%) factor VIII levels, as levels exceeding 150% are found in the upper 10% of healthy blood donors and are associated with significantly increased risk of thrombotic events. 3 Baseline patient demographic and laboratory data were compared between the 2 groups. Subgroup analysis of patients with severely elevated (>200%) factor VIII levels versus all other screened patients was also performed. Multiple outcome measures were examined, including admission and discharge National Institute of Health Stroke Scale (NIHSS), neurological worsening, functional outcome as measured by the discharge modified Rankin Scale (mRS) score, and discharge disposition. All NIHSS scores were determined by certified examiners. Neurological worsening was defined as an increase of 2 or more points in the NIHSS within a 24-hour period. 19 A mRS-certified vascular neurologist assigned mRS score and the stroke etiology using the Trial of ORG 10172 in Acute Stroke Treatment (TOAST) classification system. 20
Categorical data were compared using Pearson chi-square or Fisher exact test, where appropriate. Continuous data were compared using independent samples t test or Wilcoxon rank-sum test, where appropriate. Pearson correlations were performed to evaluate the relationship between factor VIII as a continuous variable and outcome measures. Logistic and linear regression were used to assess the relationship between elevated factor VIII and discharge NIHSS, mRS, disposition, and length of stay (LOS), adjusting for variables that were significantly different on univariate analysis and/or previously shown to impact outcome. As this was an exploratory analysis, no adjustments were made for multiple comparisons. 21 This study was approved by our institutional review board.
Results
A total of 1045 patients with AIS were screened during the study period. In all, 116 (11%) patients had a factor VIII level measured in the acute period (mean age 53 years, 69% black, 56% female). Factor VIII levels were elevated in 84 (72%) patients. Baseline patient characteristics of the patients with normal and elevated factor VIII levels are shown in Table 1. Elevated factor VIII levels were more frequent in blacks (72.6% vs 53.1%, odds ratio [OR] 1.9, 95% confidence interval [CI] 0.995-3.572, P = .049) when compared to other races and in patients with a history of diabetes (38.1% vs 3.1%, OR 2.7, 95% CI 1.23-5.85, P < .0001) when compared to those without diabetes. Patients with elevated factor VIII levels had significantly lower admission hematocrit values (38.1% vs 41.1%, P = .040) and higher median erythrocyte sedimentation rate (ESR; 21 vs 14, P = .014) than patients with normal factor VIII levels. The median NIHSS in the normal factor VIII group was significantly lower than that of the elevated factor VIII group (2 vs 5, P = .0295). Baseline NIHSS correlated with baseline factor VIII level (r = .207, P = .0266).
Baseline Characteristics of Patients With and Without Elevated Factor VIII Levels.
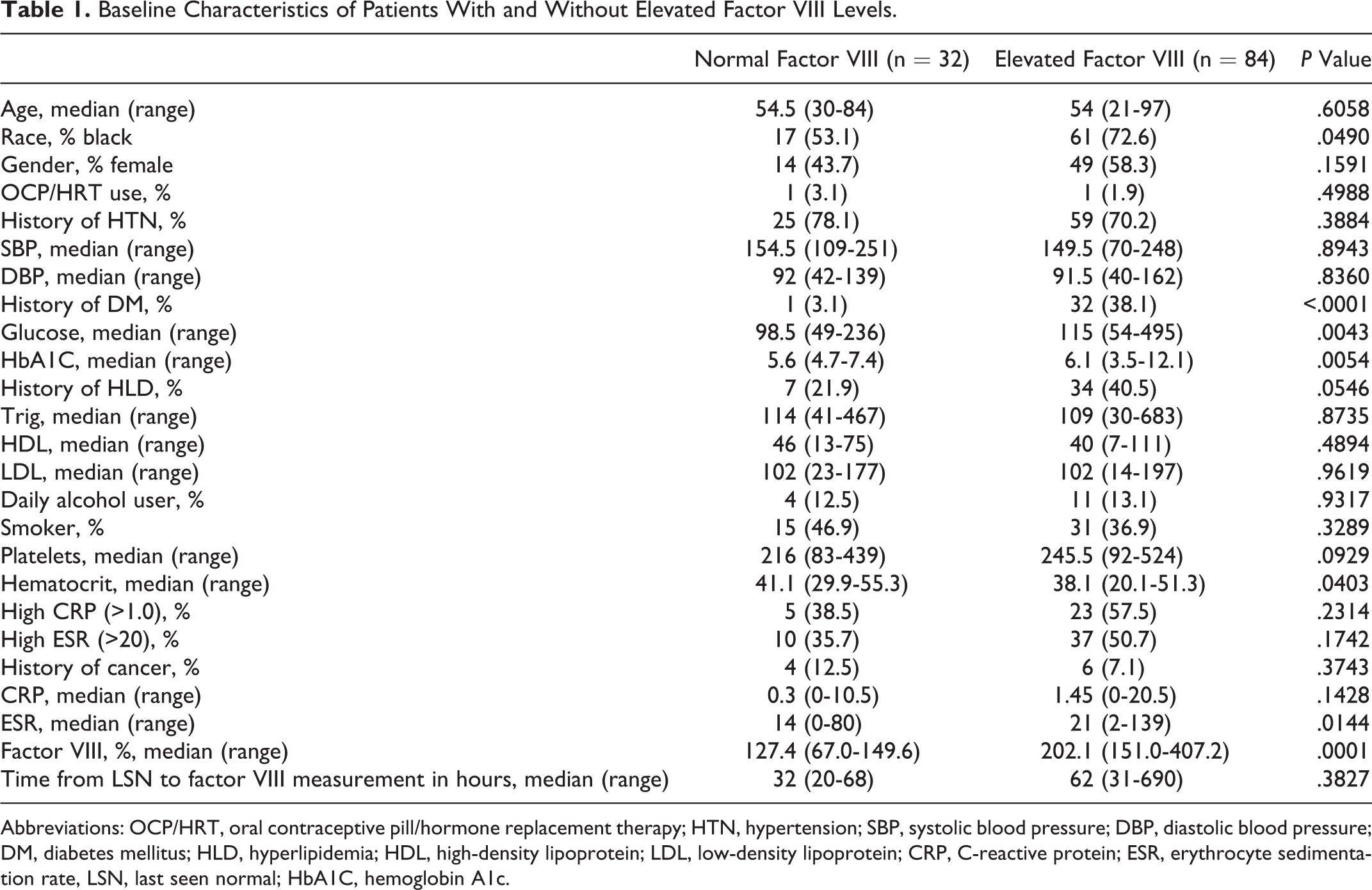
Abbreviations: OCP/HRT, oral contraceptive pill/hormone replacement therapy; HTN, hypertension; SBP, systolic blood pressure; DBP, diastolic blood pressure; DM, diabetes mellitus; HLD, hyperlipidemia; HDL, high-density lipoprotein; LDL, low-density lipoprotein; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate, LSN, last seen normal; HbA1C, hemoglobin A1c.
Hypercoagulation panels were ordered at the discretion of the treatment team. No diurnal relationship was found comparing median factor VIII levels with the time of day when blood was drawn. The median time from last seen normal (LSN) to factor VIII measurement for people with normal factor VIII levels was 32 hours (range 20-68 hours) and for those with elevated factor VIII was 62 hours (range 31-690 hours). The relationships between LSN time and factor VIII level were evaluated using Pearson correlations. Lower factor VIII levels were associated with increased LSN time in patients with normal factor VIII levels (r = −.652, P = .01); this relationship was observed in all the patients (r = −.419, P = .066) and in patients with elevated factor VIII levels (r = −.404, p = .369), although this was not statistically significant.
In univariate subgroup analysis, comparing patients with severely elevated (>200%) factor VIII to all others, the associations between black race, admission glucose, and median hemoglobin A1c with factor VIII group were no longer significant (data not shown). History of diabetes (40.9% vs 20.8%, P = .020), lower admission hematocrit (36.2% vs 40.1%, P = .030), and higher ESR (22 vs 17, P = .031) were still found with increased frequency among patients with severely elevated factor VIII.
Clinical course and outcome were compared among patients with normal and elevated factor VIII levels (Table 2). Baseline stroke severity (NIHSS) was significantly higher in patients with elevated factor VIII (5 vs 2, P = .030). Median factor VIII levels differed by etiology, with highest levels in patients with cardioembolic events. Median discharge NIHSS, mRS, and LOS were similar in patients with normal and elevated factor VIII levels. When comparing patients with severely elevated factor VIII levels to all others, there was no longer a significantly higher median baseline NIHSS (5 vs 4, P = .139), but the proportion of patients with neuroworsening was significantly higher (34.1% vs 8.3%, P = .0005), median neurologic deficits at discharge were greater (NIHSS 3 vs 2, P = .014), median functional outcome at discharge was worse (mRS 3 vs 2, P = .080), and median LOS was prolonged (7.5 vs 4.5, P = .0004).
Outcomes in Patients With Normal and Elevated Admission Factor VIII Levels.
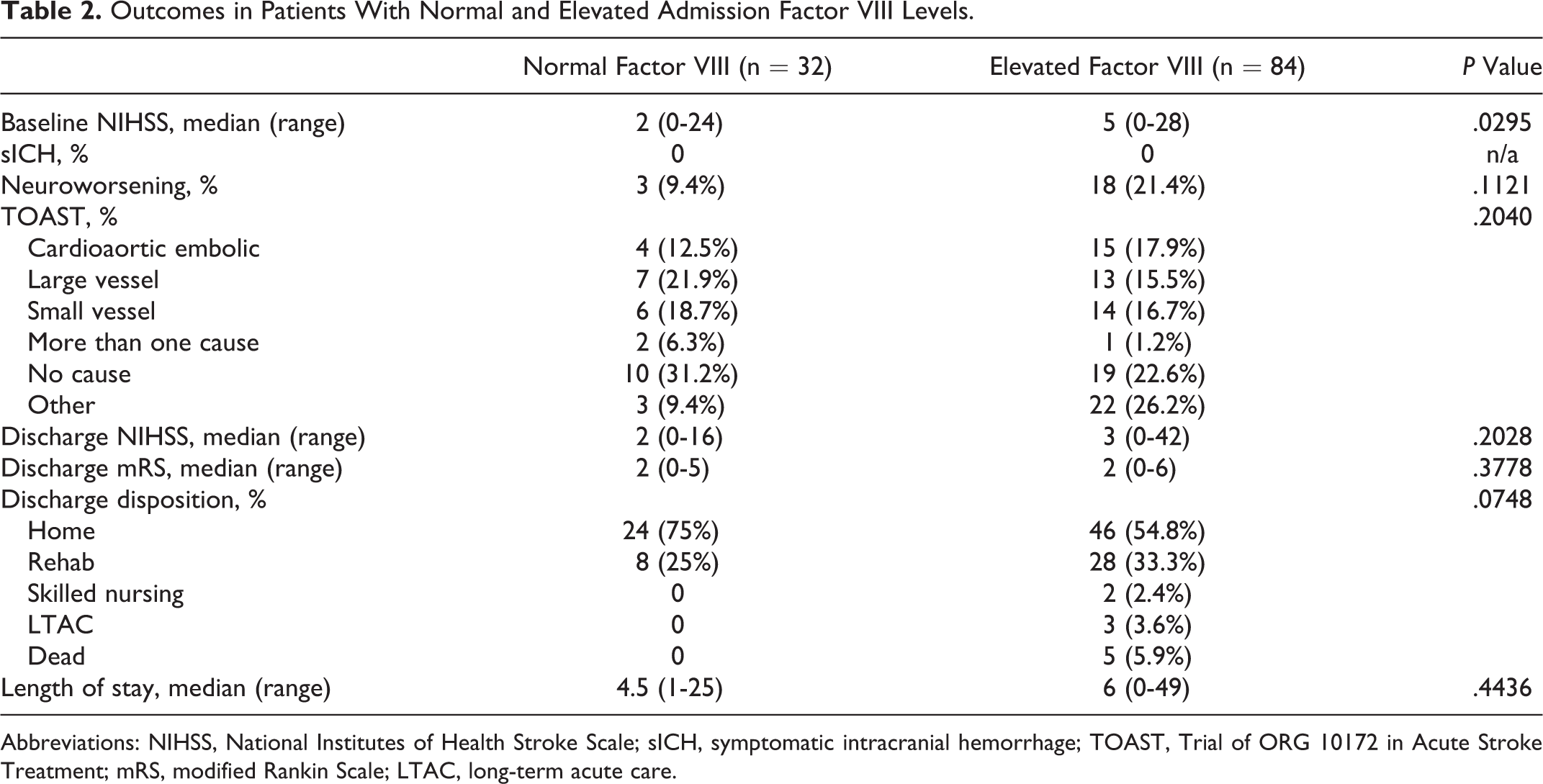
Abbreviations: NIHSS, National Institutes of Health Stroke Scale; sICH, symptomatic intracranial hemorrhage; TOAST, Trial of ORG 10172 in Acute Stroke Treatment; mRS, modified Rankin Scale; LTAC, long-term acute care.
Measured factor VIII level was positively correlated with occurrences of neuroworsening (r = .325, P = .0004) and LOS (r = .352, P = .0001); mRS did not reach significance (r = .177, P = .060). Measured factor VIII level was negatively correlated with good discharge disposition (r = −.190, P = .004). We did not find an association between factor VIII level and death. After adjusting for age, black race, history of diabetes mellitus, and baseline NIHSS, factor VIII level was not a significant-independent predictor of neuroworsening or discharge outcomes.
Discussion
To the best of our knowledge, this is the first study to explore the relationships between peristroke factor VIII levels and patient characteristics and outcomes in the acute phase of ischemic stroke. In our population, elevated factor VIII level was far more common than that previously reported in healthy blood donors 3 and was associated with black race, history of diabetes, anemia, and elevation in other acute phase reactants. Factor VIII has been demonstrated to be previously associated with a small, but significant, increased risk of having stroke, with a stronger association in blacks than whites. 16 When we compared patients with severely elevated (>200%) factor VIII levels to all others, we found no difference in the proportion of patients who were black, suggesting that most elevated factor VIII levels among blacks are in the moderate range (150%-200%).
We did find a higher frequency of diabetes and worse glycemic control (acute and over past 90 days) in patients with elevated VIII when dichotomized at 150%. The association of glycemic control did not remain when dichotomizing at 200%, suggesting the relationship was driven by those with moderately elevated factor VIII levels.
Patients with elevated factor VIII were more likely to have elevated ESR and/or CRP, suggesting that factor VIII may be an acute phase reactant in the setting of AIS. Since we did not have measurements of each patient’s factor VIII level before the stroke, we could not determine whether the elevations that we observed in factor VIII were present prior to the acute event. Further, since we did not have serial measurements after the stroke, we were unable to determine whether the levels were simply elevated in the acute setting. Even if transient and representative of an acute phase reactant, increased circulating factor VIII could predispose patients to greater thrombus formation.
We found that patients with normal factor VIII levels had shorter LSN times than patients with elevated levels. The significance of this finding is unclear at this time. Lower factor VIII levels were associated with increasing time since the event, particularly in patients with normal levels. In the event that patients with normal factor VIII levels had their level drawn later, we could expect that levels might be even lower. The fact that the patients with elevated factor VIII had delayed assessment of levels suggests that if levels are dynamic, the levels might have been even higher if sampled earlier. This finding highlights the need for additional investigation of serial factor VIII levels after stroke onset.
We did find a relationship between elevated factor VIII and baseline stroke severity. The positive correlation between baseline NIHSS and baseline factor VIII level suggests that levels might have been even higher if the sample included a larger proportion of patients with more severe strokes. Despite this, elevated factor VIII was not independently associated with any of our outcome measures after adjusting for important baseline variables, including NIHSS on admission.
This study is limited by its cross-sectional design, single measurement of factor VIII, and relatively small sample size. It was not possible to have factor VIII levels prior to stroke onset, but preliminary analysis of the subset who have returned for follow-up testing (median of 110 days later) found that two-thirds have persistently elevated factor VIII levels, which could be predicted by higher factor VIII level at the time of stroke. Testing of factor VIII was not random or universal, raising concern for selection bias and limiting generalizablility of our findings to patients with AIS with hypercoagulable state as the suspected etiology. We report only our observations, as a single factor VIII measurement performed in the acute setting of ischemic stroke cannot distinguish preexisting elevated factor VIII levels associated with increased risk of vascular events 16 from factor VIII level elevation as an acute phase reactant. Prospective studies with serial measurements will be required to clarify these complex relationships.
Conclusions
In patients with ischemic stroke suspected of a hypercoagulable state, factor VIII was commonly found to be elevated during the acute period. Although some patient characteristics appear to be associated with factor VIII levels, we found no convincing evidence that factor VIII levels in the acute period influence the early outcomes after stroke. More research is required to determine whether high factor VIII levels actively contribute to thrombosis or are a consequence of an ischemic event. A better understanding of the role and temporal relationship of factor VIII in AIS and utility of acute factor VIII levels could serve to guide and individualize treatment for patients with ischemic stroke in the future.
Footnotes
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the Agency for Healthcare Research and Quality (AHRQ) or the National Institutes of Health (NIH).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project described was supported by Award Numbers 5 T32 HS013852-10 from The Agency for Healthcare Research and Quality (AHRQ) and 3 P60 MD000502-08S1 from The National Institute on Minority Health and Health Disparities (NIMHD) and National Institutes of Health (NIH).