
Abstract
Patients with prior stroke are susceptible to venous thromboembolism (VTE). We studied patients with stroke in the Worcester VTE study of 2488 consecutive patients hospitalized with VTE. In all, 288 (11.6%) had a clinical history of stroke and 2200 (88.4%) did not. Patients with stroke were more likely to die inhospital (9.2% vs 4%) and within 30 days of VTE diagnosis (16.7% vs 6.9%) compared with patients without stroke (all P < .001). Recent immobilization (adjusted odds ratio [OR] 2.15; 95% confidence interval [CI] 1.15-4.09) and inferior vena cava (IVC) filter insertion (adjusted OR 2.1; 95% CI 1.15-3.83) were associated with a doubling of inhospital death. Recent immobilization (adjusted OR 1.84; 95% CI 1.19-2.83) and IVC filter insertion (adjusted OR 1.94; 95% CI 1.2-3.14) were associated with an increased risk of death within 30 days of VTE. In conclusion, patients with VTE and prior stroke were more than twice as likely to die while hospitalized and within 30 days of VTE diagnosis.
Venous thromboembolism (VTE), including deep vein thrombosis and pulmonary embolism, is a common and potentially preventable complication of medical illnesses resulting in immobility such as stroke. 1 –3 The frequency of proximal deep vein thrombosis was 10% among 2518 rehabilitation patients initially hospitalized with acute stroke and randomized to thigh-length graduated compression stockings versus routine care. 2 VTE coexists frequently with atherosclerotic cardiovascular disease, including stroke and myocardial infarction. 4 –7 VTE shares common risk factors with atherosclerotic cardiovascular disease such as obesity, smoking, hypertension, dyslipidemia, and diabetes. 8,9 Furthermore, VTE shares key pathophysiological pathways of inflammation, 10,11 hypercoagulability, 9,12 and endothelial dysfunction 13,14 with atherosclerotic cardiovascular disease.
There is a paucity of data regarding the outcomes of patients with prior stroke and concomitant VTE. Using data from the Worcester VTE Study, a population-based study of central Massachusetts residents with independently confirmed VTE, we examined the clinical characteristics, use of prophylaxis, treatment strategies, and short-term outcomes of 283 patients with VTE and previously diagnosed stroke and 2200 patients with VTE without prior stroke.
Methods
Patient Population
Lists of patients eligible for entry into the registry were generated from health care system encounters in which any of 34 International Classification of Diseases, Ninth Revision diagnosis codes consistent with VTE were used in 1999, 2001, 2003, and 2005. 15 These lists were obtained from 11 medical centers serving residents of the Worcester, Massachusetts metropolitan area. 15 Institutional review board approval was obtained at all 11 study sites. Data queries included discharge diagnoses and outpatient, Emergency Department, radiology, and laboratory clinical encounters. The medical records of all potentially eligible patients were reviewed by dedicated nurse abstractors using prespecified criteria to validate and characterize each case of suspected VTE. 15
Each potential case of deep vein thrombosis or pulmonary embolism was independently validated by the study project coordinator and classified as being either definite, probable, possible, or negative, based on a modification of the classification used by Silverstein et al. 16,17 Deep vein thrombosis was defined as definite if confirmed by venography, compression ultrasonography, computed tomography, magnetic resonance imaging, or autopsy; probable if the above tests were not performed or were indeterminate, but impedance plethysmography, radionuclide venography, or radiolabeled fibrinogen scan test results were reported as positive; and possible if these confirmatory tests were not performed or were indeterminate, and 2 of the following criteria were satisfied: the medical record indicated that the physician made a clinical diagnosis of deep vein thrombosis, symptoms or signs of deep vein thrombosis were documented, and the patient underwent therapy with anticoagulants or inferior vena cava (IVC) filter insertion. Pulmonary embolism was defined as definite if confirmed by pulmonary angiography, spiral chest computed tomography, magnetic resonance imaging, or autopsy; probable if the tests above were not performed or were indeterminate, but ventilation-perfusion lung scan findings were high probability; and possible if all of the above confirmatory tests were not performed or were indeterminate, and 2 of the following criteria were satisfied: the medical record indicated that the physician made a clinical diagnosis of pulmonary embolism, symptoms or signs of pulmonary embolism were documented, and the patient underwent therapy with anticoagulants or IVC filter insertion. These criteria were modified from those previously utilized by Silverstein et al in the Olmstead County study of VTE. 16 Given increasing acceptance over the last decade of compression ultrasonography as a single diagnostic modality for deep vein thrombosis, we classified patients with deep vein thrombosis confirmed by compression ultrasonography as definite, whereas these patients would have been categorized as probable by Silverstein criteria. If classification of VTE was not immediately clear using the specified criteria, the principal investigator (FAS) reviewed the medical record. Only definite, probable, and possible cases were included in the current analysis. There were no exclusion criteria for entry into the registry.
Incident cases of VTE were defined as those occurring in individuals without a prior history of deep vein thrombosis or pulmonary embolism. Recurrent VTE was defined as a new occurrence of thrombosis in a previously uninvolved vein or pulmonary artery as detected by an imaging study. Provoked VTE was defined as a venous thromboembolic event that occurred within 3 months of hospitalization, major surgery, major trauma, immobilization, pregnancy, malignancy, central venous catheter placement, or hormonal contraceptive or replacement therapy use.
Patients with any current or prior history of clinical diagnosis of stroke, cerebrovascular accident, or cerebrovascular hemorrhage were identified based on the information contained inhospital and ambulatory care records and were classified as having prior stroke.
Data Collection
Data regarding demographic characteristics, comorbidities, risk factors, diagnosis, management, prior prophylaxis utilization, and outcomes were abstracted from inpatient and outpatient medical records. Surgery was defined as a major operation where general or epidural anesthesia lasted 30 minutes or longer. Immobility was defined as limited ambulation, restricted activity of bed-to-chair or bed-to-bathroom, or complete bed rest based on the medical record documentation. Clinical characteristics were defined as “recent” if occurring or active within 3 months prior to the diagnosis of VTE.
Major bleeding for study years 1999, 2001, and 2003 was defined as any episode of bleeding requiring transfusion or resulting in hospitalization (or prolongation of hospitalization), stroke, myocardial infarction, or death. To be consistent with International Society of Thrombosis and Hemostasis criteria, 18 the definition was revised for the 2005 patient cohort. Major bleeding was defined as clinically overt bleeding that (1) resulted in death, (2) was at a critical site (intracranial, intraocular, retroperitoneal, intra-articular, pericardial, muscular with compartment syndrome, (3) required transfusion of at least 2 units of packed red blood cells, or (4) resulted in a hemoglobin decrease of at least 20 g/L.
Data regarding thromboprophylaxis utilization were obtained for patients hospitalized with any non-VTE-related disorder or for major surgery within 3 months prior to the diagnosis of deep vein thrombosis or pulmonary embolism. This information was abstracted from medical records at the same time as data regarding the incident VTE event. Medical records from other area hospitals were reviewed in case prior hospitalization was at an institution other than that of the index VTE. First recurrence of VTE or a major bleeding event was determined through review of medical records at the same hospital as the index event and screening of medical records from the other participating medical centers. Data regarding all-cause mortality were obtained through review of hospital records and death certificates at the Massachusetts Division of Vital Statistics. Median follow-up for long-term outcomes was 989 days.
Statistical Methods
Means, medians, and frequency distributions were calculated for continuous variables. Differences in the distribution of demographic characteristics, comorbidities, risk factors, diagnosis, management strategies, prophylaxis, and outcomes between patients with and without prior stroke were examined using the chi-square or Fisher exact test for categorical variables and t test for continuous variables. Cumulative incidence rates of VTE recurrence, major bleeding, and all-cause mortality were estimated using the life table method. Differences in the frequency of these end points were compared between patients with and without diabetes using the log-rank test. All statistical tests were 2-tailed, and a P value of less than .05 was considered to be statistically significant.
Cox regression analysis was utilized to evaluate whether a clinical diagnosis of stroke was associated with an increased risk of inhospital death and death within 30 days of VTE diagnosis, while controlling for several potentially confounding prognostic factors. Variables included in the regression model for these outcomes were selected based on the results of univariate analysis and a priori knowledge and included age, sex, body mass index, medical history (history of diabetes, heart failure, indwelling central venous catheter, ischemic heart disease, stroke, and chronic kidney disease), recent immobility, intensive care unit discharge within the prior 3 months, admission for non-VTE-related indication, treatment of VTE with antithrombotic therapy, and IVC filter insertion. All statistical analyses were performed using SAS version 9.2 (SAS Institute Inc, Cary, North Carolina).
Results
Baseline Characteristics
Of 2488 consecutive patients hospitalized with VTE, 288 (11.6%) had a clinical history of stroke and 2200 (88.4%) did not. Patients with VTE and prior stroke were older than patients with VTE without previous stroke (mean age 73 vs 62.6 years, P < .001; Table 1). Patients with VTE and prior stroke were leaner than those without stroke (26.5 vs 28.9 kg/m2, P < .001). Patients with prior stroke were more likely to have developed VTE during hospitalization for a non-VTE-related condition (44.2% vs 26.1%, P < .001). Patients with VTE and prior stroke had a longer mean duration of hospitalization than those without stroke (14.3 vs 10 days, P = .03).
Baseline Characteristics of Patients With Venous Thromboembolism.
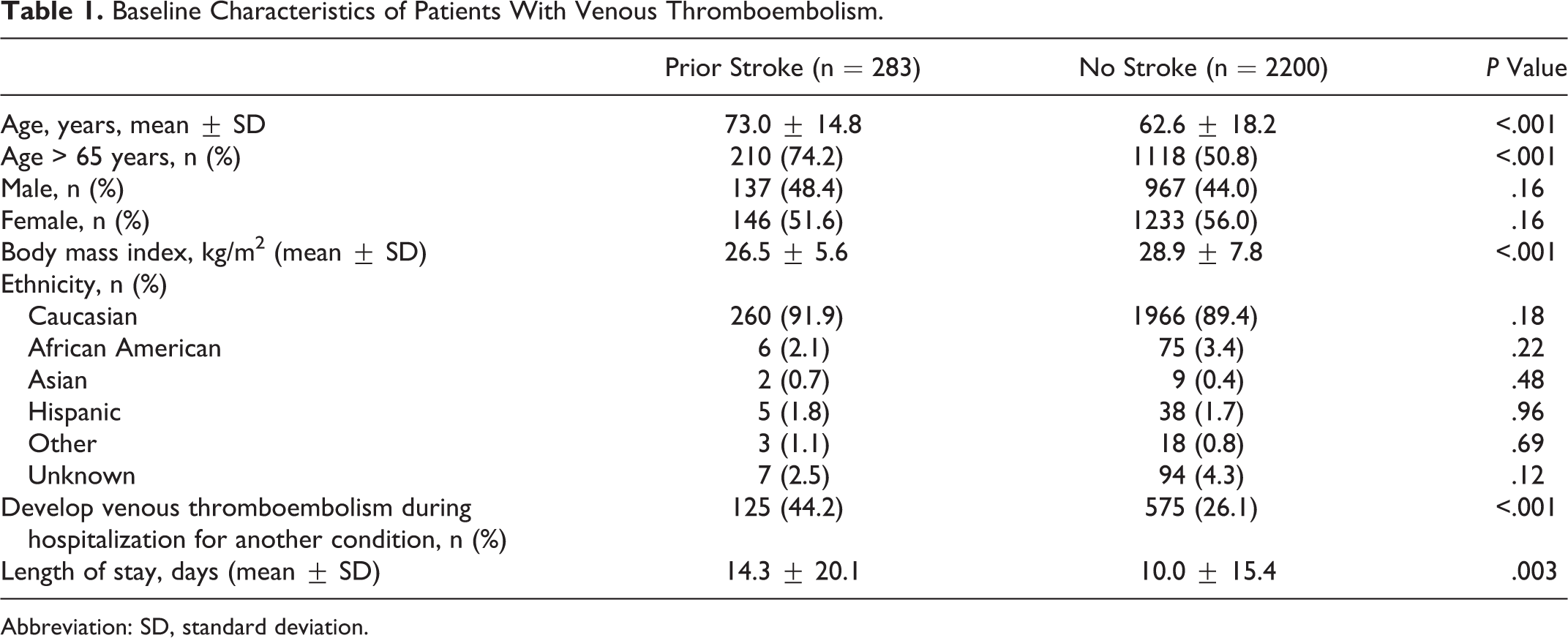
Abbreviation: SD, standard deviation.
Comorbidities and Risk Factors
Patients with acute VTE and prior stroke were more likely to have comorbid conditions of recent immobility greater than 48 hours, recent acute infectious illness, heart failure, diabetes, ischemic heart disease, peripheral artery disease, and chronic kidney disease than patients without stroke (Table 2). Patients with prior stroke were also more likely to have an indwelling central venous catheter than those without stroke (23.3% vs 17.9%, P = .03). Patients with prior stroke were twice as likely to have been discharged from the intensive care unit within the 3 months prior to VTE diagnosis than patients without stroke (29% vs 14.7%, P < .001).
Comorbid Conditions in Patients With Venous Thromboembolism.
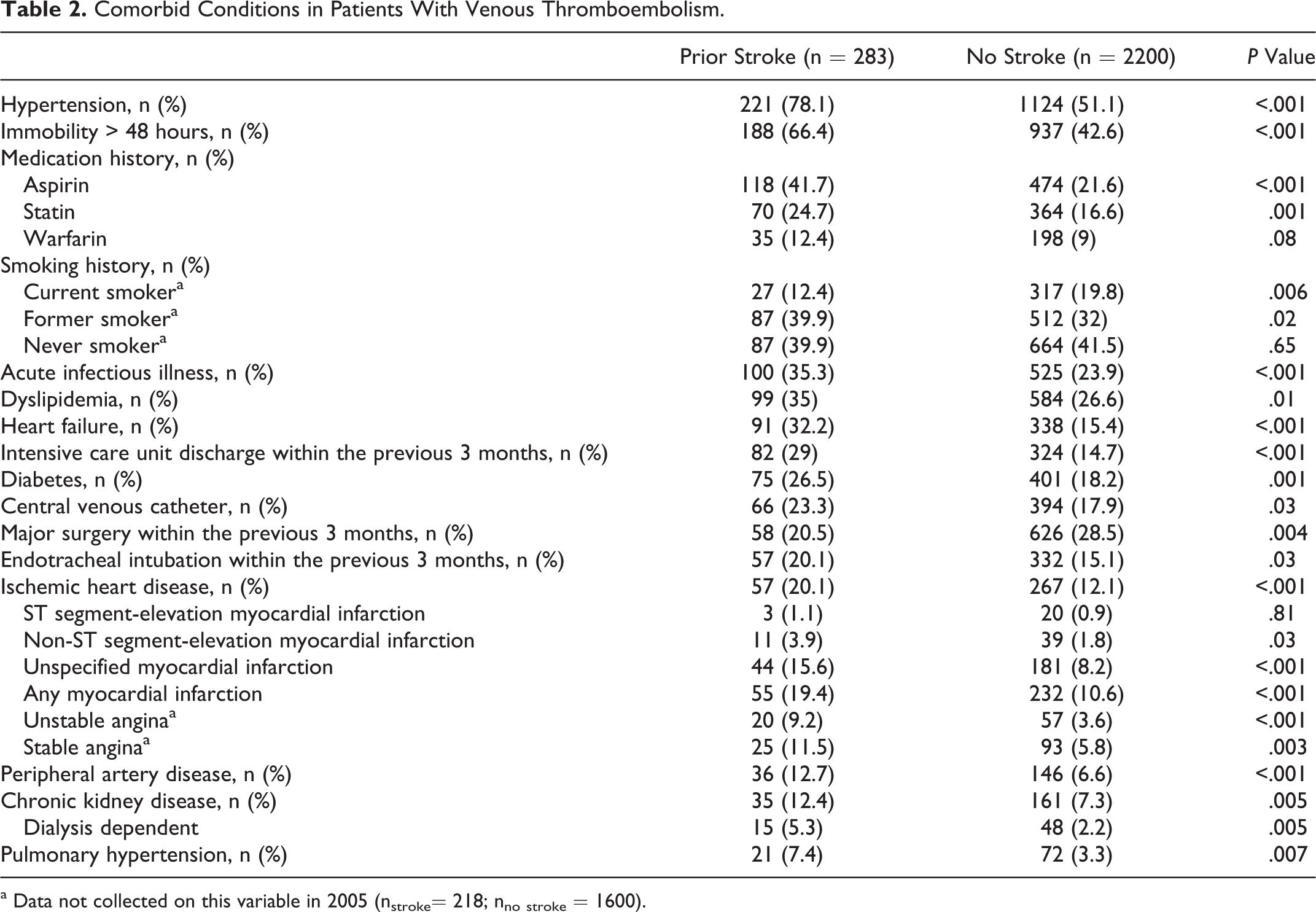
a Data not collected on this variable in 2005 (nstroke= 218; nno stroke = 1600).
Clinical Presentation of VTE
Patients with VTE and prior stroke were less likely to present with symptoms referable to either deep vein thrombosis or pulmonary embolism than patients without previous stroke (Table 3). Patients with prior stroke were more likely to present with any deep vein thrombosis, proximal deep vein thrombosis without concomitant calf vein involvement, and concomitant proximal and calf deep vein thrombosis. Patients with VTE and prior stroke were less likely to have isolated calf deep vein thrombosis than patients without stroke (3.9% vs 8.3%, P = .005). Patients with prior stroke were more likely to have had provoked VTE than those without stroke (85.2% vs 73.5%, P < .001).
Clinical Presentation of Venous Thromboembolism.

Abbreviation: VTE, venous thromboembolism.
Prophylaxis of VTE
Patients with prior stroke who were hospitalized for any non-VTE-related condition or had major surgery within 3 months prior to diagnosis of deep vein thrombosis or pulmonary embolism were more likely to have received thromboprophylactic measures than patients without stroke (67.2% vs 46.9%, P < .001; Table 4). Patients with VTE and prior stroke were also more likely to have received pneumatic compression devices or intravenous unfractionated heparin for thromboprophylaxis.
Characteristics of Thromboprophylaxis in Patients With Hospitalization or Major Surgery Within 3 Months of Subsequently Developing Venous Thromboembolism.a
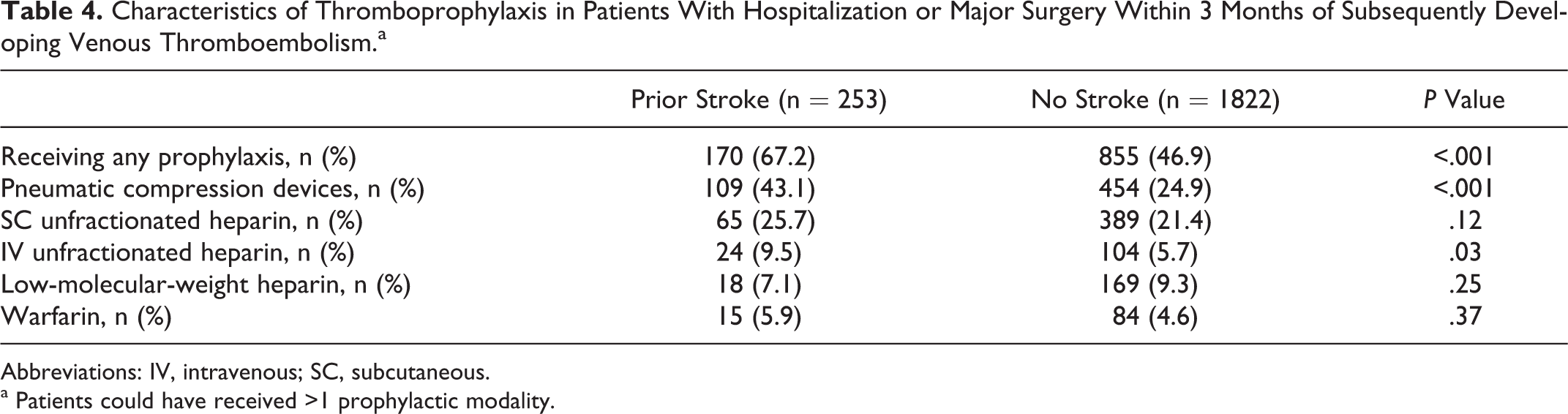
Abbreviations: IV, intravenous; SC, subcutaneous.
a Patients could have received >1 prophylactic modality.
Treatment of VTE
Intravenous unfractionated heparin was the most commonly used parenteral anticoagulant in the initial treatment of VTE in patients with prior stroke, while low-molecular-weight heparin was most frequently used in those without stroke (Table 5). Patients with VTE and prior stroke were less likely to be prescribed low-molecular-weight heparin as a bridge to therapeutic anticoagulation with warfarin at discharge. Patients with VTE and prior stroke were more likely to have been discharged without warfarin therapy, low-molecular-weight heparin as a “bridge” to anticoagulation with warfarin, or low-molecular-weight heparin monotherapy (27.6% vs 18.5%, P < .001). The IVC filter insertion was more common among patients with VTE and prior stroke than those without prior stroke (22.3% vs 10.5%, P < .001).
Therapy in Patients With Venous Thromboembolism.a
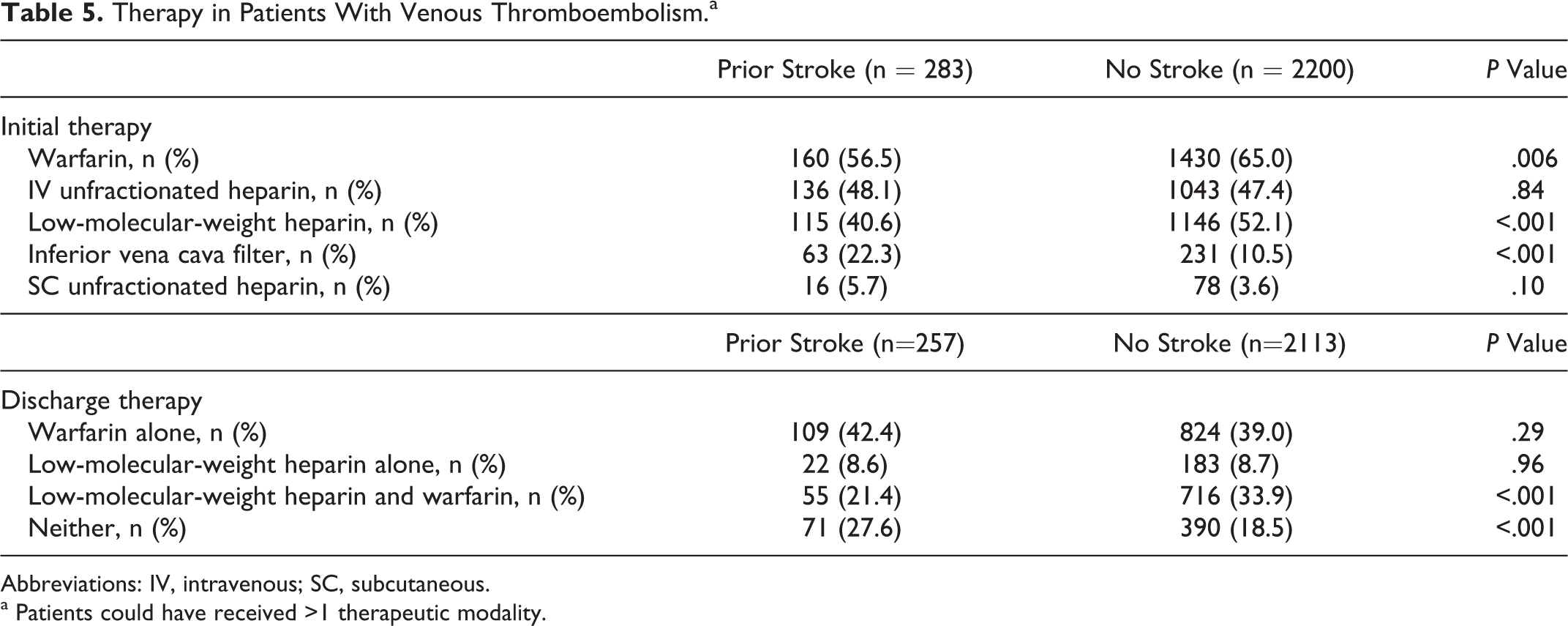
Abbreviations: IV, intravenous; SC, subcutaneous.
a Patients could have received >1 therapeutic modality.
Outcomes
After VTE, patients with prior stroke were more likely to have a complicated course than patients without stroke (Table 6). Although we observed no difference in inhospital or long-term bleeding, patients with VTE with prior stroke were more likely to have inhospital death (9.2% vs 4%) and death within 30 days of VTE diagnosis (16.7% vs 6.9%; all P < .001). After adjusting for several potentially confounding prognostic variables, only a history of recent immobilization (adjusted odds ratio [OR] 2.15; 95% confidence interval [CI] 1.15-4.02), heart failure (adjusted OR 1.91; 95% CI 1.07-3.41), admission for non-VTE-related indication (adjusted OR 2.23; 95% CI 1.26-3.96), and IVC filter insertion (adjusted OR 2.1; 95% CI 1.26-3.96) were associated with a significant increase in the risk of inhospital death. Recent immobilization (adjusted OR 1.84; 95% CI 1.19-2.83), admission for non-VTE-related indication (adjusted OR 1.86; 95% CI 1.23-2.83), and IVC filter insertion (adjusted OR 1.94; 95% CI 1.2-3.14) were associated with a significant increase in the risk of death within 30 days of VTE. Treatment with antithrombotic therapy after diagnosis of VTE was significantly associated with a reduction in 30-day mortality (adjusted OR 0.53; 95% CI 0.31-0.9).
Outcomes of Patients With Venous Thromboembolism.
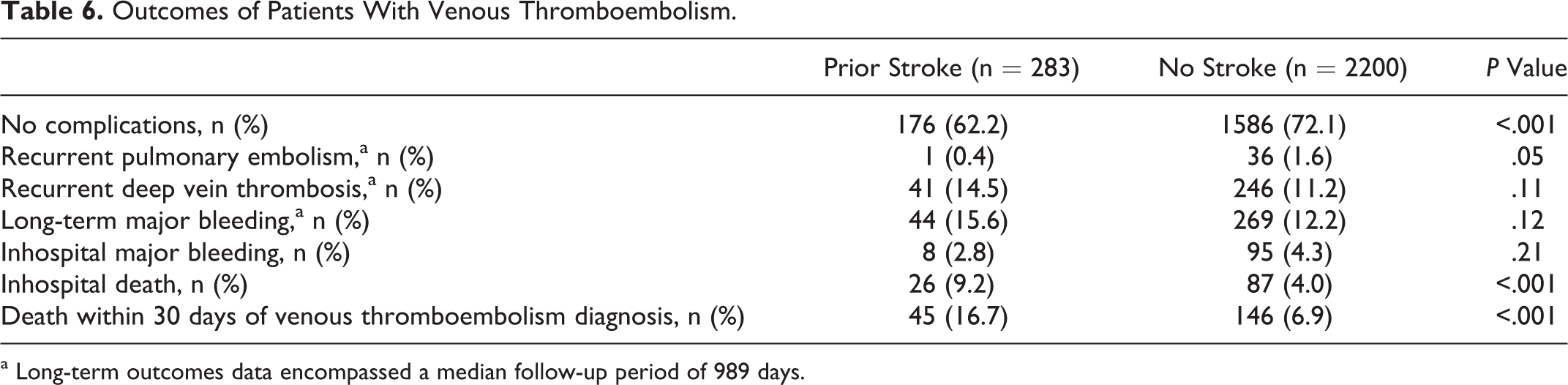
a Long-term outcomes data encompassed a median follow-up period of 989 days.
Discussion
Patients with VTE who had prior stroke were more than twice as likely to die while hospitalized and within 30 days of VTE diagnosis compared to patients with VTE without stroke. Immobility, a comorbidity common in the stroke population, was associated with a doubling in the risk of inhospital death and death within 30 days of VTE diagnosis. The IVC filters were inserted more than twice as frequently among patients with VTE with prior stroke.
Based on our analysis, patients who develop acute VTE with prior history of stroke represent a vulnerable population at particularly increased risk of a complicated clinical course after the diagnosis of VTE. patients with VTE and prior stroke were more than twice as likely to have inhospital death and death within 30 days of VTE diagnosis. In multivariate analyses, prior stroke was not independently associated with an increase in death during hospitalization and death within 30 days of VTE diagnosis. Although atherosclerotic cardiovascular disease is associated with a greater frequency of deep vein thrombosis and pulmonary embolism, 4,5 a reciprocal relationship exists in which VTE increases the risk of potentially fatal cardiovascular events such as myocardial infarction 7 and stroke. 6 Patients with prior stroke who subsequently develop VTE also have a higher frequency of comorbid conditions such as heart failure and chronic kidney disease that may further contribute to overall greater medical frailty and adverse outcomes. The increased risk of mortality following VTE highlights the importance of VTE prevention in the vulnerable stroke population. 19 –22
Immobility is ominous in patients with prior stroke and doubled the risk of inhospital death and death within 30 days of VTE diagnosis. Immobility has been previously demonstrated to be a potent independent predictor of mortality in other high-risk medical patient populations, including those with heart failure and chronic obstructive pulmonary disease. 23,24 Neurological deficits following stroke frequently contribute to immobility and predispose to numerous complications such as VTE. 25 Quality improvement initiatives emphasizing early mobilization after stroke have the potential to reduce immobility-associated medical complications such as VTE in this vulnerable population. 26
Patients with prior stroke who subsequently developed VTE were more than twice as likely to receive an IVC filter as those without stroke. Concerns about the risk of hemorrhagic conversion after ischemic stroke or extension of hemorrhage in patients with hemorrhagic stroke may have resulted in greater reliance on IVC filters in lieu of therapeutic anticoagulation. Despite increasing utilization of both permanent and retrievable IVC filters in the United States, 27 there is little evidence to suggest a reduction in all-cause mortality among patients receiving these devices. 28 We observed that IVC filters were associated with more than a doubling in death during hospitalization and within 30 days of VTE diagnosis. One explanation is that patients with stroke may have a higher frequency of IVC filter insertion because of comorbid conditions that preclude therapeutic anticoagulation. These comorbid conditions may also independently increase the risk of death following VTE.
The present findings should be interpreted in the context of our study design and patient population. The registry population was predominantly Caucasian, thereby limiting the ability to generalize our findings. Because neurological imaging studies were not required to identify patients with stroke, some patients without stroke may have been misclassified as having had prior stroke based on a clinical diagnosis. Furthermore, the registry did not distinguish between ischemic and hemorrhagic strokes and did not account for stroke severity (National Institutes of Health Stroke Scale), which has an important impact on outcomes such a mortality. 29 Patients with hemorrhagic stroke may be less likely to receive thromboprophylaxis or anticoagulation once diagnosed with VTE. We did not collect data regarding dose, frequency, or adequacy of thromboprophylaxis, different treatment regimens, or cause of death. As in any observational study, unrecognized confounding may be present despite extensive evaluation of patient characteristics. Confounding by indication may explain differences in outcomes observed with particular treatments, such as IVC filter insertion.
To our knowledge, our study represents one of the first registry analyses to evaluate the clinical characteristics, thromboprophylactic practices, treatments received, and outcomes in patients with stroke and concomitant VTE. The methodology is consistent with published criteria for evaluating the scientific value of clinical data registries. 30 Consecutive patients with objectively confirmed VTE from urban, suburban, and rural communities were enrolled and comprise a “real-world” population.
Conclusions
Patients with VTE and prior stroke were more than twice as likely to die while hospitalized and within 30 days of VTE diagnosis compared with patients with VTE without stroke. Immobility, a frequent and ominous sequela of stroke, was associated with a doubling in the risk of inhospital death and death within 30 days of VTE. The IVC filters were inserted more than twice as frequently among patients with VTE and prior stroke. Quality improvement initiatives should focus on reducing immobility and understanding the utilization of IVC filters in the vulnerable stroke population.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Spencer is supported by a Career Investigator Award from the Ontario Heart and Stroke Association.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant R01-HL70283 (PI: Spencer) from the National Heart, Lung, and Blood Institute.