
Abstract
Myocardial injury following carotid endarterectomy (CEA) is a common cause of morbidity and mortality, and its risk varies depending on the severity and extent of disease. However, when patients with sympotomatic severe carotid stenosis undergo CEA, the frequency and potential predictors of myocardial injury remain unknown. A total of 40 patients (32 men and 8 women) who underwent successful standard CEA were observed. Cardiac troponin I (cTnI) concentrations were assessed before surgery and on postoperative days 1, 2, and 3 in all patients. Myocardial injury was defined as the peak cTnI concentration > 0.04 ng/mL. In all, 42.5% patients had postoperative myocardial injury. Previous ischemic stroke and abnormal ST-segment changes were the preoperative predictors of myocardial injury after CEA, with odds ratios of 4.1 (95% confidence interval, 1.1-16.1; P = .04) and 5.9 (95% confidence interval, 1.3-27.7; P = .04), respectively. Sympotomatic patients with those conditions should receive more attention to myocardial injury, when presented for CEA.
Introduction
Carotid atheromatous disease is the result of atherosclerosis at the bifurcation of the common carotid artery or the origin of the internal carotid artery and considered as a manifestation of systemic atheromatous disease. Symptomatic carotid disease has been defined as a risk factor for coronary artery disease. 1 But in patients with carotid disease, the absolute risks of myocardial infarction and vascular death vary, depending on the severity and extent of disease. 2
Carotid endarterectomy (CEA) is performed to prevent ischemic stroke in patients with carotid atheromatous disease. The CEA has an inherent risk of perioperative stroke and cardiovascular events. Indeed, in addition to cerebrovascular accident, myocardial infarction is another major perioperative complication of CEA. 3 By the similar nature of disease pathogenesis, patients undergoing CEA are likely to have extensive atheromatous disease with significant risk of perioperative myocardial injury. However, the frequency and possible risk factors for myocardial injury in patients undergoing CEA with symptomatic severe carotid stenosis remain unknown, because there was no such study specifically addressing this issue.
Cardiac troponin I (cTnI), an intracellular protein involved in heart muscle contraction, is a highly sensitive and specific marker for cardiomyocyte damage. Previous study has demonstrated that cTnI is a reliable marker for myocardial injury that indicates myocardial ischemia in patients undergoing vascular surgery. 4 The normal range of cTnI is below 0.04 ng/mL in apparently healthy population. 5 Myocardial injury is indicated if the cTnI concentration is above 0.04 ng/mL. A diagnosis of myocardial infarction was considered with the cTnI value greater than 1.5 ng/mL and myocardial ischemia with the cTnI value of between 0.5 and 1.5 ng/mL. 4 It has been shown that routine surveillance for cardiac troponins can be useful in identifying patients without clinical evidence of myocardial ischemia who are at increased risk of perioperative myocardial infarction and death. 6
The aim of this prospective, observational study was to evaluate the frequency and potential risk factors for early ischemic myocardial injury in symptomatic patients undergoing unilateral standard CEA with severe atherosclerotic carotid artery stenosis.
Materials and Methods
Patients
The study was approved by the institutional review board. After signing informed written consent, 40 consecutive patients scheduled for unilateral standard CEA at XuanWu Hospital of Capital Medical University from May 2010 to March 2012 were prospectively studied. All patients had a sympotomatic carotid artery stenosis (>70% of the luminal diameter on color duplex ultrasonography). Exclusion criteria for the study included a history of disabling stroke, unstable angina, or myocardial infarction within the preceding 3 months, age less than 60 years, a permanent pacemaker, chronic renal failure, and other operations at the same time. Before surgery, clinical risk factors were noted, and echocardiography was performed for cardiac risk assessment. All medications for chronic cardiovascular therapy were continued until the day of surgery and resumed as soon as possible postoperatively.
Anesthesia
All procedures were performed by a single team of surgeons and anesthesiologists. The standard monitoring was used throughout the study, including invasive arterial blood pressure, 5-lead electrocardiography, heart rate, pulse oximetry, nasopharyngeal temperature, and bispectral index. In addition, an arterial pressure-based cardiac output monitor (FloTrac system; Edwards Lifescience LLC, Irvine, CA, USA) was used to assess cardiac function and transcranial Doppler to evaluate the cerebral blood flow and predict the shunt selection. All patients were placed in the horizontal supine position.
Standard general anesthesia with propofol and remifentanil was performed in all the patients. A bolus of 5000 U of heparin was given before clamping. Ephedrine, phenylephrine, or norepinephrine were given in case of stroke volume lower than 25 mL/beat, a decrease in ispilateral middle cerebral artery velocity (MCAV) of greater than 40% before declamping, or both. A shunt was selected after clamping when it was difficult to maintain the ispilateral MCAV above 60% of baseline. Urapidil were used when the increase in blood pressure exceeded 20% of the preoperative value or an increase in MCAV is greater than 150% of the baseline.
All intraoperative adverse events, including hypotension, hypertension, or arrhythmias, were recorded. Hypotension and hypertension were defined as a systolic arterial blood pressure below 80% or above 120% of baseline for more than 5 minutes, respectively. Arrhythmia was defined as a change in baseline cardiac rhythm requiring specific pharmacologic therapy.
Postoperative Management
After surgery, all patients were monitored for at least 1 night in the neurosurgery intensive care unit with continuous 5-lead electrocardiography, invasive blood pressure, pulse oximetry monitoring, and neurological assessment. All patients were monitored for ischemia by computerized ST-segment analysis for the first 48 hours after surgery.
Exposure Variable: CTnI
Blood specimens were taken for cTnI assessment before surgery, in the first, second, and third days postoperatively. This schedule was chosen according to previous findings. 4,7 The cTnI assays were performed in the hospital clinical laboratory with the use of the AxSYM Troponin-I ADV assay (Abbott Laboratories) on a routine AxSYM analyzer (Abbott Laboratories, Longford, Ireland). All the patient specimens were collected by the clinician and processed by the hospital-qualified laboratorian according to the manual strictly. The detection limit of the assay was 0.02 ng/mL. The single highest cTnI concentration was used as the exposure variable, and patients were considered to have myocardial injury if the peak serum level was more than 0.04 ng/mL.
Statistical Analysis
In the univariate analysis of baseline characteristics, dichotomous variables were compared by means of a chi-square test with the Yates correction or Fisher exact probability test, where appropriate. For continuous variables, the Kolmogorov-Smirnov modification of Lilliefor test was performed to test for normal distribution. Continuous variables of Gaussian distribution were compared by means of a Student t test and those of nonnormal distribution by the Mann-Whitney U test. Logistic regression analysis was also used as indicated. Estimated odds ratios and corresponding 95% confidence intervals and probability values are reported.
Continuous variables are presented as mean ± standard deviation or median (25th and 75th quartiles), whereas categorical data are presented as number (%). Results are considered significant whenever probability values are <.05. The SPSS, version 13.0 for Windows (SPSS Inc, Chicago, Illinois) was used for all the analyses.
Results
A total of 40 patients were included 32 men and 8 women, with a mean age of 67 ± 6.1 years (range, 60-79 years). All patients had transient ischemic attacks. In all, 19 (47.5%) patients had a nondisabling ischemic stroke before the preceding month; 6 (15%) patients had coronary artery disease under stable condition. The characteristics of the study population were described in Table 1. The cTnI levels of all the patients were within the normal range (≤0.04 ng/mL) before surgery. In all 17 (42.5%) patients showed myocardial injury during the first 3 days after surgery. All cTnI values peaked on postoperative day 1 and were below the level for diagnosing myocardial infarction (1.5 ng/mL). Previous stroke and abnormal ST-segment changes consistent with ischemia were the 2 preoperative predictors of an elevated cTnI, with odds ratios of 4.1 (95% confidence interval, 1.1-16.1) and 5.9 (95% confidence interval, 1.3-27.7), respectively (Table 1). There were no differences between cTnI positive and negative groups in age, gender, smoking habit, coronary artery disease, diabetes mellitus, uncontrolled hypertension, prior percutaneous transluminal coronary angioplasty, chronic cardiac medication, severe stenosed or occlusive contralateral carotid artery, Q waves consistent with previous myocardial infarction, echocardiogram, using shunt, the side of surgery, and serum creatinine. However, multivariate logistic regression analysis failed to identify statistically significant risk factors for postoperative elevation of cTnI.
Univariate Analysis of Associations Between Baseline Characteristics and Frequency of Perioperative Abnormal Cardiac Troponin I.a
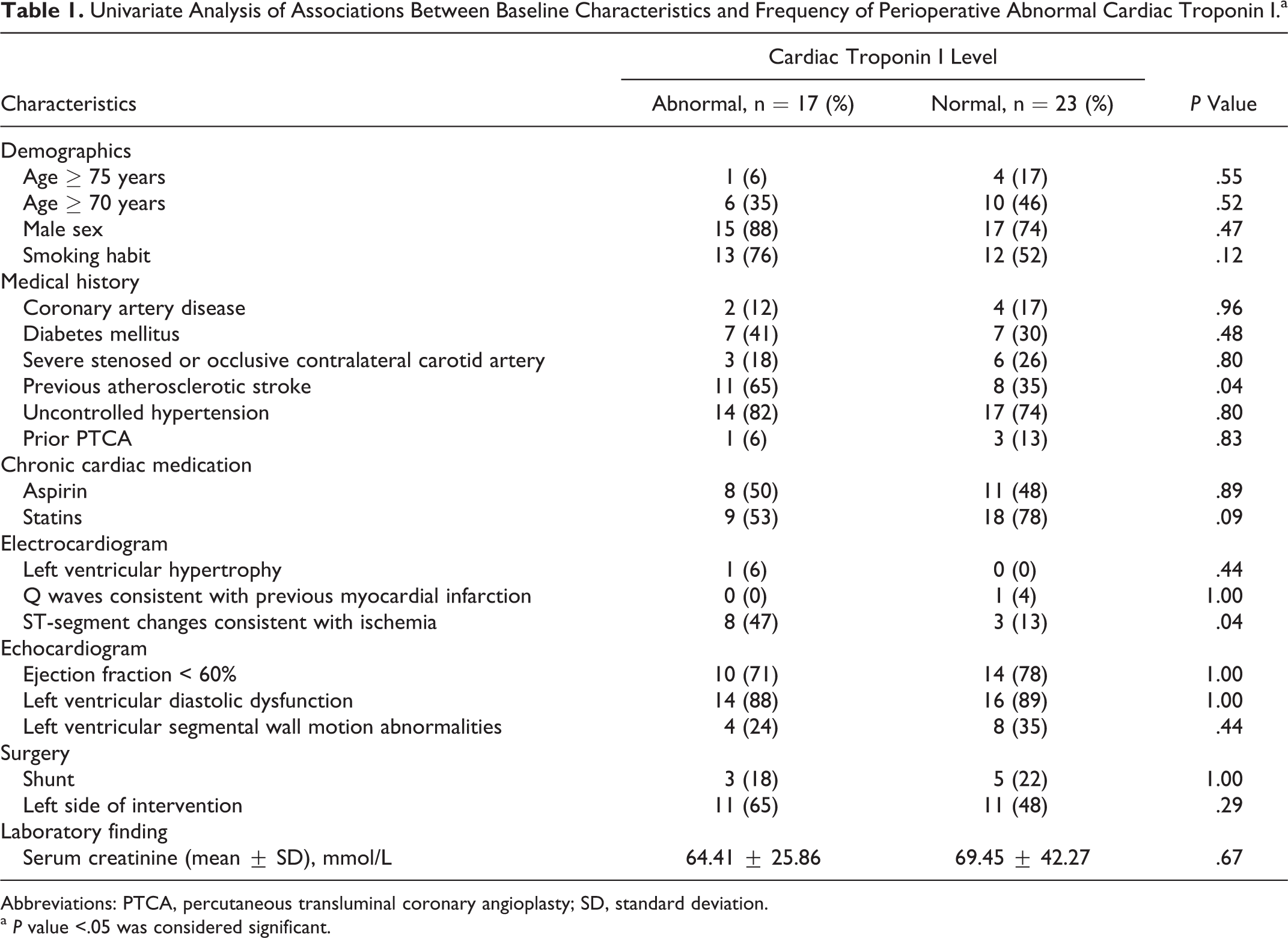
Abbreviations: PTCA, percutaneous transluminal coronary angioplasty; SD, standard deviation.
a P value <.05 was considered significant.
The variations of heart rate and blood pressure in all patients were within 20% of baseline. No hypotension, hypertension, or arrhythmias were recorded during anesthesia. Compared to patients with normal levels of cTnI, patients with an increased cTnI had a higher cardiac output index, stroke volume index, and a lower diastolic pressure and mean arterial pressure (Table 2). No differences were found in systolic pressure and heart rate during the operation. Phenylephrine and norepinephrine were not used in any patients. The cTnI positive patients had larger total dosage of ephedrine than cTnI negative patients. Patients with a higher cTnI had a smaller total dosage of urapidil, but the difference did not reach statistical significant (Table 2).
Hemodynamic Parameters and Dosages of Vasoactive Drugs Between Patients With Abnormal and Normal Cardiac Troponin I.a
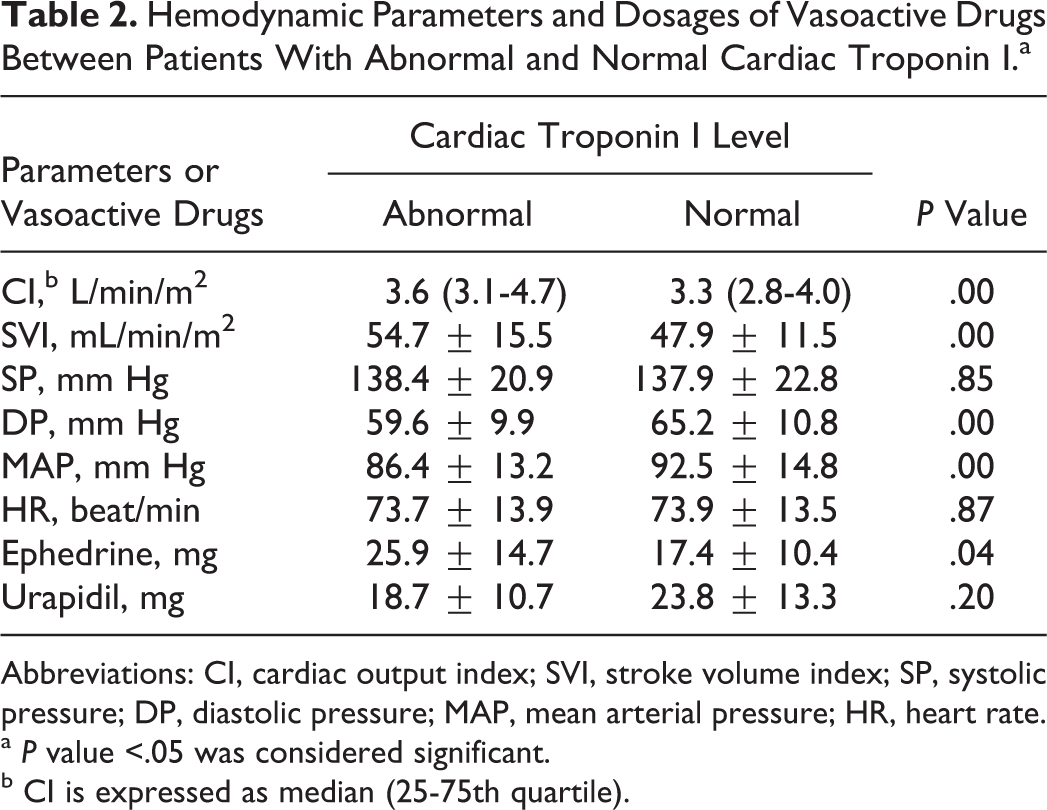
Abbreviations: CI, cardiac output index; SVI, stroke volume index; SP, systolic pressure; DP, diastolic pressure; MAP, mean arterial pressure; HR, heart rate.
a P value <.05 was considered significant.
b CI is expressed as median (25-75th quartile).
No patient had neurological complication. Two (5%) patients developed angina pectoris with new ST-segment changes on the first postoperative day, and both of them had an elevation of cTnI. Their symptoms were well controlled with nitrates.
Discussion
The association between asymptomatic perioperative troponin release after major vascular surgery and a worsened intermediate and long-term prognosis has been well established. 3 Barbagallo et al reported that an early increase in cTnI levels over 0.05 ng/mL was associated not only with an increased acute myocardial infarction but also with a delayed cardiac complications. 8 Landesberg et al considered that minor postoperative troponin elevations could be related to very minimal silent episodes of myocardial ischemia and predicted a greater risk of long-term mortality after vascular surgery. 7 Recently, Levy et al reported a meta-analysis of 14 studies, enrolling 3318 patients that demonstrated the independent prognostic value of even mildly increased postoperative cTn levels with odds ratio of 3.4 (95% confidence interval, 2.2-5.2) for mortality. 9
The incidence of myocardial injury in patients of our study was obviously higher than what was reported previously. 4 This might be related to the nature of our study. Moreover, we considered myocardial injury when cTnI levels exceeded the normal range (0.04 ng/mL), which were below the conventional value of 0.5 to 1.5 ng/mL associated with the diagnosis of myocardial ischemia. 4 All patients with ischemic myocardial injury were included not only those with accepted myocardial ischemia. This can partly explain the higher frequency of myocardial injury detected in the present study.
To investigate the potential predictors of an increase in cTnI levels after CEA, we included all of the possible factors associated with the cardiovascular diseases, the protopathy and the surgery. Apart from ST-segment changes, the results indicated that a history of ischemic stroke predicted the postoperative myocardial injury. This finding is in agreement with previous study that patients with previous stroke were more likely to have a cardiovascular event. 10 This is also in accordance with the new guideline of cardiovascular risk prediction instruments from the American Heart Association/American Stroke Association. 1 They declared that patients with atherosclerotic stroke should be included among those deemed to be at high risk of further atherosclerotic coronary events. 1 For the purposes of primary prevention, ischemic stroke should be included among cardiovascular disease outcomes in the absolute risk assessment algorithms. 1
The mechanism of myocardial injury after CEA is still unknown but possibly related to the high tissue factor (TF) activity. The TF is highly expressed in atherosclerotic plaques. Increased expression of TF in severe stenosed carotid arteries has been demonstrated to be associated with plaque destabilization, clinically evidenced by a history of previous ischemic symptoms. 11 Blood-borne TF contributes to the marked procoagulant activity that has been related to the hypercoagulability state in patients with acute thrombotic events in the heart. 12 Thus, patients with previous stroke or abnormal ST-segment changes might have higher TF activity, and more prone to have microemboli in coronary artery and myocardial injury. Further study should aim at the changes of TF activity related to CEA and its role in myocardial injury after CEA.
In our observation, patients with myocardial injury were likely to receive more vasoactive drugs support. Similar results have been reported in patients with abdominal aortic aneurysm. 13 Although the variations in blood pressure during the surgery were within the normal range, patients with myocardial injury had a lower diastolic pressure than patients with normal cTnI levels. This implied that cTnI positive patients had less oxygen supply for the heart than cTnI negative patients during the surgery, whereas the patients with higher stroke volume index in elevated cTnI group indicated greater work the heart did. Less oxygen supply and greater work may be the 2 important factors that may contribute to the minor thrombotic myocardial injury.
Several analytical interfering factors are associated with falsely elevated cTnI results and may lead to misdiagnosis of acute myocardial infarction or acute coronary syndromes. 14 In this study, the clinician and the laboratorian who collected and processed the patient specimens are hospital qualified. Furthermore, quality control specimens were analyzed to avoid the interference of analyzer malfunction after instrument maintenance. All of above have made sure that the cTnI levels in the current study were true and reliable. The other limitation of the present study is small sample size. A total of 40 patients were included in the study, despite the efforts to ensure the inclusion of representative patients. The small sample size may lead to the bias of this study.
Conclusion
The current observational study shows that more than 40% of patients had ischemic myocardial injury when presented to CEA for sympotomatic severe carotid artery stenosis. Those patients with previous ischemic stroke and abnormal ST-segment changes should receive more attention to myocardial injury.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.