
Abstract
Cardiac surgery involving cardiopulmonary bypass (CPB) is often associated with important blood loss, allogeneic blood product usage, morbidity, and mortality. Coagulopathy during CPB is complex, and the current lack of uniformity for triggers and hemostatic agents has led to a wide variability in bleeding treatment. The aim of this review is to provide a simplified picture of the data available on patients’ coagulation status at the end of CPB in order to provide relevant information for the development of tailored transfusion algorithms. A nonsystematic literature review was carried out to identify changes in coagulation parameters during CPB. Both prothrombin time and activated partial thromboplastin time increased during CPB, by a median of 33.3% and 17.9%, respectively. However, there was marked variability across the published studies, indicating these tests may be unreliable for guiding hemostatic therapy. Some thrombin generation (TG) parameters were affected, as indicated by a median increase in TG lag time of 55.0%, a decrease in TG peak of 17.5%, and only a slight decrease in endogenous thrombin potential of 7%. The most affected parameters were fibrinogen levels and platelet count/function. Both plasma fibrinogen concentration and FIBTEM maximum clot firmness decreased during CPB (median change of 36.4% and 33.3%, respectively) as did platelet count (44.5%) and platelet component (34.2%). This review provides initial information regarding changes in coagulation parameters during CPB but highlights the variability in the reported results. Further studies are warranted to guide physicians on the parameters most appropriate to guide hemostatic therapy.
Introduction
An epidemiological survey of transfusion in the United States, England, Australia, and Denmark showed that cardiovascular surgery utilizes a high percentage of all units of red blood cells (RBCs), platelets, and plasma. 1 Surgery involving cardiopulmonary bypass (CPB) is well known to be associated with increased blood loss, allogeneic blood products usage, morbidity, and mortality. 2 Activation of the hemostatic system during surgery can lead to important blood loss, and during CPB, additional factors such as hemodilution, anticoagulation, or contact activation with the extracorporeal circulation system can further contribute to the disruption of normal hemostasis. 3 –7
During CPB, close monitoring of the patient’s coagulation status is crucial and traditionally done using standard laboratory parameters, including prothrombin time (PT), activated partial thromboplastin time (aPTT), international normalized ratio (INR), activated clotted time (ACT), fibrinogen concentration, and platelet count. Although these tests are widely and routinely used, they involve long turnaround times, a critical limitation in settings where the patient’s coagulation status can change very quickly. Viscoelastic methods are increasingly employed in addition to standard laboratory tests. Conventional viscoelastic parameters recorded with TEG (Haemoscope Inc, Niles, Illinois) or ROTEM (Tem International GmbH, Munich, Germany) devices during CPB include ROTEM clotting time (CT), ROTEM maximum clot firmness (MCF), TEG reaction time (R), and TEG maximum amplitude (MA). Viscoelastic tests can be easily run at the point of care, thereby decreasing the time required to obtain informative data on patients’ coagulation status. Moreover, multiple tests can be run simultaneously on a single viscoelastic device, allowing for the assessment of various aspects of hemostasis and a more precise diagnosis of the underlying cause of coagulopathy.
The major causes of bleeding, complexity of coagulopathy, and available hemostatic therapies in cardiac surgery involving CPB have been extensively described. 3 –7 However, it is not clear which hemostatic or coagulation parameters are affected the most and consequently whether the current triggers for hemostatic therapy in this setting are appropriate. Therefore, a large variation in practice across institutes exists with regard to blood product usage in cardiac surgery. 8,9 Furthermore, a study involving patients undergoing primary elective coronary artery bypass graft demonstrated that 27% of transfusions were deemed unnecessary and 15%, 32%, and 47% of RBCs, plasma, and platelets, respectively, were inappropriate. 10
We undertook a nonsystematic search of publications describing changes in hemostatic and coagulation parameters during cardiovascular surgery involving CPB in adults, with the aim of depicting common and less common reported parameters usually considered as triggers in transfusion algorithms.
Literature Search and Data Collection
A nonsystematic search for publications describing both common and less common coagulation parameters during CPB was undertaken using PubMed. We retrieved data from original research articles providing both values at baseline and post-CPB (ranging from after protamine infusion up to intensive care unit admission). Studies were discarded if they did not provide numerical data.
A total of 25 publications were retrieved, covering studies involving cardiac surgery with CPB such as coronary artery bypass grafting, valve surgery/replacement, or other complex aortic cardiac procedures. The percentage change in hemostatic and coagulation parameters after CPB compared to baseline was calculated for each study using the mean or median values provided in the retrieved publications (Supplementary Tables 1–5). Parameters of interest were as follows:
– PT, aPTT, INR, ACT, and fibrinogen concentration.
– ROTEM EXTEM CT, MCF; ROTEM FIBTEM, MCF; and kaolin-activated TEG R, MA.
– Platelet count, platelet component (ROTEM EXTEM maximum clot elasticity [MCE]–ROTEM FIBTEM MCE), Multiplate (Roche Diagnostics Ltd, Rotkreuz, Switzerland) adenosine diphosphate (ADP), COL, and TRAP tests data.
– Factor (F) II, FV, FVII, FVIII, FIX, FX, FXI, FXIII activity; von Willebrand factor concentration (vWF); vWF antigen activity (vWF: Ag); vWF collagen-binding activity (vWF: CB); vWF ristocetin cofactor activity.
– Thrombin generation (TG) test lag time, peak, and endogenous thrombin potential (ETP); antithrombin activity (AT); thrombin–antithrombin III complex concentration (TAT); prothrombin fragment 1 + 2 (F 1 + 2) concentration;
Standard Laboratory Parameters
Described mean and median values at baseline and after CPB, and calculated percentage changes in standard laboratory parameters, are presented in Table 1.
Standard Laboratory Parameters.
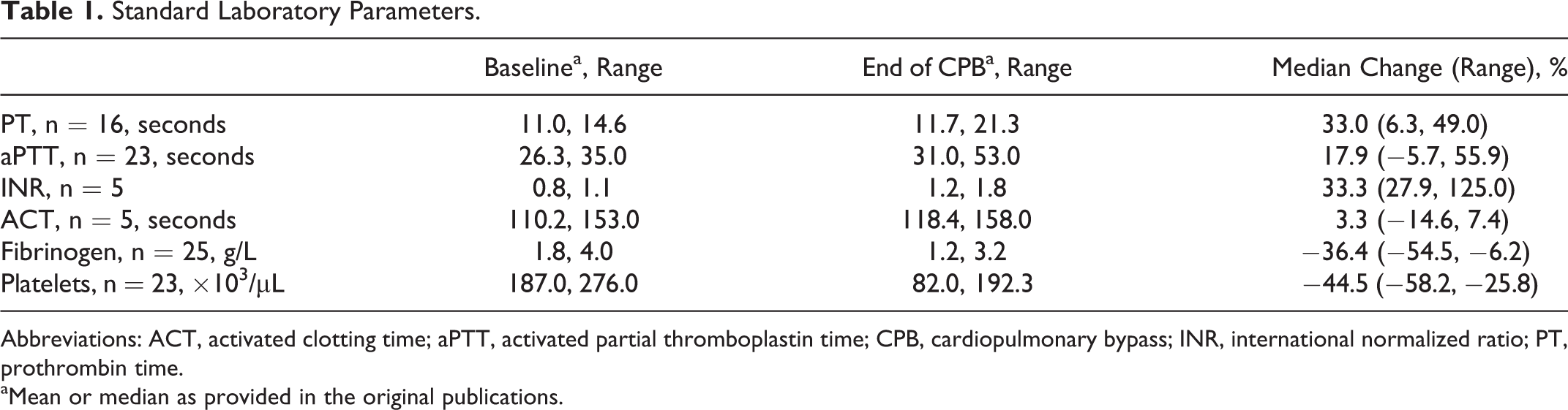
Abbreviations: ACT, activated clotting time; aPTT, activated partial thromboplastin time; CPB, cardiopulmonary bypass; INR, international normalized ratio; PT, prothrombin time.
aMean or median as provided in the original publications.
Prothrombin time, INR, and aPTT
Prothrombin time and INR (a normalized parameter derived from the PT) allow for the detection of defects within the extrinsic and common coagulation pathways; aPTT, on the other hand, provides information on the intrinsic and common coagulation pathways. These tests are run on citrated plasma samples and are therefore not affected by platelet numbers. Both PT and aPTT increase during CPB by 33.3% and 17.9%, respectively. The INR was increased by 33.3% during CPB. However, there was marked variability between studies with increases ranging from 27.9% to 125.0% after CPB compared to the baseline.
Activated clotted time
The ACT is commonly performed during CPB, as it allows the anticoagulant effect of heparin to be monitored. In addition, the extent of heparin neutralization by protamine at the end of the procedure can be assessed. This test is run on fresh whole blood samples and is known to be less sensitive than the aPTT. 11 Activated clotted time is only moderately affected during CPB, with an average increase of 3.3%. Reported values varied across studies, ranging from a 14.6% decrease to a 7.4% increase after CPB compared to baseline.
Fibrinogen Concentration
Plasma fibrinogen levels can be assessed by various methods, the most routinely used being the Clauss method run on citrated platelet-poor plasma samples. 12 Fibrinogen concentration after CPB was consistently decreased by an average of 36.4%. However, there were marked differences between studies with decreases ranging from 6.2% to 54.5%.
Platelet Count
Platelets play various roles within the coagulation process from the activation of coagulation factors to the physical maintenance of the clot. 13 Therefore, patients with a low platelet count are considered to be at risk of bleeding. The platelet count is traditionally monitored during CPB and was found to be strongly affected as shown by an average reduction of 44.5% (range: −58.2% to −25.9%).
Viscoelastic Parameters
Described mean and median values at baseline and after CPB and calculated percentage changes in viscoelastic parameters are presented in Table 2.
Viscoelastic Parameters.
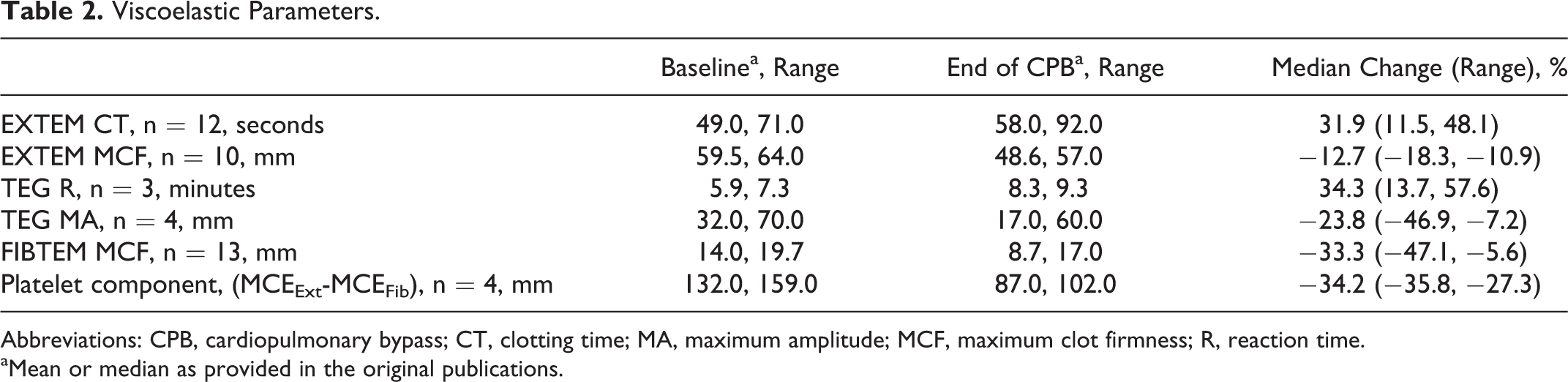
Abbreviations: CPB, cardiopulmonary bypass; CT, clotting time; MA, maximum amplitude; MCF, maximum clot firmness; R, reaction time.
aMean or median as provided in the original publications.
Overall clot parameters
The ROTEM EXTEM test and the standard TEG test are both run on whole blood samples in the presence of activators of the coagulation cascade (tissue factor in the EXTEM test and kaolin in the standard TEG test). These tests allow close monitoring of the kinetics of clot formation, thereby providing an indication for the time to initiation of coagulation (CT and R, respectively) and the time to maximum firmness (or strength) of the clot (MCF and MA, respectively). Prolonged CTs after CPB are observed with viscoelastic tests as shown by increased EXTEM CT and TEG R (31.9% and 34.3%, respectively). The strength of the clot is also affected during CPB as shown by reductions in both EXTEM MCF and TEG MA (12.7% and 23.8%, respectively).
Contribution of fibrin/fibrinogen to the clot
In addition to the EXTEM test, the FIBTEM test is often run simultaneously on the ROTEM device. In addition to tissue factor, the FIBTEM test contains the platelet inhibitor cytochalasin D; therefore, FIBTEM parameters provide information on the quality of the fibrin-based clot. The fibrin-based clot firmness is reduced during CPB as shown by an average decrease in FIBTEM MCF by 33.3% (ranging from 47.1% to 5.6%).
Platelet component
The platelet component provides an indication of the contribution of platelets to the clot and is calculated by subtracting FIBTEM MCF from EXTEM MCF. The overall contribution of platelets to the clot is reduced after CPB compared to baseline by an average of 34.2% (ranging from −35.8% to −27.3%).
Platelet Function
Described mean and median values at baseline and after CPB and calculated percentage changes in platelet function parameters are presented in Table 3. Platelet function tests, which can identify potential platelet disorders, are often run in addition to the platelet count. Multiplate analyses allow the quantification of platelet activation triggered by different pathways: the ADP receptor-dependent pathway in the ADP test; the collagen-dependent pathway in the COL test; and the TRAP-6-dependent pathway in the TRAP test. Platelet function declines during CPB, as shown by reductions in Multiplate parameter by an average of 70.0%, 65.1%, and 53.8% in the ADP test, COL test, and TRAP test, respectively.
Platelet Function Parameters.
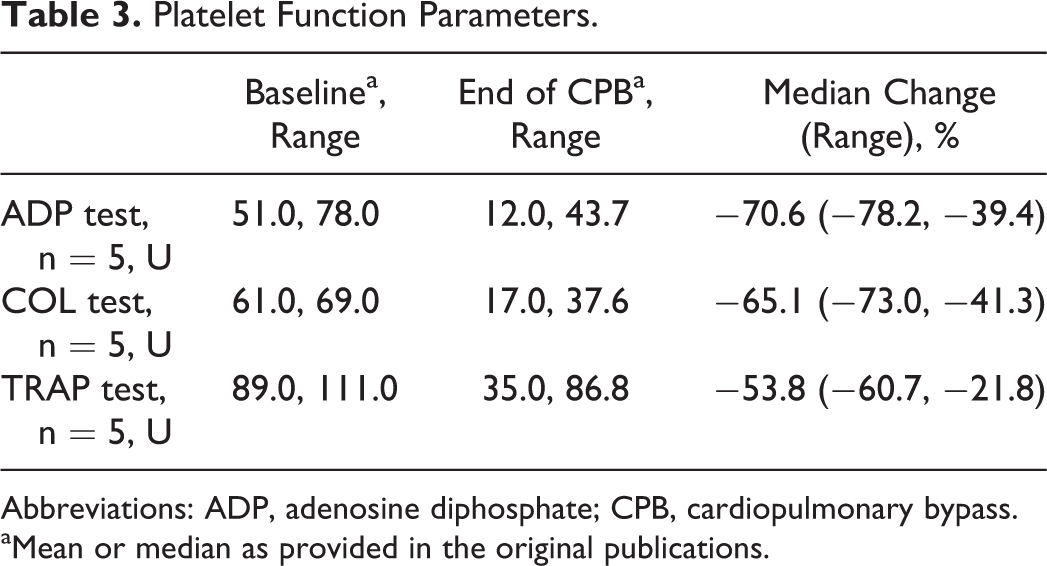
Abbreviations: ADP, adenosine diphosphate; CPB, cardiopulmonary bypass.
aMean or median as provided in the original publications.
Coagulation Factors Activity
Described mean and median values at baseline and after CPB and calculated percentage changes in the activity of coagulation factors are presented in Table 4. Most coagulation factors investigated show an overall decrease in activity during CPB. Factor II, FV, FVII, FX, FXI, and FXIII all strongly decrease by an average of 47.0%, 39.9%, 23.5%, 40.3%, 35.6%, and 33.6%, respectively. Changes in the activity of FVIII, FIX, and vWF are more varied. Factor VIII activity was found to decrease by an average of 9.8% during CPB; however, changes varied across studies as shown by a wide range of values (from a decrease of 29.9% to an increase of 34.8%). Similarly, FIX activity decreased by an average of 8.4%, ranging from a decrease of 29.9% to an increase of 13.0%. Finally, calculations of percentage changes in vWF: Ag and vWF: CB activities also varied, with increases of up to 13.0% and 18.8%, respectively, and decreases of 33.0% and 35.2%, respectively.
Coagulation Factor Activity.
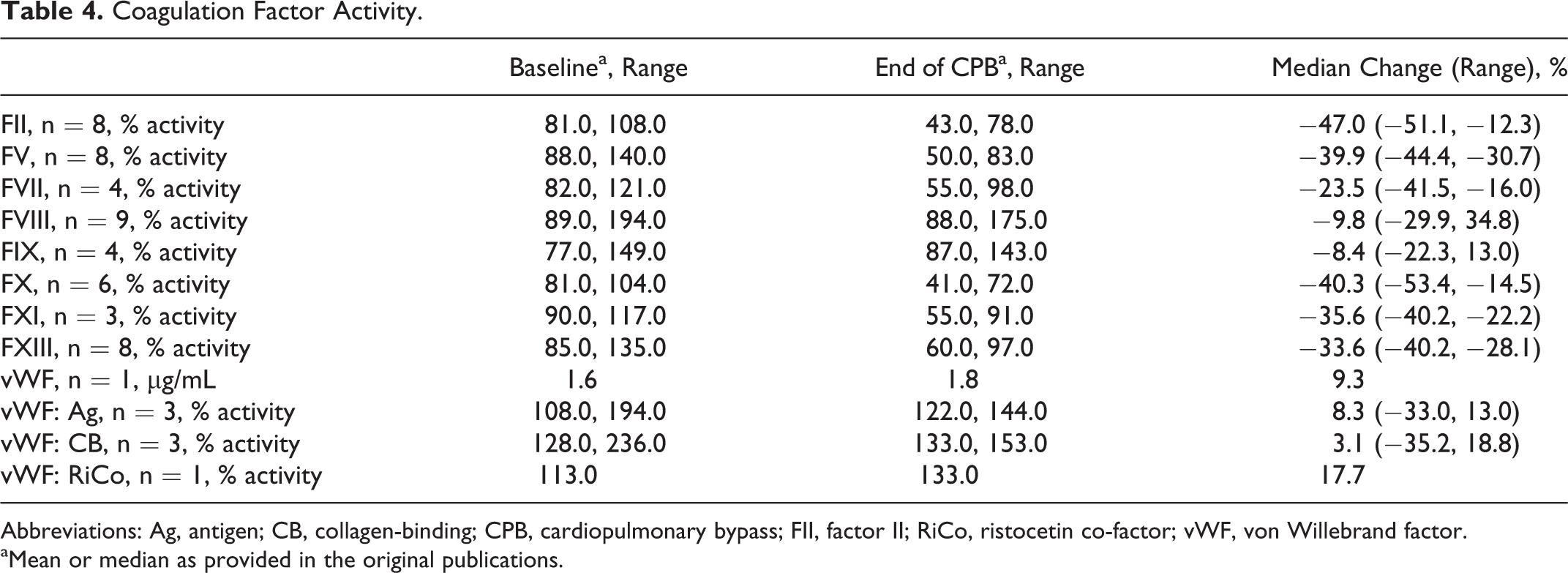
Abbreviations: Ag, antigen; CB, collagen-binding; CPB, cardiopulmonary bypass; FII, factor II; RiCo, ristocetin co-factor; vWF, von Willebrand factor.
aMean or median as provided in the original publications.
Thrombin Generation
Described values at baseline and after CPB, and calculated percentage changes in TG parameters, are presented in Table 5. Thrombin generation can increase as a consequence of the activation of the hemostatic system during CPB 14 and can be monitored by calibrated automated thrombography. Among the parameters provided by the TG curve, the lag time indicates the time to beginning of TG, the peak indicates the maximum concentration of thrombin generated, and the area under the curve indicates the ETP. Thrombin generation lag time increased by an average of 55.0% (range: 39.5%, 70.6%) after CPB. Furthermore, TG peak showed an average decrease of 17.5% (range: −28.1%, −6.9%), while TG ETP is minimally affected with a calculated decrease of 7.2% (range: −7.4%, −6.9%).
Thrombin Generation and Clot Lysis Parameters.
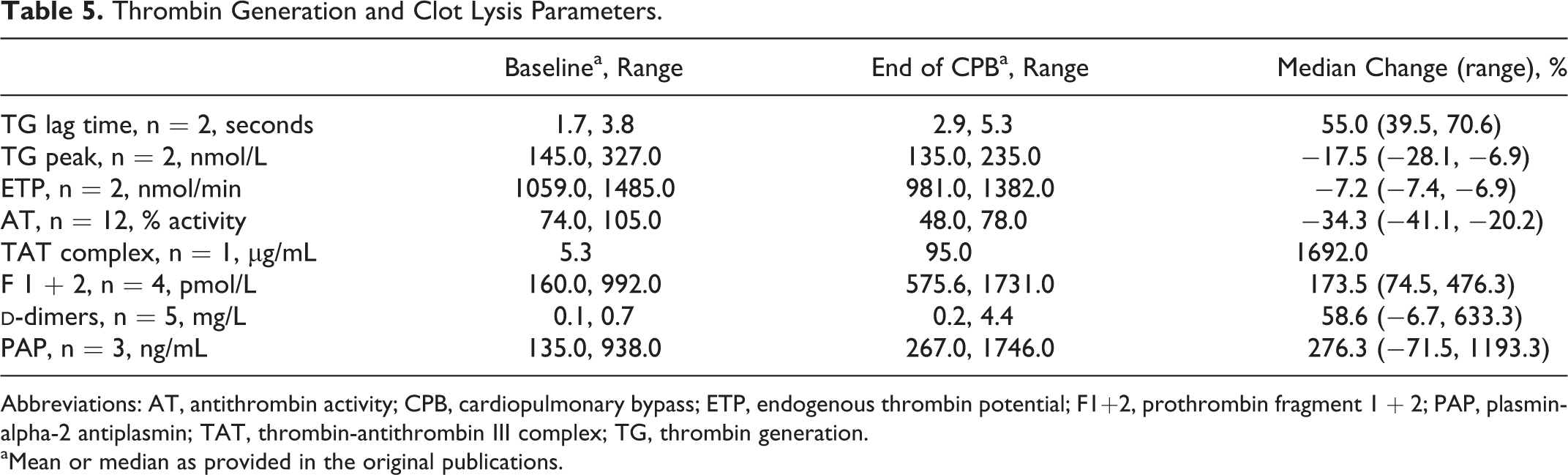
Abbreviations: AT, antithrombin activity; CPB, cardiopulmonary bypass; ETP, endogenous thrombin potential; F1+2, prothrombin fragment 1 + 2; PAP, plasmin-alpha-2 antiplasmin; TAT, thrombin-antithrombin III complex; TG, thrombin generation.
aMean or median as provided in the original publications.
Fibrinolysis
Described values at baseline and after CPB, and calculated percentage changes in clot lysis parameters, are presented in Table 5. Similar to TG, fibrinolysis can be strongly induced as a consequence of the activation of the coagulation cascade during CPB.
14
Fibrinolysis can be assessed by quantifying various markers, including AT activity, TAT complex levels, F 1 + 2 levels, and
Discussion
Cardiac surgery has been shown to utilize a significant percentage of allogeneic blood product units transfused, 1 and CPB is known to be associated with increased blood loss, allogeneic blood products usage, morbidity, and mortality. 2 Acquired coagulopathy can develop secondary to blood loss, consumption and loss of coagulation factors, and hemodilution, and this coagulopathy can lead to progression from initial bleeding to severe hemorrhage. Early targeted hemostatic therapy may prevent the development of complex coagulopathies and the progression to life-threatening hemorrhage. An understanding of the changes in coagulation status related to CPB would therefore be of use in the development of recommendations to guide such early treatment.
We initially considered the standard laboratory parameters due to their widespread availability and use. Prothrombin time and aPTT are generally described as useful to detect coagulation deficiencies 14,15 and are standardly used as hemostatic triggers to guide transfusion. However, they have been shown to be very poor predictors of bleeding. 16 Although both PT and aPTT increased during CPB, there was a marked variability across the studies retrieved (Table 1 and Figure 1). The use of prolonged PT and aPTT values as triggers to guide hemostatic therapy, in the absence of a strong relationship with bleeding tendency, might therefore lead to unnecessary transfusion of allogeneic blood products, exposing patients to an increased risk of adverse events (ie, transfusion-related acute lung injury or transfusion-associated circulatory overload), which may be detrimental to their health. 17,18 In addition, PT and aPTT are often used as triggers for hemostatic therapy with allogeneic blood products, such as plasma. It should be noted that there is currently a debate as to the usefulness of plasma, with little evidence to support its efficacy for the treatment of coagulopathic bleeding. 16
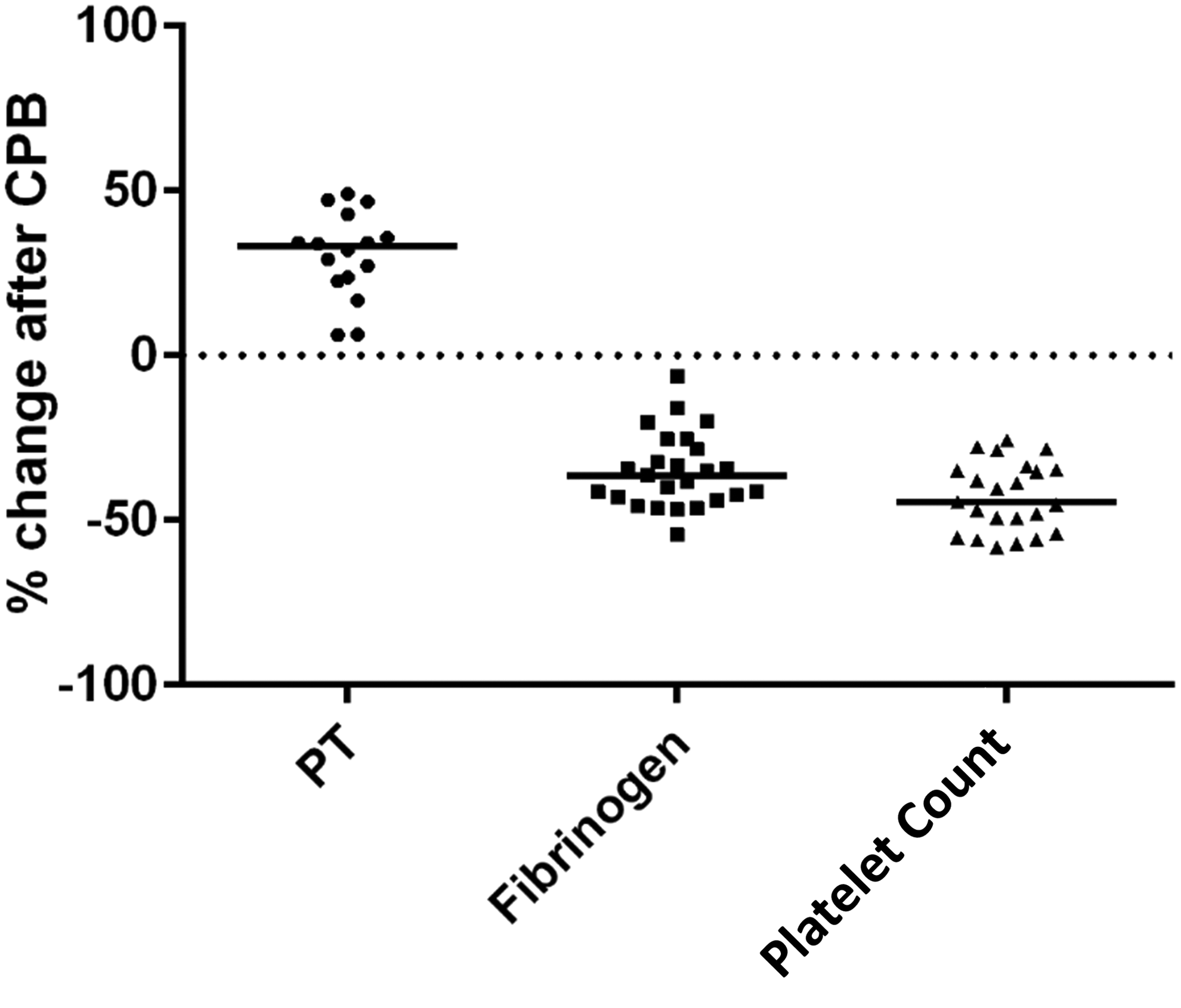
Prothrombin time, fibrinogen concentration, and platelet count percentage change after cardiopulmonary bypass (CPB). Graphical representation of percentage change in prothrombin time (PT), fibrinogen concentration, and platelet count calculated from published means/medians values at baseline and after CPB.
Viscoelastic tests are increasingly used, particularly at the point of care, and can reduce the time taken to obtain results. As part of our review, we considered the changes during CPB to standard laboratory parameters in conjunction with viscoelastic parameters. We observed an important decrease in plasma fibrinogen levels and a similar reduction in FIBTEM MCF (Figures 1 and 2). Interestingly, the extent to which both fibrinogen concentration and FIBTEM MCF decreased is comparable with the observed increase in PT; however, unlike PT, low fibrinogen concentration has been suggested to be predictive of increased bleeding in cardiac surgery. 19 –22 Fibrinogen is the first coagulation factor to reach critical levels during massive bleeding, 23 and point-of-care–guided hemostatic therapy, such as fibrinogen concentrate, to replenish fibrinogen levels is recommended in complex cardiovascular surgery. 24 Indeed, while primary hemostasis is also affected, various studies showed that fibrinogen has the strongest decline during CPB, and replacement therapy with fibrinogen concentrate was reported to be effective and well tolerated. 25 Additionally, high plasma fibrinogen concentration may compensate for thrombocytopenia or thrombocytopathia. 26 Furthermore, the recent European Society for Anesthesiology guidelines for the management of severe perioperative bleeding propose various recommendations in the cardiovascular setting, including, for example: “We recommend treatment with fibrinogen concentrate if significant bleeding is accompanied by at least suspected low fibrinogen concentrations or function. We recommend that a plasma fibrinogen concentration <1.5 to 2.0 gl−1 or ROTEM/TEG signs of functional fibrinogen deficit should be triggers for fibrinogen substitution.” 24(p275)
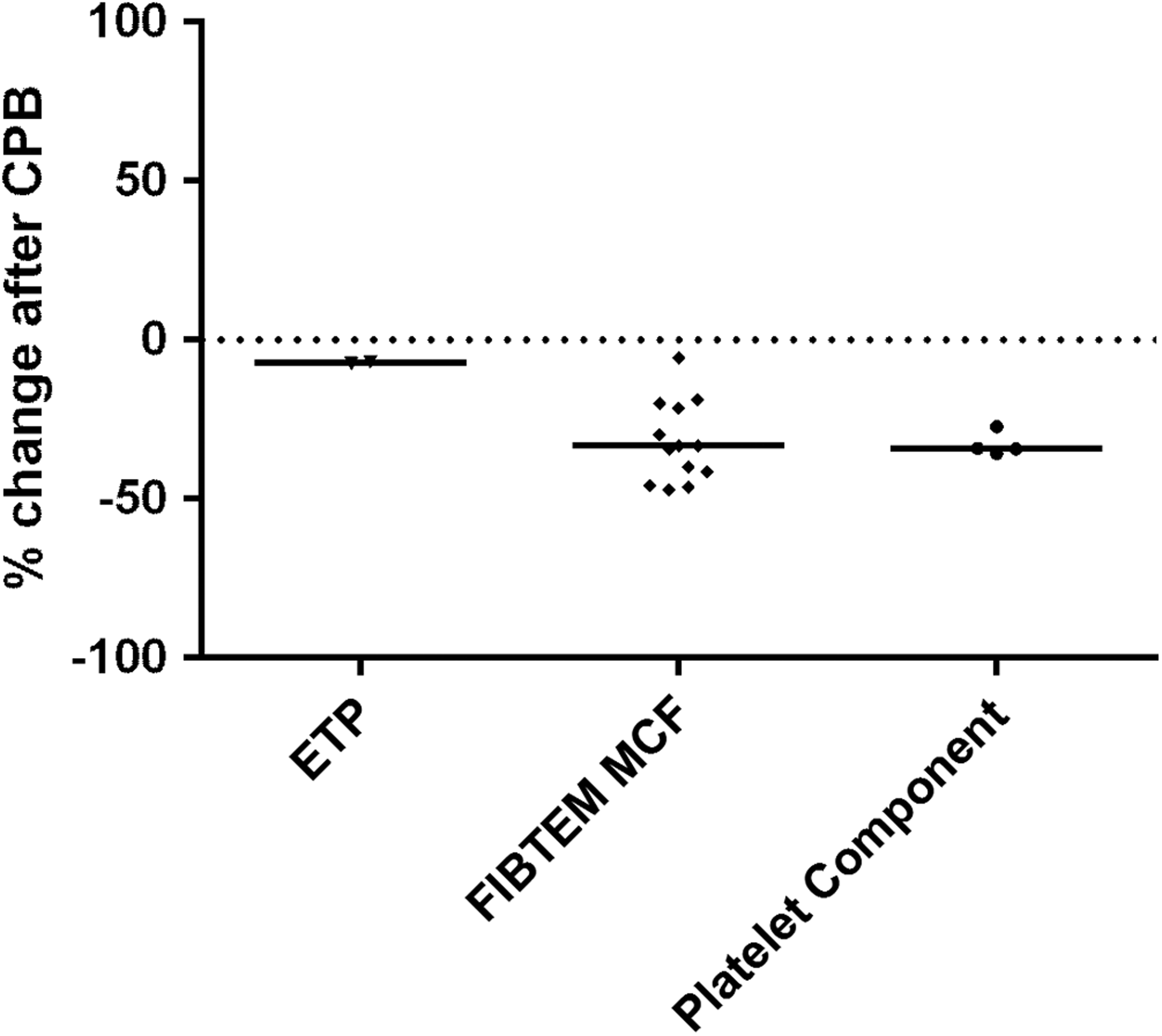
Endogenous thrombin potential, fibrin-based maximum clot firmness, and platelet component percentage change after cardiopulmonary bypass (CPB). Graphical representation of percentage change in endogenous thrombin potential (ETP), fibrin-based maximum clot firmness (FIBTEM MCF), and platelet component calculated from published means/medians values at baseline and after CPB.
Our observations also show a strong decrease in the platelet count and platelet component after CPB (Figures 1 and 2). Platelet transfusion is usually based on the platelet count; current guidelines recommend platelet administration in bleeding patients with characterized thrombocytopenia or with suspected platelet dysfunction. 27 Only a few studies have investigated the use of the platelet component as a trigger for platelet administration. However, it should be noted that the platelet component provides an indication of the contribution of platelets to the clot strength and, therefore, depends highly on both platelet count and function. Furthermore, we found a low variability in the change of platelet component during CPB between studies, which suggests this parameter might potentially be considered a more reliable trigger for platelet transfusion. In addition to the decrease in platelet count, platelet function is found to be greatly reduced. However, there is currently little evidence on the utility of platelet function tests to guide platelet administration.
Coagulation factors were not affected equally, with some showing consistent decreases in activity (FII, FV, FVII, FX, FXI, and FXIII) and others a varied response (FVIII and FIX). The significance of these changes is not currently clear, as blood loss after CPB is not correlated with changes in all coagulation factors, and differences in correlation were found between studies. For example, a correlation between blood loss and decreased FII or FVII has been previously described. 28,29
We also investigated reported changes to TG. Overall, while the time-related parameters such as TG lag time tended to be considerably prolonged, the parameters assessing the amount of thrombin generated, such as ETP, remained almost unchanged. In this context, immediately following cardiac surgery fibrin formation was shown to be significantly more impaired than both ETP and the platelet component of the whole blood clot. 30
A variety of mechanisms underlie the development of coagulopathy among patients undergoing CPB. At the outset, high-dose heparin is administered to prevent extracorporeal coagulation, and the CPB priming solution causes hemodilution. 4,7 Despite administration of heparin, use of the CPB circuit causes a degree of contact activation of coagulation; platelets may become activated, and inflammatory pathways are triggered. 5,6 At the surgical site, blood is exposed to air and tissue factor, further activating coagulation. These processes result in consumption of coagulation factors and platelets as well as increased fibrinolysis. 5,7 Thus, normal hemostasis may not be restored upon reversal of heparin at the end of CPB.
The limitations of this review are related to the amount of data retrieved, and the variability between reports regarding the type of change in some of the parameters investigated. This variability may be due to differences in patient populations or surgery types between studies. Additionally, there may be differences in CPB duration, or information was often not provided in the studies we retrieved, which may have affected the results reported. Finally, it is well known that differences in clinical practice exist among institutions and consequently, differences in hemostatic therapies used in the various studies could have also affected the extent to which some of the parameters changed during CPB. 31
Most of the hemostatic and coagulation parameters we investigated are affected during CPB, reflecting the overall destabilization of the clot which can lead to coagulopathic bleeding if not treated promptly. Coagulopathy during cardiac surgery involving CPB is complex; bleeding management varies among institutions and is mostly based on a limited number of triggers, which might not be predictive of bleeding risk (ie, PT and aPTT). Despite the overall changes throughout the coagulation system after CPB, not all parameters are affected to the same extent. Fibrinogen levels (reflected in plasma fibrinogen levels and FIBTEM MCF parameters) and platelet count/function (reflected in platelet count and platelet component parameters) are the most affected at the end of CPB. In contrast, ETP, vWF, and FVIII activities are some of the least affected parameters (Tables 4 and 5; Figure 2).
Our observations in this review suggest that first-line hemostatic therapy following CPB should be focused first on correcting impaired fibrinogen levels and/or platelet count/function before considering supplementation to correct a possible deficit in TG, vWF, or FVIII. However, further studies, where larger sets of coagulation and hemostatic parameters are investigated, are warranted in order to provide physicians with clearer views on which parameters would be most appropriate to guide hemostatic therapy during cardiovascular surgery involving CPB.
Footnotes
Acknowledgments
Editorial assistance with manuscript preparation was provided by Sandrine Dupré and Claire Crouchley of Meridian HealthComms Ltd, funded by CSL Behring.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. CS was an employee of CSL Behring at the time of writing and previously received speaker honoraria and research support from Tem International and CSL Behring and travel support from Haemoscope Ltd (former manufacturer of TEG®). CV-F has received research funding from CSL Behring. DF has received honoraria for consulting, lecture fees and sponsoring for academic studies from the following companies: Astra Zeneca, AOP Orphan, Baxter, Bayer, B. Braun, Biotest, CSL Behring, Cytosorb, Delta Select, Dade Behring, Edwards, Fresenius, Glaxo, Haemoscope, Hemogem, Lilly, LFB, Mitsubishi Pharma, NovoNordisk, Octapharma, Pfizer, Tem-Innovation. JH and JA have no conflict of interests.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.