
Abstract
Unfractionated heparin has remained the anticoagulant of choice in patients undergoing hemodialysis. However, wide variations in the heparinization responses have been observed in patients anticoagulated with this drug. The purpose of this investigation was to measure circulating heparin levels in patients with end-stage renal disease (ESRD) prior to and after maintenance hemodialysis. This study included 119 patients with ESRD undergoing maintenance hemodialysis who received heparin during dialysis. Citrated blood samples were collected prior to and immediately after the dialysis session and analyzed utilizing clot-based methods such as activated partial thromboplastin time (APTT), Heptest, and prothrombinase-induced clotting time (PiCT). Circulating anti-Xa levels, antithrombin III levels, and thrombin generation (TG) were also measured. The circulating heparin levels ranged from 0 to 1.08 IU/mL with a mean of 0.07 ± 0.11 for the APTT and a range of 0 to 1.98 for the Heptest with a mean of 0.09 ± 0.26 U/mL. There was no significant difference in circulating levels of heparin between pre- and post-hemodialysis samples using APTT, Heptest, and PiCT, whereas the TG and anti-Xa tests showed a statistically significant P value <0.05 when comparing the 2 groups. The presence of detectable levels of heparin in the predialysis plasma samples for almost two-thirds (87 of 119) of the patients suggests that residual heparin circulates in these patients for a longer period of time. In all, 5% of postdialysis samples, 6 of 119, contained >0.25 U/mL of heparin, which may be related to a central catheter vascular access flushed with heparin. These findings suggest that patients on maintenance hemodialysis may accumulate a detectable amount of heparin due to the decreased renal clearance.
Introduction
Unfractionated heparin has remained the anticoagulant of choice in patients undergoing hemodialysis. 1 Anticoagulation prevents thrombosis in the circulating blood and assures patency of the dialysis membrane. 2 In general, hemodialysis anticoagulation consists of a dose of heparin given as a bolus at the beginning of dialysis with a second dose in the middle of the treatment to maintain appropriate anticoagulation. Most dialysis units do not measure heparin levels routinely unless there is a problem with dialyzer clotting or prolonged bleeding following dialysis. However, there is a need to better optimize the amount of heparin given during hemodialysis. 3,4 A number of alternative forms of anticoagulation have been used in patients at increased risk of bleeding. 5 –11 This study focuses specifically on the use of unfractionated heparin during hemodialysis.
Wide variations in the heparinization responses have been observed in patients undergoing maintenance hemodialysis. In 2008, Brunet et al and Fourtounas described independently the substantial interindividual variability in unfractionated heparin pharmacokinetics. 12,13 The purpose of this investigation was to measure the circulating heparin levels in patients prior to and after hemodialysis. Heparin is used during the dialysis session to keep the patency of the dialysis circuit. In patients with end-stage renal disease (ESRD) on maintenance hemodialysis, heparin is used for an extended period of time. Because of the sole renal clearance of heparin components, it is likely that a significant amount of heparin may accumulate in these patients with impaired renal function. Given the short half-life of heparin 14 of approximately 1.5 hours, it is projected that no detectable levels of heparin would be found in the blood samples collected prior to routine hemodialysis sessions in patients on maintenance hemodialysis. However, because of frequent heparin administration and compromised renal clearance, it is likely that a significant amount of heparin may accumulate in these patients. To validate this hypothesis, the current studies were undertaken to detect the heparin level utilizing the available testing methods of this anticoagulant.
Materials and Methods
Materials
This study included 119 patients with ESRD undergoing maintenance hemodialysis after appropriate institutional review board approval and patient consent. Of the 119 patients with ESRD participating in the study, 57% were African American. The gender distribution was approximately equal with 58 female and 61 male patients participating in the study. We studied an older population with a mean age of 62.5 years (range 23-64). The etiology of ESRD was attributed to diabetes mellitus in 57.5%, hypertension in 27%, glomerulonephritis in 3.0%, and unknown in 12.5% of dialysis recipients. Most of the patients had been on hemodialysis for over 5 years with the exception of 1 new patient who completed his third month of hemodialysis 3 months prior to initiating the study. Adequacy of dialysis as measured by urea reduction rate >65% was achieved in 96% of the patients.
Hemodialysis was administered to patients 3 times per week following a Monday, Wednesday, and Friday protocol. For the 3- to 4-hour hemodialysis duration, a heparin-loading dose of 1000 units followed by 2 additional dosages of 500 heparin IU/hour was administered. Citrated blood samples were collected prior to and immediately after the dialysis session via venipuncture for all but 9 patients for whom a central catheter was used. The blood samples were centrifuged for 15 minutes at 3000 g at 4°C, and platelet-poor plasma was retrieved.
Methods
Citrated plasma was frozen at −70°C and analyzed utilizing clot-based methods such as activated partial thromboplastin time (APTT), Heptest, and prothrombinase-induced clotting time (PiCT). The circulating levels of heparin were determined using a calibration curve constructed from the heparin used in the dialysis unit. Results were computed for the individual tests, and heparin concentrations were obtained using assay-based calibration procedures using Microsoft Excel.
The APTT was performed on ACL 300 Plus kinetic coagulation analyzer (Beckman Coulter, Fullerton, California) using the Platelin reagent (Trinity Biotech, Bray, Colorado). Heptest was completed using reagents from Hemachem, Inc (St Louis, Missouri) with the use of a fibrometer. The PiCT was measured using the Pentapharm assay (Basel, Switzerland) via a fibrometer. Circulating anti-Xa levels were measured using a chromogenic substrate method; assays were run on ACL 300 Plus using bovine factor Xa from Enzyme Research Laboratories (South Bend, Indiana) and Spectrozyme Xa from American Diagnostica (Stamford, Connecticut).
The antithrombin (AT) III levels in each of these patients were also measured using a functional assay (American Diagnostica) that was run on ACL 300 Plus. Thromboplastin-induced thrombin generation (TG) was also measured using a fluorogenic substrate method, TG assay (Technoclone GmbH, Vienna, Austria) that was run on Technoclone TG Analyzer.
Statistical Analysis
We used a paired t test to compare pre- and post-hemodialysis data for each of the heparin assays used in the study. A P value <0.05 was considered to be statistically significant for a difference between pre- and posthemodialysis samples. The mean along with standard deviation and standard error of the mean was calculated.
Results
In the clot-based assays, such as APTT and Heptest, no significant differences between pre- and post-plasma samples were noted (Figure 1). The circulating levels of heparin in the predialysis samples were from 0 to 1.08 IU/mL with a mean of 0.07 ± 0.11 IU/mL for the APTT and a range of 0 to 1.98 IU/mL for the Heptest with a mean of 0.09 ± 0.26 IU/mL (Table 1). With the PiCT test, for the predialysis samples, the range was from 0.00 - 1.81 IU/mL with a mean of 0.08 ± 0.27 IU/mL, whereas for the postsamples, the range was from 0.00 - 0.53 IU/mL with a mean of 0.06 ± 0.08 IU/mL. For the anti-Xa levels, the percentage of inhibition for the pre- and postdialysis samples was similar (P = .08). The estimated circulating levels of heparin using anti-Xa in the predialysis samples ranged from 0 to 0.77 IU/mL with a mean of 0.10 ± 0.14 IU/mL, whereas the postdialysis levels ranged from 0 to 0.51 IU/mL with a mean of 0.13 ± 0.11 IU/mL (Table 1). For the TG, the percentage of inhibition levels ranged from 0% to 100% predialysis with a mean of 34.2% ± 34.2% and ranged 0% to 100% postdialysis with a mean of 44.5% ± 34.4%. The AT levels ranged from 28% to 130% with a mean of 86.6% ± 19.6% in the predialysis samples (Table 2). In all, 4 (3.4%) of the 119 patients had <50% ATIII (normal range, 80%-120%). The AT levels in postdialysis samples were not performed.
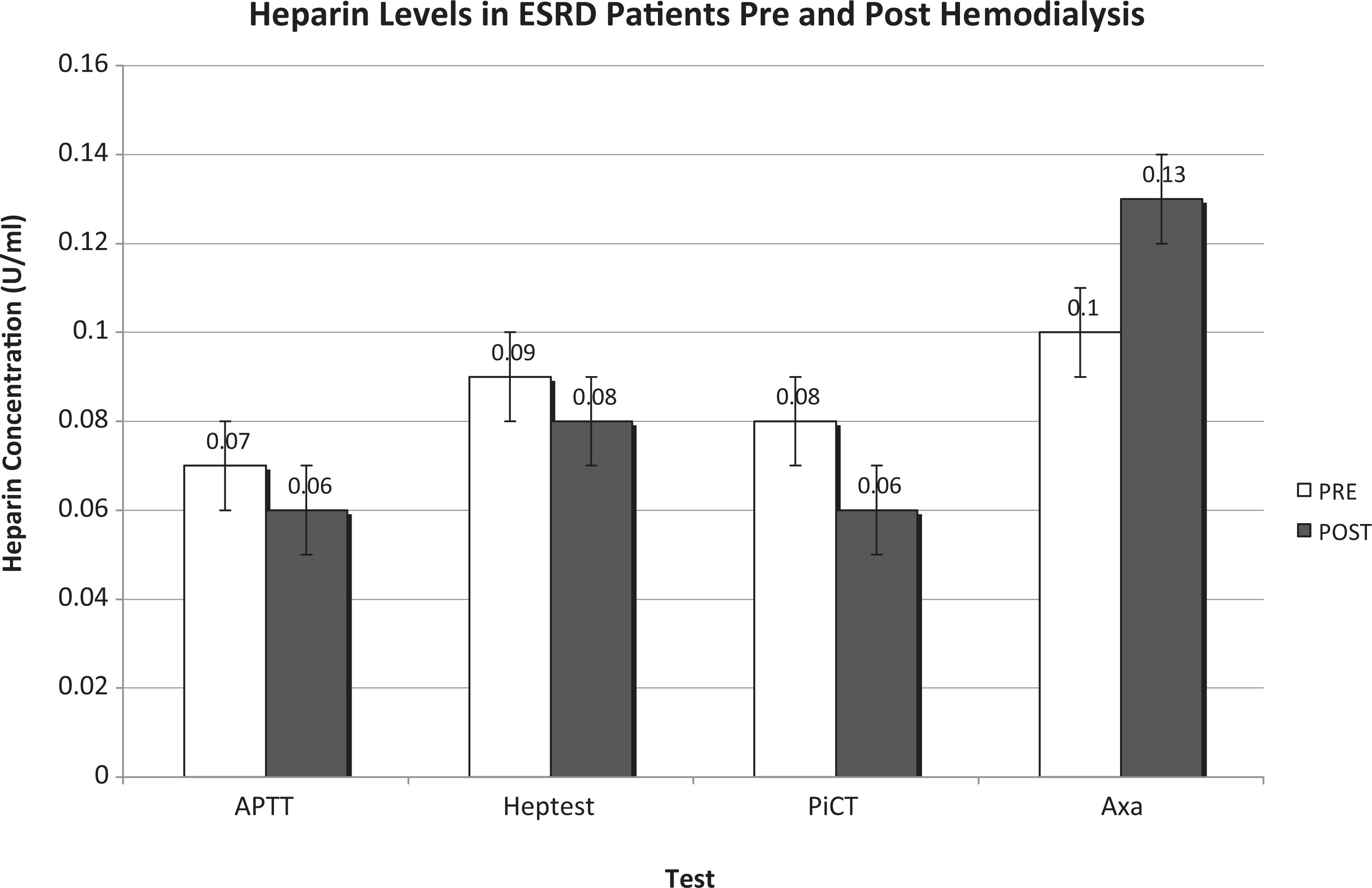
Heparin levels in patients with end-stage renal disease (ESRD) pre- and post-hemodialysis.
Comparison of Estimated Heparin Levels (IU/mL) Pre- and Post-Hemodialysis.
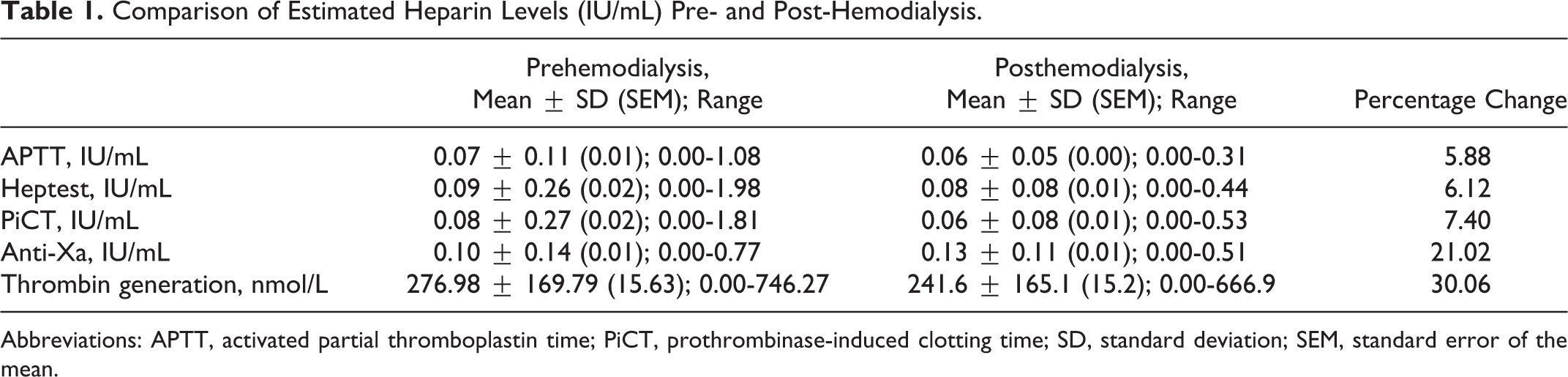
Abbreviations: APTT, activated partial thromboplastin time; PiCT, prothrombinase-induced clotting time; SD, standard deviation; SEM, standard error of the mean.
Antithrombin III Levels Prehemodialysis.
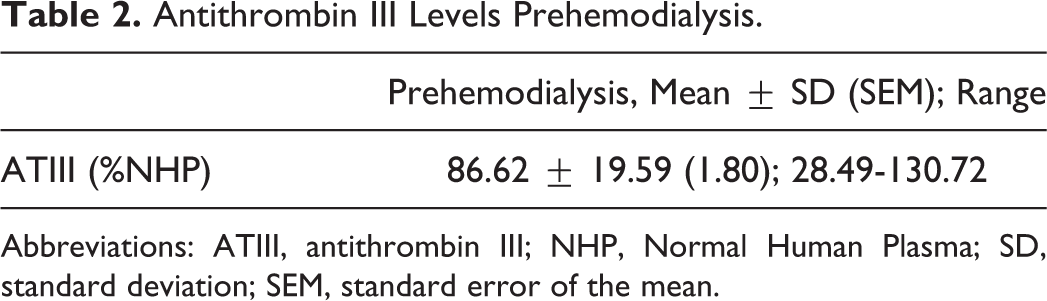
Abbreviations: ATIII, antithrombin III; NHP, Normal Human Plasma; SD, standard deviation; SEM, standard error of the mean.
There was no significant difference in circulating heparin levels between the cumulative means of the pre- and postdialysis samples using APTT, Heptest, and PiCT, whereas the TG and anti-Xa assays demonstrated a statistically significant difference with P values of 0.01 and 0.02, respectively (Figure 1).
Discussion
Wide variations in circulating heparin levels were noted in both the pre- and the postdialysis samples collected from these patients. The fact that detectable levels of heparin were present in the predialysis plasma samples for almost two-thirds (87 of 119) of the patients suggests that residual heparin circulates in patients with ESRD for a longer period of time. In all, 6 (5%) of the 119 of the pre- and postdialysis samples contained high heparin levels >0.25 IU/mL that may be related to a vascular access flushed with heparin. All 6 of these patients were among the 9 patients who had a perm catheter as their hemodialysis access. In the postdialysis samples, the circulating levels of heparin as measured by different tests were similar in most assays compared to predialysis samples.
The heparin measurement studies were carried out utilizing mainly APTT along with a newly developed PiCT and Heptest time. In addition, amidolytic anti-Xa and anti-IIa measurements were also made. The APTT is most widely used in the measurement of circulating heparin levels. The Heptest and PiCT are also sensitive methods to measure the anticoagulant activities of heparin at different sites in the coagulation cascade. The complex interaction between AT and heparin is measured using the anti-Xa and anti-IIa activities. Interestingly, in all these assays wide variations in heparin levels were noted.
Heparin is a polydispersed drug that is metabolized by the liver, and the remaining fragments are renally excreted. Since our patients with ESRD are renally impaired at varying levels, the noted variation in circulating levels of heparin supports the notion that differential elimination exists, and it is population dependent. Moreover, the differences in the results of different tests are due to the fact that each of these individual assays detects different properties of heparin fragments.
Unfractionated heparin represents a heterogeneous mixture of sulfate glycosaminoglycans ranging in the molecular weight from 2 to 50 kDa. Thirty percent of the oligosaccharide components of this anticoagulant are capable of binding to AT. The known anticoagulant components also exhibit affinity to different cells and proteins. The AT has a relatively longer half-life; therefore, the oligosaccharides with high affinity to this protein may exhibit longer duration of anticoagulant activity.
Moreover, heparin components also bind to the endothelium, and they are slowly released. As maintenance hemodialysis is repeatedly carried out, many of the binding sites are saturated, and even after circulating plasma heparin is cleared, the anticoagulant effects are manifested upon slow release of the endogenously bound heparin components. The current results support this hypothesis. The binding profile may vary widely among patients, and the observed results confirm this variation in our studies.
The AT levels varied widely in the predialysis samples. In all, 4 (3.4%) of the 119 patients had <50% AT and may have compromised heparin function. This may be due to an inherited thrombophilia that predisposes patients to venous thromboemobilsm. 15 However, AT levels may be decreased in patients with renal disease, especially nephrotic syndrome, as antithrombin is lost in the urine.
The results of all of the clot-based and chromogenic substrate assays reveal that both the pre- and the postdialysis samples had a sustained degree of hypocoagulation. These results also suggest that the administration of heparin during hemodialysis sessions is effective in preventing the formation of thrombus, and that residual heparin levels sustained their anticoagulant effects between dialysis sessions.
Conclusion
Wide variations in circulating heparin levels are noted in patients undergoing maintenance hemodialysis at predialysis and postdialysis time periods. Some patients exhibit higher levels of heparin due to a vascular access flush. These results also suggest that the use of heparin in patients undergoing maintenance hemodialysis in repeated regimen results in a steady-state hypocoagulation as evidenced by the inhibition of TG, the circulating anti-Xa level, and the prolongation of various clotting times.
Footnotes
Acknowledgments
The authors gratefully acknowledge the staff of the dialysis unit at the Loyola University Medical Center for their skillful assistance in collecting the blood samples and their processing. We are also thankful to Dr Eva Wojcik, Chairperson of the Department of Pathology, and Dr Richard Kennedy, Vice President Research Services of the Health Science Division of Loyola University, for their support in completing this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.