
Abstract
Background:
Red cell distribution width (RDW) has been shown to be helpful in predicting adverse long-term events in patients with cardiovascular diseases. However, to date, no study has been conducted on the relationship between RDW and thromboembolism risk in atrial fibrillation (AF). Therefore, we aimed to investigate the relationship between RDW and CHA2DS2-VASc score used for the evaluation of thromboembolism risk in patients with AF.
Methods:
The study population consisted of 320 patients with AF. We calculated CHA2DS2-VASc risk score for each patient and baseline hemoglobin, white blood cell, RDW, mean platelet volume, platelet counts, estimated glomerular filtration rate (eGFR), left ventricular ejection fraction (LVEF), and left atrial volume index (LAVi) were measured.
Results:
High CHA2DS2-VASc score group had higher RDW, lower LVEF, higher LAVi, and lower eGFR values when compared to the low CHA2DS2-VASc score group. The multivariate logistic regression analysis performed to predict high CHA2DS2-VASc scores revealed that RDW eGFR, LVEF, and LAVi were independent predictors. The area under the receiver–operating characteristic curve of RDW was 0.65 (0.59-0.71, P < .001) to predict high CHA2DS2-VASc score.
Conclusion:
Our study results indicate that RDW values are significantly correlated with CHA2DS2-VASc score in nonanemic patients with AF, while also being independent predictor of high CHA2DS2-VASc score.
Keywords
Introduction
Atrial fibrillation (AF) is a rather frequently encountered disease that causes serious thromboembolic complications and manifests increasing incidence by age. 1 There are many scoring systems evaluating thromboembolism risk in patients with AF. 2 –5 However, CHA2DS2-VASc is the most commonly recommended one. Each component of this scoring system has been shown to be associated with increased incidence of thromboembolism in cases of AF. 5 Red cell distribution width (RDW) is a marker that has become the focus of many recent studies, and it has been shown to be helpful in predicting adverse long-term events both in the general population and in patients with cardiovascular diseases such as coronary artery disease or heart failure and stroke. 6 –9 Furthermore, RDW has been shown to have a strong relationship with some of the components of CHA2DS2-VASc score. 10 –13 In addition, high intermountain risk score, which also includes RDW, has been shown to be correlated with higher risk of AF development. 14 However, to date, no study has been conducted on the relationship between RDW and thromboembolism risk in AF cases. Therefore, in this study, we aimed to reveal the relationship between RDW and CHA2DS2-VASc score used for the evaluation of thromboembolism risk in patients with AF.
Methods
Study Population
Our retrospective study consisted of 583 patients who presented to our hospital with AF between January 2011 and August 2012. The patients with prosthetic valve (n = 65), moderate-advanced valvular pathology (n = 136), baseline anemia (hemoglobin level <13 g/dL in men and <12 g/dL in women; n = 44), thalassemia trait (n = 4) as well as those with a history of blood transfusion within the first 3 months (n = 14) were excluded from the study. Our final study population consisted of 320 patients. Our study was approved by the local ethics committee.
Atrial fibrillation was defined as absence of p waves on electrocardiography and irregular R-R interval. The types of AF were defined as per European Society of Cardiology guideline. 15 According to this guideline, every patient who presents with AF for the first time is considered a patient with first diagnosed AF, irrespective of the duration of arrhythmia or the presence and severity of AF-related symptoms. Paroxysmal AF is of self-terminating character and continues for up to 7 days. Persistent AF is present when an AF episode either lasts longer than 7 days or requires termination by cardioversion, either with drugs or by direct current cardioversion. When AF lasted for ≥1 year and when it is decided to adopt a rhythm control strategy, it is called long-standing persistent AF. Permanent AF defines patients with long-standing AF in whom cardioversion fails or is not attempted. In this study, we employed CHA2DS2-VASc score that is used to estimate the risk of long-term thromboembolic events associated with AF (Table 1). 16 Thus, a score of “0” was recognized as low risk, “1” as intermediate risk, and ≥2 as high risk. 16
CHA2DS2-VASc Score.
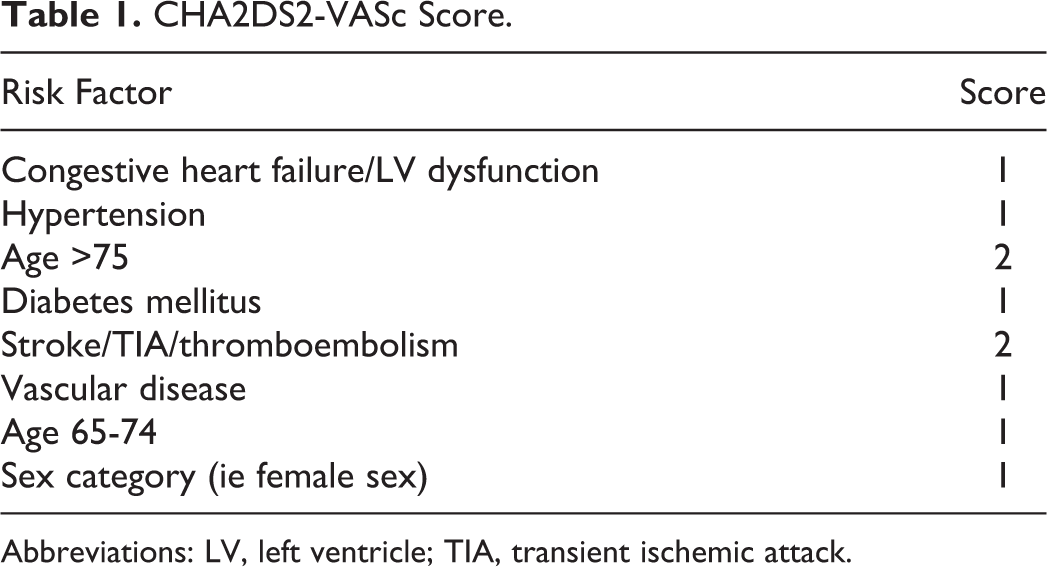
Abbreviations: LV, left ventricle; TIA, transient ischemic attack.
The data concerning age, gender, diabetes, hypertension, smoking status, dyslipidemia, previous history of myocardial infarction, previous history of valvular heart disease, previous history of coronary artery bypass grafting, thyroid disorders, congestive heart failure , peripheral artery disease, previous stroke/ transient ischemic attack, or systemic embolism were noted. Diabetes was defined as a fasting glucose level of >126 mg/dL in at least 2 separate measurements or previous use of antidiabetic drugs. Hypertension was defined as a blood pressure level of >140/90 mm Hg at least in 2 separate measurements or previous use of antihypertensive drugs. Patients with no transthoracic echocardiogram taken within the last 3 months were subjected to transthoracic echocardiogram. These transthoracic echocardiograms were used to check for the presence of valvular regurgitation or stenosis or prosthetic valvuli as well as to evaluate left ventricular ejection fraction (LVEF) by biplane Simpson method and left atrial (LA) volumes. 17
Baseline hemoglobin, white blood cell, neutrophil/lymphocyte ratio (NLR), RDW, mean platelet volume, and platelet counts were measured as part of the automated complete blood count using a Coulter LH 780 Hematology Analyzer (Beckman Coulter Ireland Inc, Mervue, Galway, Ireland). Furthermore, each patient was evaluated for lipid profile and estimated glomerular filtration rate (eGFR) was calculated by the Cockcroft–Gault Formula ([140 − age] × [weight in kg] × [0.85, if female]/[72 × creatinine]).
Statistics
Numerical variables were expressed as mean ± standard deviation, while categorical variables were expressed as percentage values. Comparisons between the 2 groups were made using the Student t test or Mann-Whitney U test or chi-square tests, as appropriate. Multiple logistic regression analysis was performed to identify the independent predictors of high CHA2DS2-VASc score. Receiver–operating characteristic (ROC) analyses were used to detect the cutoff value of RDW in prediction of CHA2DS2-VASc score. Correlation analyses between variables were performed using Pearson or Spearman correlation. A P value of <.05 was considered significant. All statistical analysis was carried out using SPSS 17.0 for Windows (SPSS Inc, Chicago, Illinois).
Results
The mean age of the 320 patients included in our study was 64 ± 11 years, and 52.2% of the entire study population was female. The median CHA2DS2-VASc score was 2, and 68.1% of the patients were in the high CHA2DS2-VASc group. In all, 27.8% of the cases were paroxysmal, 14% were persistent, and 58.2% were permanent AF. Other baseline characteristics and previous medications are shown in Table 2.
Baseline Clinical and Laboratory Characteristics According to CHA2DS2-VASc Score in Patients With AF.
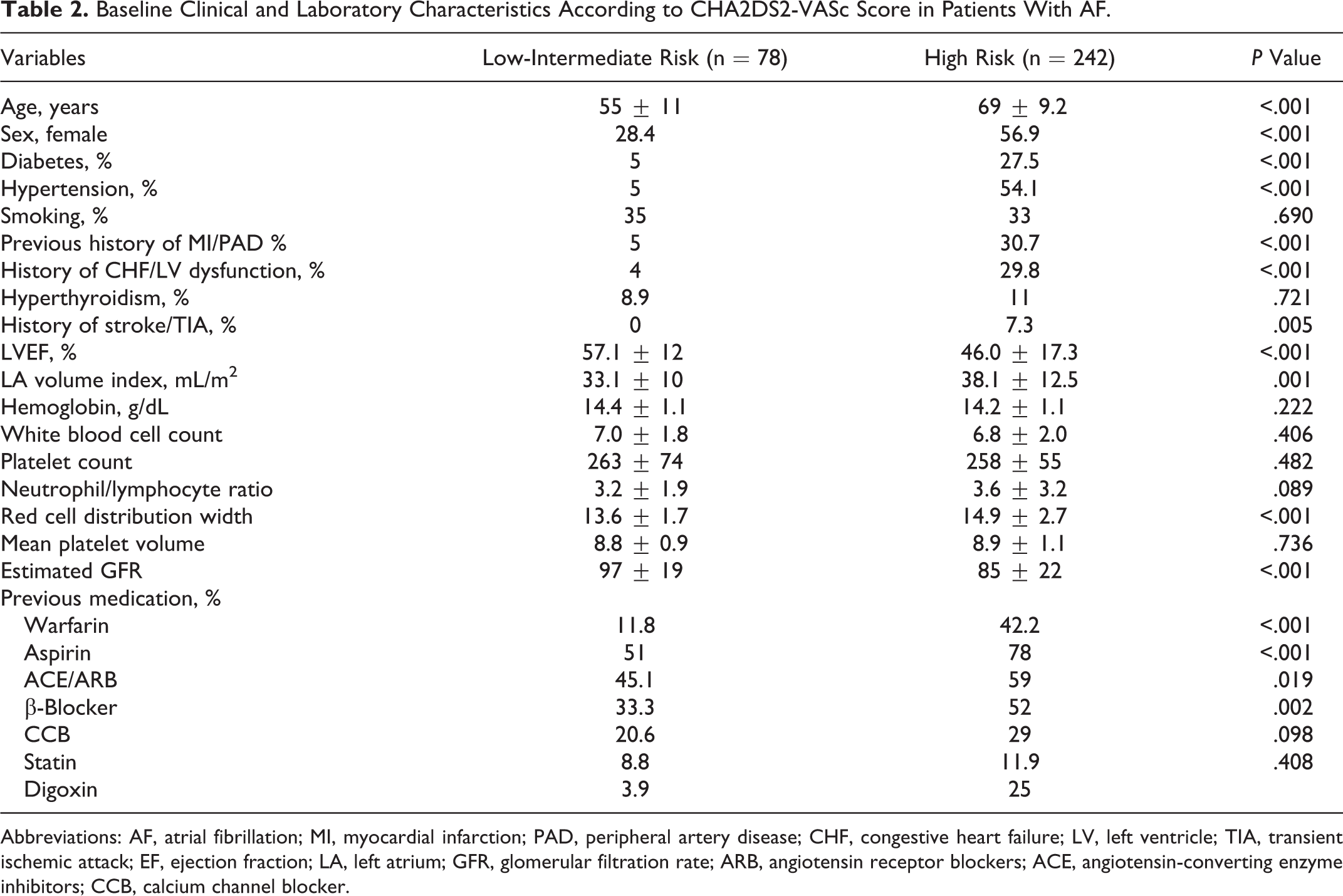
Abbreviations: AF, atrial fibrillation; MI, myocardial infarction; PAD, peripheral artery disease; CHF, congestive heart failure; LV, left ventricle; TIA, transient ischemic attack; EF, ejection fraction; LA, left atrium; GFR, glomerular filtration rate; ARB, angiotensin receptor blockers; ACE, angiotensin-converting enzyme inhibitors; CCB, calcium channel blocker.
High CHA2DS2-VASc score group had higher RDW, lower LVEF, higher LA volume index, and lower eGFR values when compared to the low CHA2DS2-VASc score group. The NLR ratio was similar in both the groups (Table 2). According to the correlation analysis, CHA2DS2-VASc score showed significant relationships with RDW (r = .383, P < .001; Figure 1), LVEF (r = −.322, P < .001), LA volume index (r = .244, P < .001), and eGFR (r = −0.216, P < .001). The multivariate logistic regression analysis performed to predict high CHA2DS2-VASc scores revealed that RDW, e GFR, LVEF, and LA volume index were independent predictors (Table 3). The area under the ROC curve of RDW was 0.65 (0.59-0.71, P < .001), LV-EF was 0.68 (0.63-0.73, P < .001), and eGFR was 0.65 (0.59-0.71, P < .001) to predict high CHA2DS2-VASc score. The best cutoff value of RDW to predict high CHA2DS2-VASc score was 14.05. A RDW value higher than 14.05 has a sensitivity of 65% and a specificity of 70% (Figure 2). The correlation of ROC curves of LVEF, eGFR, and RDW are shown in Figure 3. There were no significant differences in the ROC curves of these variables.
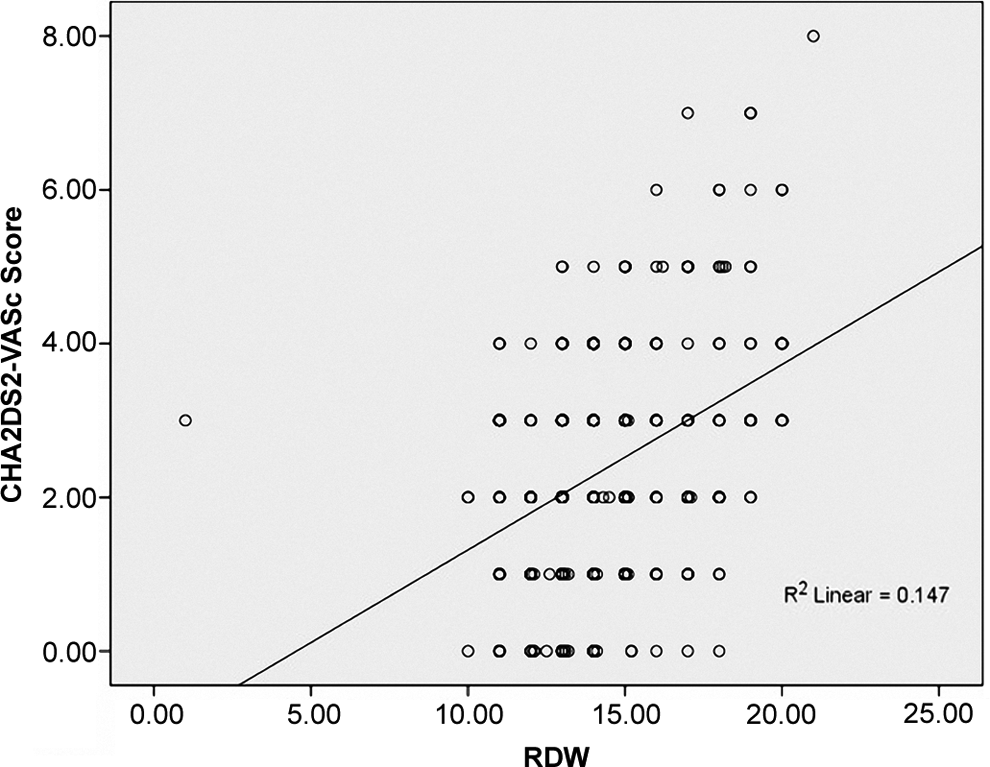
Correlation plots between red cell distribution width (RDW) value and CHA2DS2-VASc score.
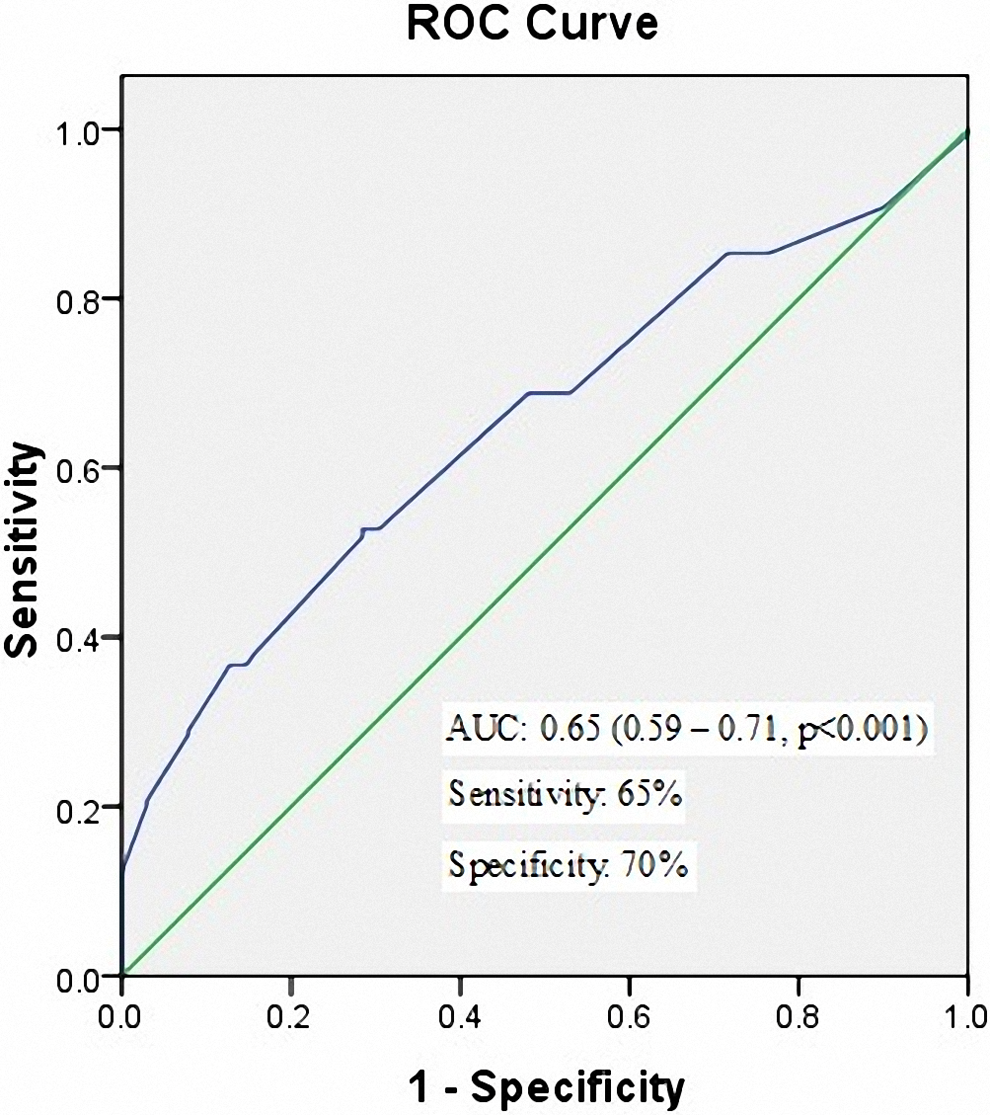
Receiver–operating characteristic (ROC) curves for red cell distribution width (RDW) values in prediction of high CHA2DS2-VASc score.
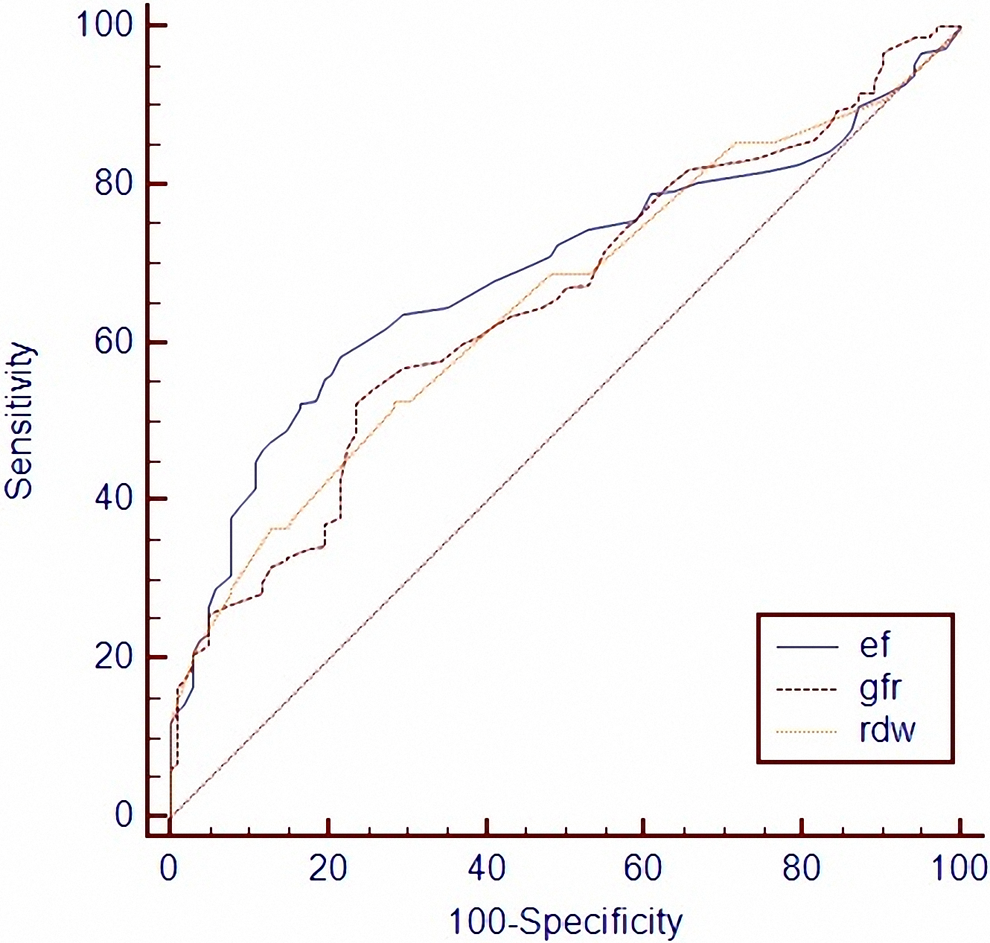
Comparison of left ventricular ejection fraction (LVEF), estimated glomerular filtration rate (GFR), and red cell distribution width (RDW) receiver–operating characteristics (ROC) curves.
Multiple Logistic Regression Analysis to Detect the Independent Predictors of High CHA2DS2-VASc Risk Score in Patients With AF.
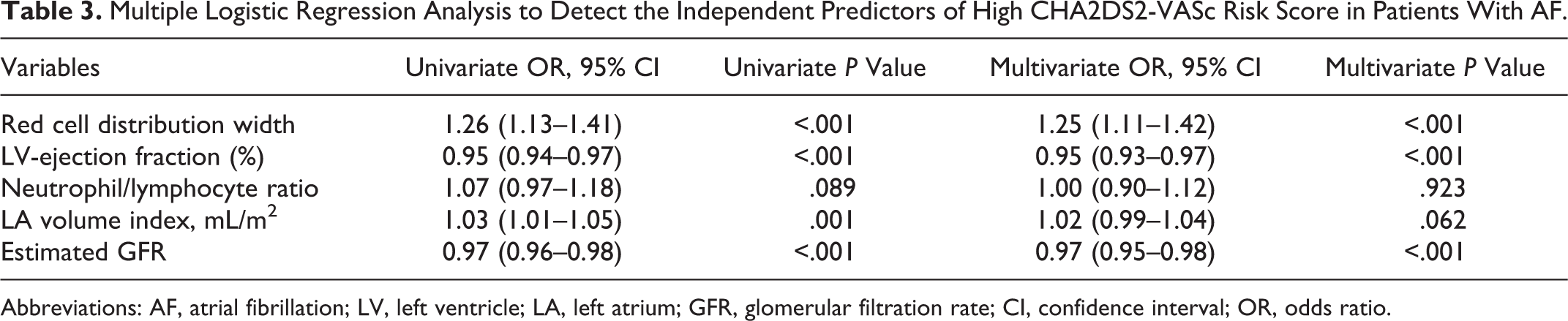
Abbreviations: AF, atrial fibrillation; LV, left ventricle; LA, left atrium; GFR, glomerular filtration rate; CI, confidence interval; OR, odds ratio.
Discussion
Our study results indicate that RDW values are significantly correlated with CHA2DS2-VASc score in nonanemic patients with AF, while also being independent predictor of high CHA2DS2-VASc score.
The AF is a widespread health problem that has a high incidence particularly at advanced ages. Thromboembolic events are one of the most serious complications of AF and they generally present in the form of ischemic stroke. 18 –20 However, the incidence of thromboembolism may vary relative to the coexisting clinical, echocardiographic, and biochemical factors in patients with AF. Thus, various scoring systems have been developed for the evaluation of thromboembolism risk by examining coexisting factors in AF such as clinical, echocardiographic, and biochemical factors. 2 –5 The CHA2DS2-VASc score is the most commonly recommended scoring system for the assessment of thromboembolism risk. 5,21 This score has been categorized in 2 groups in the evaluation of thromboembolism risk in patients with AF, low risk and high risk. Patients with AF with high CHA2DS2-VASc score exhibit increased incidence of thromboembolic events, and these patients benefit significantly from warfarin or aspirin therapy.
In this study, we found that 68.1% of the patients with AF had high CHA2DS2-VASc scores. The RDW value was determined to be correlated with CHA2DS2-VASc score as well as being an independent predictor of high CHA2DS2-VASc value. A RDW score of >14.05 was predictive of an augmented CHA2DS2-VASc score with 65% sensitivity and 70% specificity. The relationship between RDW value and CHA2DS2-VASc score can be explained by several mechanisms. First, RDW value may show a direct correlation with AF. In an intermountain risk score study, the investigators conducted long-term follow-ups and found that risk scores (including RDW) were a predictor of AF. 14 Second, patients with AF present with higher C reactive protein and brain natriuretic peptide and levels when compared to controls. 22 –25 These augmented levels might increase RDW. 26,27 Furthermore, RDW levels are high both in coronary artery disease, acute coronary syndrome, and in patients with heart failure 8,9,11,28 ; some of our patients had coexisting coronary artery disease and heart failure, as well. Finally, the relationships between several components of the CHA2DS2-VASc score and RDW have been shown by previous studies. 10 –13 In patients with heart failure, RDW values are higher when compared to controls, while patients with heart failure with higher RDW levels exhibit elevated incidence of adverse events in the long-term. 29,30 In addition, RDW levels are higher in patients with a history of stroke than in controls. 10 Furthermore, raised RDW is a good predictor of cerebrovascular events both in the general population and in patients with a history of stroke. 10 Similarly, RDW has a relationship with diabetes and hypertension, as well. 12,13
Thromboembolism risk stratification is very important in terms of preventing adverse events in patients with AF. We proposed that RDW values, which can be measured by a cheap and simple test, could be predictive.
Limitation
Our study had a relatively small number of patients. The most important limitations were the retrospective character of the present study and absence of long-term follow-ups. Further large-scale and prospective studies are needed in order to exactly clarify the role of RDW with regard to prediction of thromboembolic events.
Conclusion
We showed that RDW values were closely associated with thromboembolic risk shown by CHA2DS2-VASc score in patients with AF. Therefore, it could be used with this score in thromboembolic risk stratification. However, further studies of prospective and large-scale character are needed in this regard.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.