
Abstract
The study was conducted to evaluate the effect of anticoagulant therapy in women with thrombophilia and to detect the possible differences among carriers of mutations (factor V [FV] Leiden and FIIG20210) and those with natural anticoagulant deficiency. The 4-year prospective investigation included 85 pregnant women, with a history of recurrent fetal loss (RFL). They were treated with prophylactic doses of low-molecular-weight heparin (nadroparin) starting from 6 to 8 weeks of gestation. Pregnancy outcomes were evaluated based on the thrombophilia type. Carriers of thrombophilic mutations had a live birth rate of 93%, compared to 41.6% for women with natural anticoagulant deficiencies. Significant differences between the groups were also observed for intrauterine fetal death, intrauterine growth restriction, and postpartum thrombosis. The optimal therapy for women with natural anticoagulant deficiency and RFL remains unclear and future prospective study with a large number of patients is required to determine the best treatment for these severe thrombophilic conditions.
Introduction
Pregnancy loss is the most common gestational complication accounting for 12% to 15% of all clinically recognized pregnancies. The vast majority of losses occur in early pregnancy, and only 1% to 2% of the offsprings are lost after 12 weeks of gestation. 1 The presence of inherited thrombophilia and its association with recurrent fetal loss (RFL) was detected for the first time in 1996 by Sanson et al. 2 In large meta-analyses, different thrombophilic polymorphisms were identified to be connected with RFL. Moreover, the association depended on the type of thrombophilic disorder and the mode of fetal loss. 3,4 Our previous findings confirmed the association between thrombophilia and RFL and thus justified an investigation into this condition among women with pregnancy-associated complications in Serbia. 5,6 It is recognized that successful pregnancy outcome is dependent on the development and maintenance of an adequate utero-placental circulation, with evidence that prothrombotic factors underlie some pregnancy losses. 7 In particular, antithrombotic therapy may prevent pregnancy loss in the antiphospholipid syndrome, although this may not be an exclusively anticoagulant effect. 8 Data from several studies have provided substantial evidence that low-molecular-weight heparin (LMWH) might improve pregnancy outcomes in women with inherited thrombophilia and RFL. On the basis of these results, LMWH has been suggested to have the potential to improve live birth rates in high-risk pregnancies associated with thrombophilia. 9 –12 On the other hand, a study on the natural course in factor V (FV) Leiden carriers demonstrated that untreated patients with a history of habitual miscarriages or 1 previous fetal loss had 89% and 98% live birth rates, respectively. 13 A recently published meta-analysis included 5 studies, where live birth rate after LMWH treatment was investigated in women with thrombophilia. The LMWH may be beneficial, but the markedly favorable effect observed by Gris et al has not been replicated so far. 14 Very recently, 2 placebo-controlled randomized trials found no effect of thromboprophylaxis for women with 2 or more miscarriages, with or without thrombophilia. In these studies, a relatively small number of women with inheriteted thrombophilia were included (HABENOX study 24 women, SPIN study 10 women), with high but nonsignificant live birth rate for women with thrombophilia treated with enoxiparin. 15,16
In our prospective study, which is the first in our population, exclusively women with inherited thrombophilia were included and treated with LMWH in order to evaluate its effect on the pregnancy outcome. Since the lack of natural anticoagulants, especially antithrombin (AT) deficiency, represents severe thrombophilia, our second aim was to explore the possible differences between female carriers of prothrombotic mutations (FV Leiden and FIIG20210) and women lacking natural anticoagulants.
Study Design
Patients
The prospective study, carried out from January 2008 to June 2012 in 2 Serbian thrombosis centers (Blood Transfusion Institute of Serbia, Haemostasis Department, Belgrade and Institute of Laboratory Medicine, Clinical Center of Vojvodina, Novi Sad), involved 85 pregnant women with thrombophilia and previous miscarriages defined as pregnancy loss at a gestational age of 20 weeks or less. All the patients were interviewed about their medical history. The general demographic information, family history, previous venous thromboembolic events (VTEs), and obstetric history with outcomes in prior pregnancies were recorded. Pregnant women did not receive LMWH in previous pregnancies. The definition of miscarriage did not include the loss of a biochemical pregnancy (<6 weeks). Recurrent miscarriage was defined as at least 2 miscarriages. Participating women were tested before the current pregnancy for FV Leiden, prothrombin G20210A mutation, and plasma activity levels of AT, protein C, and protein S (PS). Deficiencies of natural anticoagulants were defined as less than 75% of normal activity for AT, less than 69% of normal activity for protein C, and less than 65% of normal activity for PS. If the results were below the normal range, the assays were repeated using another plasma sample. Prior to thrombophilia testing, all women were interviewed about taking medications such as antibiotics, vitamin K antagonists, or hormonal therapy (estrogen) as well as about the presence of acute infections, bowel disease, kidney, or liver disease, in order to minimize the presence of acquired deficiency of natural anticoagulants especially protein C or protein S. Women with antiphospholipid antibodies were excluded from the study (all of them were tested for lupus anticoagulant, anticardiolipin, and antiβ2glycoprotein 1 antibodies).
Methods
Women were included when a viable intrauterine pregnancy was confirmed on ultrasonography. The treatment protocol consisted of a prophylactic body weight-adjusted dose of LMWH (nadroparin) once daily, started between 6 and 8 weeks of gestation, in all the cases. Depending on the body weight, the doses of LMWH ranged from 2850 to 5700 IU and the treatment was continued throughout the pregnancy and for 6 weeks following delivery for thromboprophylactic reasons. Participating women received standard care provided by their own obstetrician throughout pregnancy, including structural fetal ultrasonography at 18 to 22 weeks of gestation. At the initial visit in the first trimester, blood was drawn for routine assessment of full blood count, coagulation screening, and
Outcome Measures
The primary outcome measure was the live birth rate. Secondary outcomes included rates of miscarriage defined as early (before 12 weeks of gestation) or late (after 12 weeks of gestation) intrauterine fetal death (IUFD), defined as fetal death after 20 weeks of gestation and obstetrical complications.
18
Such complications included intrauterine growth restriction (IUGR) defined as birth weight below the 10th percentile for gestational age and sex, placental abruption, preeclampsia, and premature delivery.
19
Premature delivery was divided into subgroups according to weeks of gestational age (24-28, 28-32, or 32-37 weeks of gestation). The rates of maternal complications included thrombocytopenia defined as a platelet count of <1 50 000 × 109/L, bleeding complications, and skin allergic reactions as well as the occurrence of VTE during pregnancy or postpartum. The
Institutional approval for the study was granted by the Local Research Ethics Committee in accordance with internationally accepted ethical standards and each patient signed the informed consent form.
Statistical Analysis
The analyses were performed using Medcalc, Belgium. Differences between the groups were estimated by chi-squared test, Fisher test, and Student t test. The probability value P < .05 was considered to indicate statistical significance.
Results
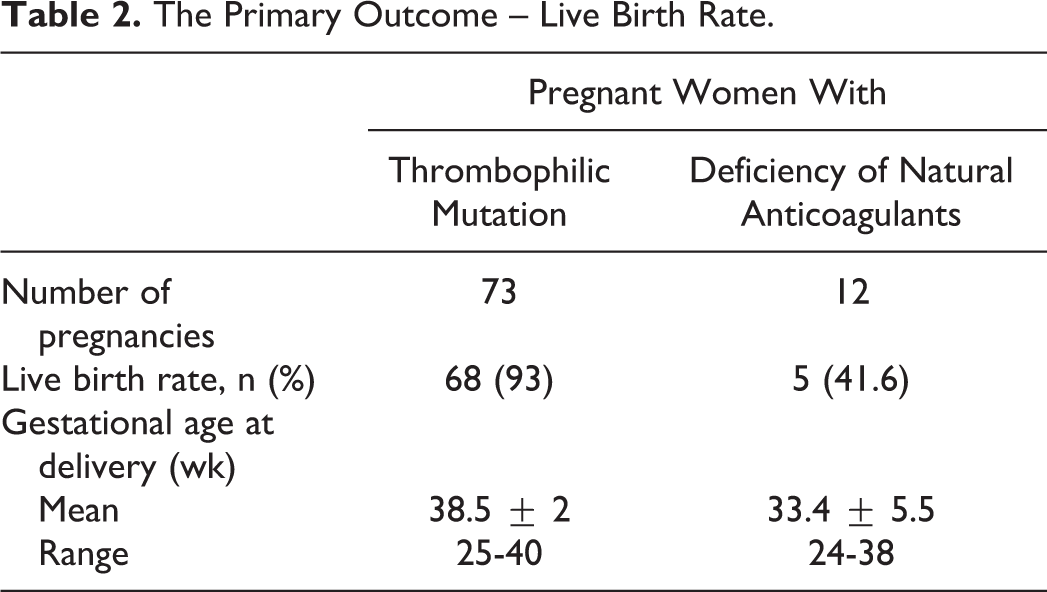
Among the 85 pregnant women, 73 carried prothrombotic mutations (51 were heterozygous carriers of FV Leiden and 22 were heterozygous carriers of the prothrombin G20210A mutation). In all, 12 women were deficient in natural anicoagulants, 8 with AT deficiency (AT activity from 33%-65%), and 4 with PS deficiency (PS activity from 34%-38%). A significant difference between the 2 groups of women was observed only for previous early fetal loss (P = .008), while the other characteristics (age, number of previous miscarriages, late fetal loss, and IUFD) were similar in both the groups (Table 1). Analysis of pregnancy outcome regarding the type of thrombophilia showed that the carriers of FV Leiden and FIIG20210A mutations treated with LMWH had a high live birth rate of 93%, while the live birth rate was 41.6% for the women deficient in natural anticoagulants (Table 2). Early fetal loss was observed in 5.5% of the women with thrombophilic mutations and in 33.3% of those with a natural anticoagulant deficiency. The difference between the 2 groups for IUFD was also significant, with an incidence of 1.3% in the thrombophilic mutations group and 25% in the lack of natural anticoagulants group. Similar differences were recorded for IUGR and preterm delivery. Thus, among women with natural anticoagulant deficiency 25% of the pregnancies ended as preterm delivery mainly due to IUGR, while in the thrombophilic group this was less prevalent (8.2%; Table 3). The rate of late fetal loss plus IUFD among women with anticoagulant deficiency decreased in the study compared to previous pregnancies without treatment (Table 4). In comparison to the women with thrombophilic mutations, the effect of LMWH was not as favorable. Despite the use of prophylactic anticoagulant therapy in 2 women after miscarriage and in 1 after delivery, venous thrombosis developed in 1 case complicated with pulmonary embolism. All women were from the group with AT deficiency (Table 3). Regarding maternal adverse events, such as thrombocytopenia, local skin reactions, necessary change of heparin formulation, or bleeding complications, there were no differences between the subgroups (Table 3). The analysis of hemostatic activity, measured by
Characteristics of the Study Population (N = 85).a
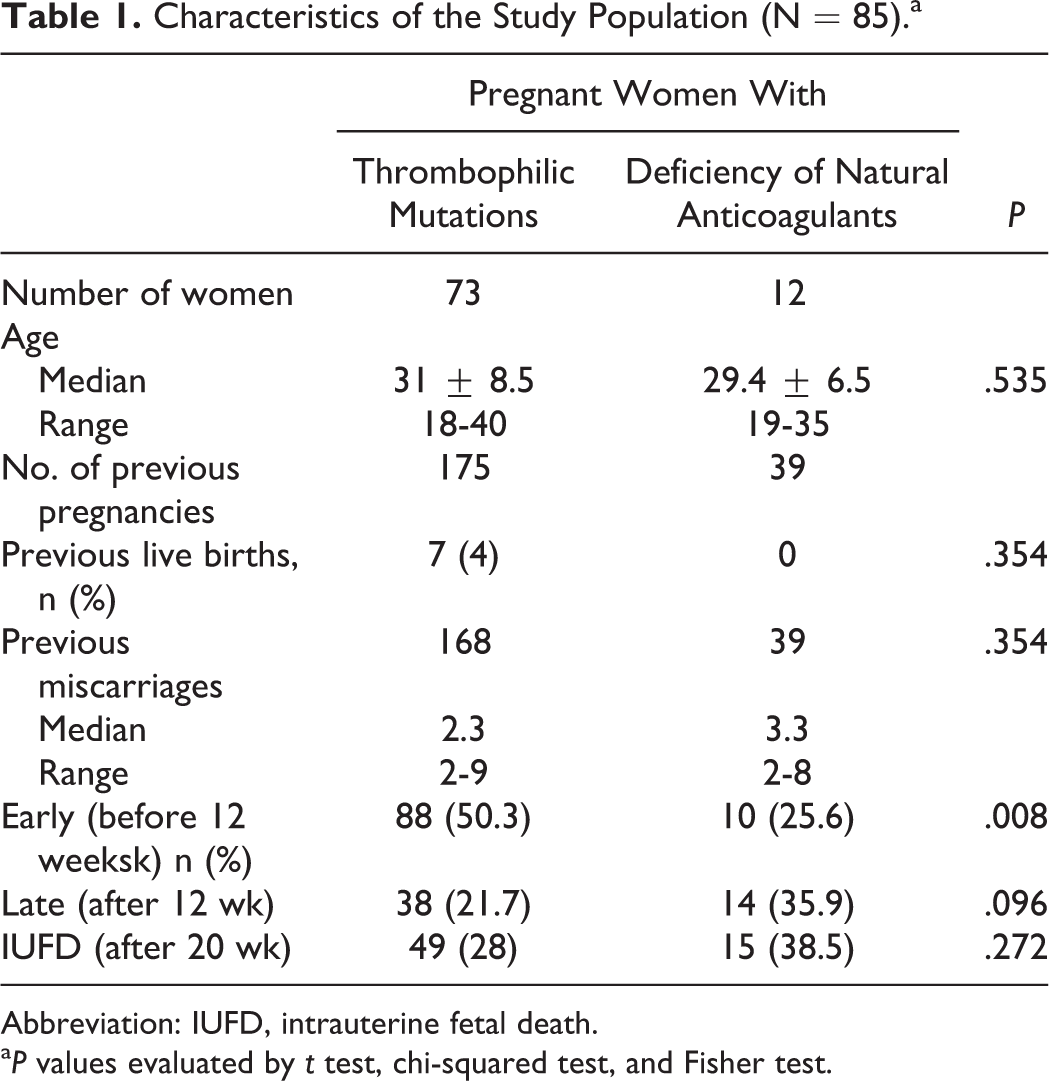
Abbreviation: IUFD, intrauterine fetal death.
a P values evaluated by t test, chi-squared test, and Fisher test.
The Primary Outcome – Live Birth Rate.
Secondary Outcomes.
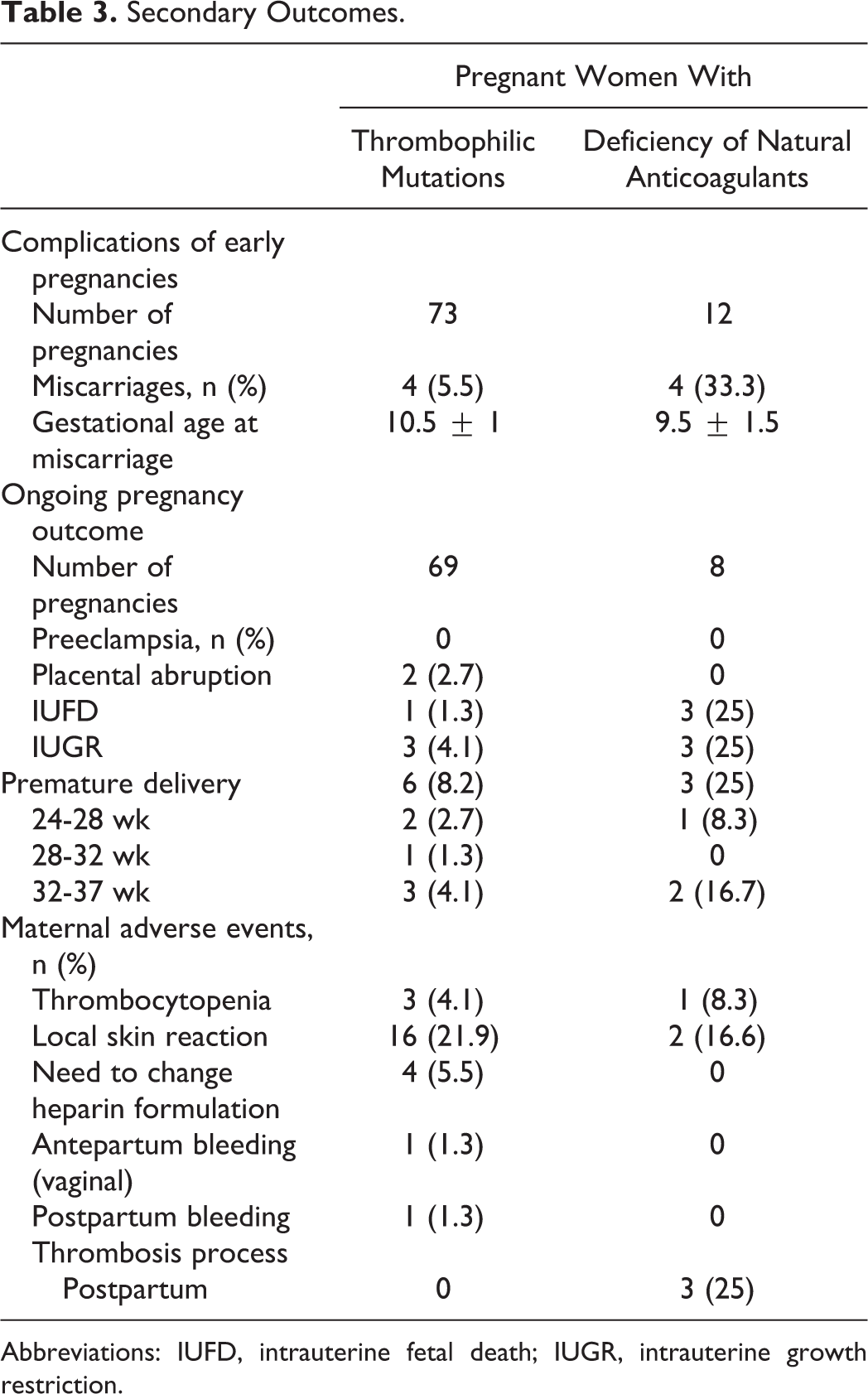
Abbreviations: IUFD, intrauterine fetal death; IUGR, intrauterine growth restriction.
Obstetrical History in Women With Natural Anticoagulants Deficiency.
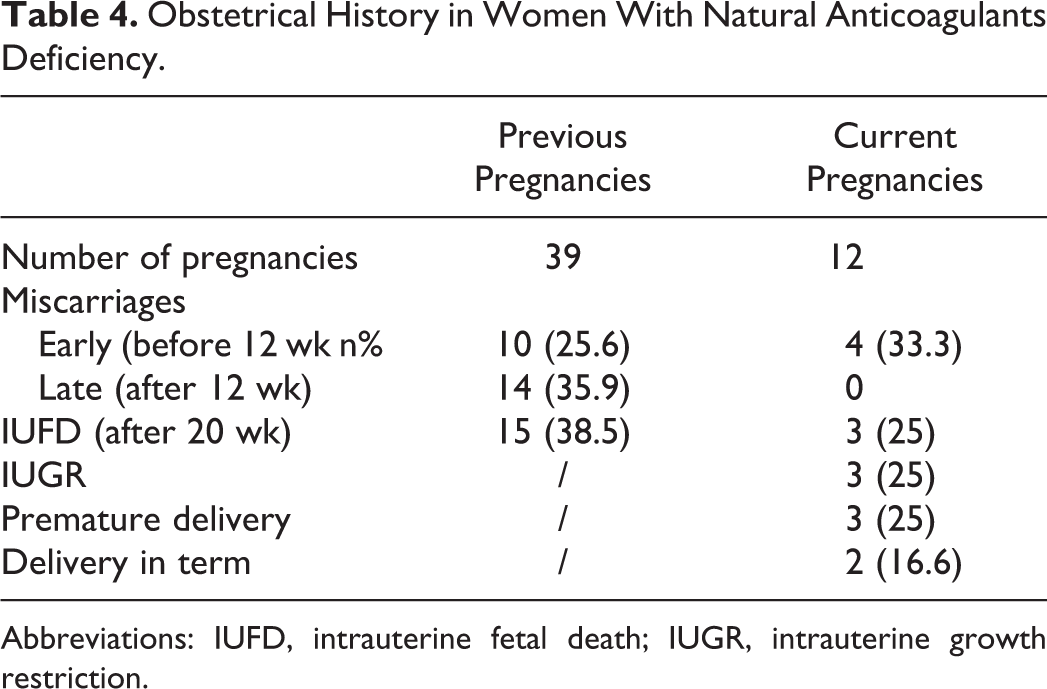
Abbreviations: IUFD, intrauterine fetal death; IUGR, intrauterine growth restriction.
D-dimer (ng/mL) in Pregnant Women Regarding the Type of Thrombophilia.a,b
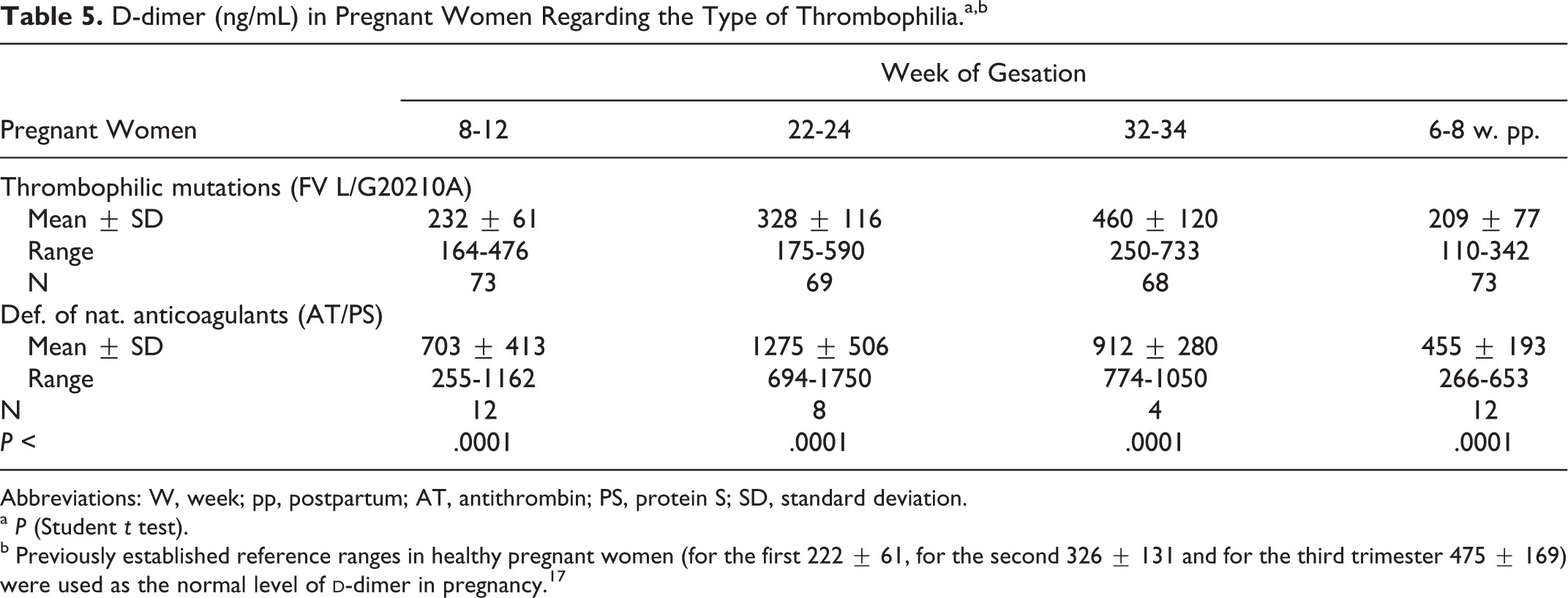
Abbreviations: W, week; pp, postpartum; AT, antithrombin; PS, protein S; SD, standard deviation.
a P (Student t test).
b Previously established reference ranges in healthy pregnant women (for the first 222 ± 61, for the second 326 ± 131 and for the third trimester 475 ± 169) were used as the normal level of
Discussion
The live birth rate of 85.8% observed in our study group of women with thrombophilia receiving treatment is consistent with the previously reported rates ranging from 75% to 85%. 10,11,20,21 Analysis of primary pregnancy outcomes regarding specific thrombophilic disorders showed that women carriers of mutations had a high live birth rate of 93%, while in the group of women with a deficiency of natural anticoagulants it was much lower, indicating that specific thrombophilic disorders have an impact on the live birth rate. Although the probability of pregnancy loss seems to decrease significantly upon LMWH, which was confirmed by the results obtained in women with mutations, pregnant women with a deficiency of natural anticoagulants, and a history of RFL remained at increased risk for a new pregnancy loss despite LMWH treatment. The secondary outcomes of pregnancies strongly supported this finding considering that 33.3% of women deficient in natural anticoagulants had early fetal loss, while 25% of their pregnancies ended as IUFD. Among 5 women whose pregnancies resulted in a live birth, 3 of them delivered preterm, mainly due to IUGR. In contrast, the rate of pregnancy complications was significantly lower in the group with mutations. In comparison to the other studies involving women with a deficiency of natural anticoagulants, the lowest live birth rate was observed in our study. We would like to point out that our patients with this type of thrombophilia had an average of more than 3 RFL and no previous successful pregnancies. In some studies asymptomatic pregnant women with natural anticoagulant deficiency were too included, 22,23 which could have had a possible influence on the live birth rate. In the retrospective study of Grandone et al, the live birth rate of women with PS deficiency before referral was 24% and under treatment it was 66%, while in the study of Gris et al the latter was even 79%. 24,12 In contrast, Carp et al showed that in women with a natural anticoagulant deficiency the live birth rate was 66.7% in the case of PS deficiency and 50% for AT deficiency, while in untreated pregnancies it was 50% for PS deficiency and 40% for AT deficiency, indicating no significant advantage associated with the treatment. 11
Our second very important finding was the high rate of hemostatic activity, measured by
One of the limitations of our study is the difference in sample size between the groups of patients. The relatively small sample size of the group with deficiencies of natural anticoagulants is due to their low prevalence in the general population. Consequently, during evaluation of current pregnancy outcomes, descriptive statistical methods were used as a more appropriate method of analysis. In this respect, our investigation should be considered as a pilot study, whose observations should be confirmed in a large controlled randomized clinical trial.
In conclusion, although the probability of pregnancy loss seems to decrease significantly upon LMWH, pregnant women deficient in natural anticoagulants and with a history of RFL remain with an increased risk of a new pregnancy loss despite LMWH treatment. Moreover, optimal therapy for women with low levels of natural anticoagulants and with RFL remains unclear. A future prospective study with a large number of patients is required to determine the optimal treatment of these severe thrombophilic conditions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: grant 173008 from Ministry of Education, Science and Technological Development, Serbia.