
Abstract
Some now recommend a lung scan if the plain chest radiograph is normal instead of computed tomographic (CT) angiography to minimize the risks of radiation in younger patients with suspected pulmonary embolism. The purpose of this investigation is to determine practice standards according to age and gender in regard to noninvasive imaging. Data are from the Nationwide Inpatient Patient, 1998 to 2009. In 2006 to 2009, the proportion of females with pulmonary embolism imaged with CT angiography was 275 (90%) of 305 among teenagers and girls, 3990 (87%) of 4570 among women 20 to 40 years, and 25 650 (85%) of 30 160 among women >40 years. Among males the proportion imaged with CT angiography was 175 (92%) of 190 among teenagers and boys, 3000 (89%) of 3370 among men 20 to 40 years, and 21 280 (86%) of 24 800 among men >40 years. In conclusion, contrary to the recommendations of some, CT angiography is usually obtained in young patients.
Introduction
Recognizing the difficulty in diagnosing pulmonary embolism, physicians now liberally use computed tomographic (CT) pulmonary angiography in patients with suspected pulmonary embolism. 1 Coincident with the increased use of CT angiography, the use of ventilation/perfusion lung scans has decreased. 1 Among 1903 patients with suspected acute pulmonary embolism, the prevalence of a positive test on 64-detector CT angiography was 10.8%. 2 Others reported a prevalence positive CT angiograms of 5% to 10%. 3 A disadvantage of CT angiography is exposure to ionizing radiation.
Ventilation-perfusion lung scans or perfusion lung scans alone were shown to be diagnostic in 89% to 91% of patients with suspected pulmonary embolism who had a normal chest radiograph. 4,5 It would seem reasonable, therefore, to select a lung scan as the first imaging test in patients at high risk of radiation-induced cancer, children, and young adults, if the plain chest radiograph is normal. This was the Consensus Group recommendation in 2011 of investigators who published in the field of pulmonary embolism, 6 and the recommendation by Moores et al 7 in 2011 for all patients with suspected pulmonary embolism who have a normal chest radiograph. If available, ventilation-perfusion single-photon–emission computed tomography (SPECT) has been recommended as the initial imaging test for premenopausal women with suspected pulmonary embolism. 8 Some, however, recommended ventilation-perfusion scintigraphy only if there is a contraindication for CT pulmonary angiography. 9 The current practice with regard to diagnostic testing is not known. The purpose of the present investigation, therefore, is to determine usual practice in the United States, according to age and gender with regard to noninvasive imaging for suspected acute pulmonary embolism.
Methods
Patients with acute pulmonary embolism discharged from short-stay hospitals throughout the United States from 1998 through 2009 and the method of diagnostic imaging were identified from the Nationwide Inpatient Sample (NIS), Healthcare Cost and Utilization Project (HCUP), and Agency for Healthcare Research and Quality (AHRQ). 10 The NIS contains data from 5 to 8 million hospital stays from about 1000 hospitals and is designed to approximate a 20% sample of US nonfederal, short-term hospitals.
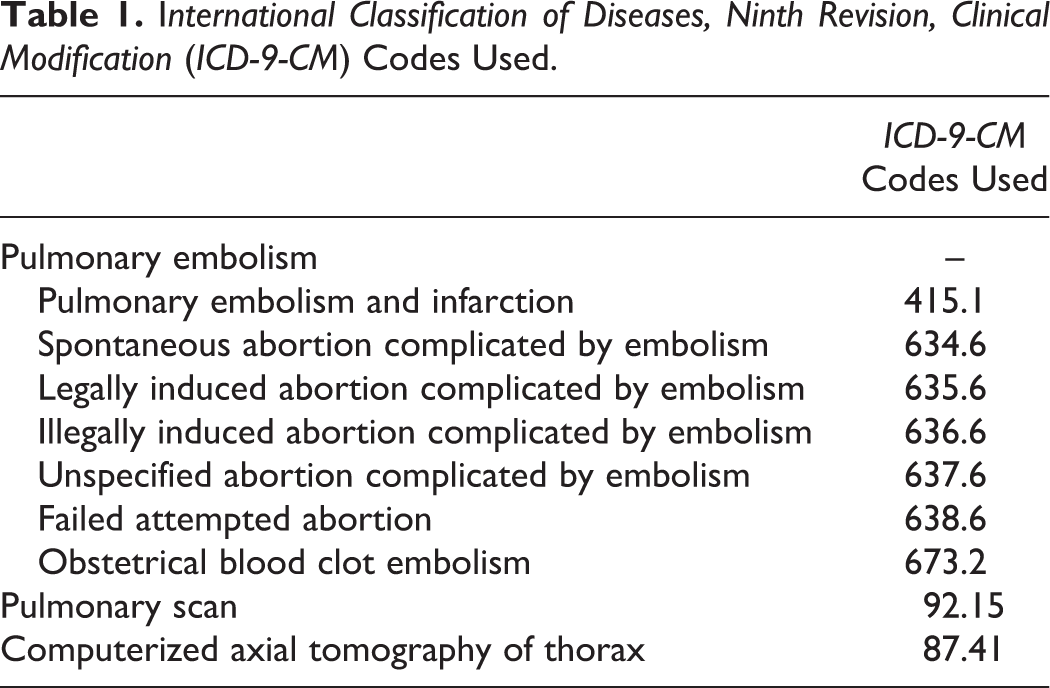
International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes were used to identify patients with pulmonary embolism, and the noninvasive imaging tests were also used (Table 1). We interpreted a procedure code for a pulmonary radioisotope scan in patients with pulmonary embolism to be either a ventilation-perfusion lung scan or a perfusion lung scan. We interpreted a procedure code for computerized axial tomography of the thorax in patients with pulmonary embolism to be a CT pulmonary angiogram.
International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) Codes Used.
Statistical Methods
We identified patients with pulmonary embolism who had a procedure code for CT angiography or a pulmonary radionuclear scan. Only 6.5% of patients with pulmonary embolism had a procedure code for these diagnostic tests. Our data show the proportion of patients with pulmonary embolism who had a CT pulmonary angiogram or pulmonary scintigram among those who had a procedure code for one of these tests. The proportion of tests with CT angiography compared to scintigraphy was determined according to sex and age. Differences in use were assessed by chi-square. Chi-square and 95% confidence intervals (CIs) were calculated using GraphPad Software (San Diego, California).
Results
In the 12-year period of investigation, imaging with CT angiography increased to 89% in patients with pulmonary embolism and imaging with scintigraphy decreased to 11% (Figure 1). The proportion of patients imaged by CT pulmonary angiography peaked in 2009.
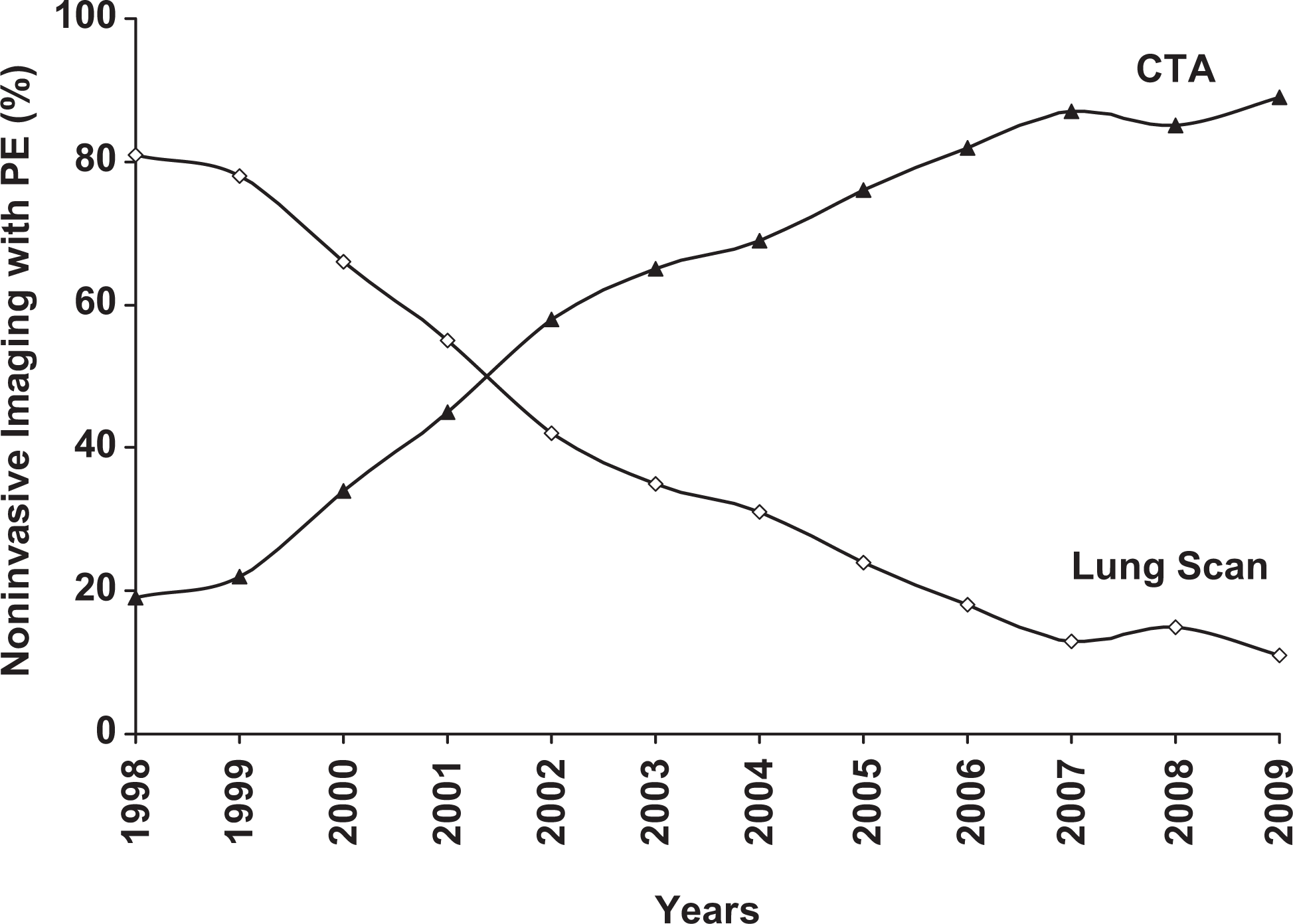
Proportion of patients with pulmonary embolism (PE) diagnosed by computed tomographic pulmonary angiography (CTA) and by lung scans according to 1998 to 2009.
Among female teenagers and girls, the proportion with pulmonary embolism who were imaged with CT angiography from 2006 to 2009 was higher than among women >40 years of age (P < .01; Table 2, Figure 2). The proportion of women aged 20 to 40 years who were imaged with CT angiography from 2006 to 2009 was also higher than the proportion of women >40 years of age (P < .0001; Table 2, Figure 2).
Proportion Diagnosed by Computed Tomographic Pulmonary Angiography and by Lung Scans in Patients With Pulmonary Embolism, 2006 to 2009.
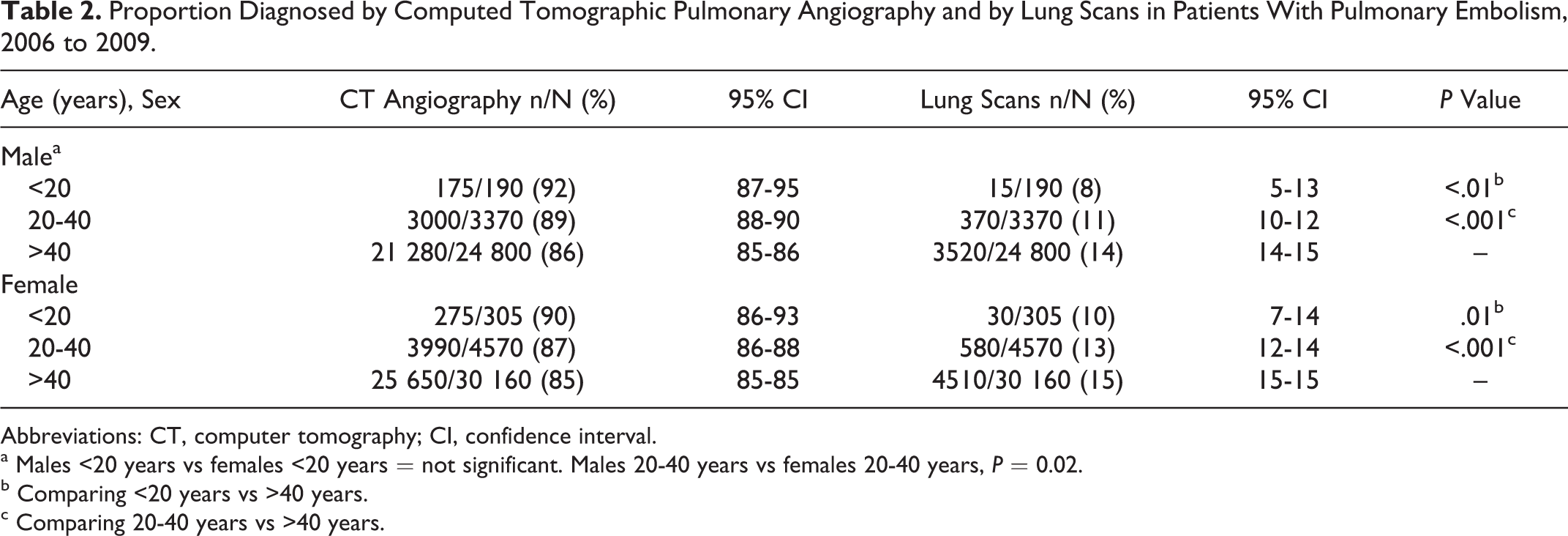
Abbreviations: CT, computer tomography; CI, confidence interval.
a Males <20 years vs females <20 years = not significant. Males 20-40 years vs females 20-40 years, P = 0.02.
b Comparing <20 years vs >40 years.
c Comparing 20-40 years vs >40 years.
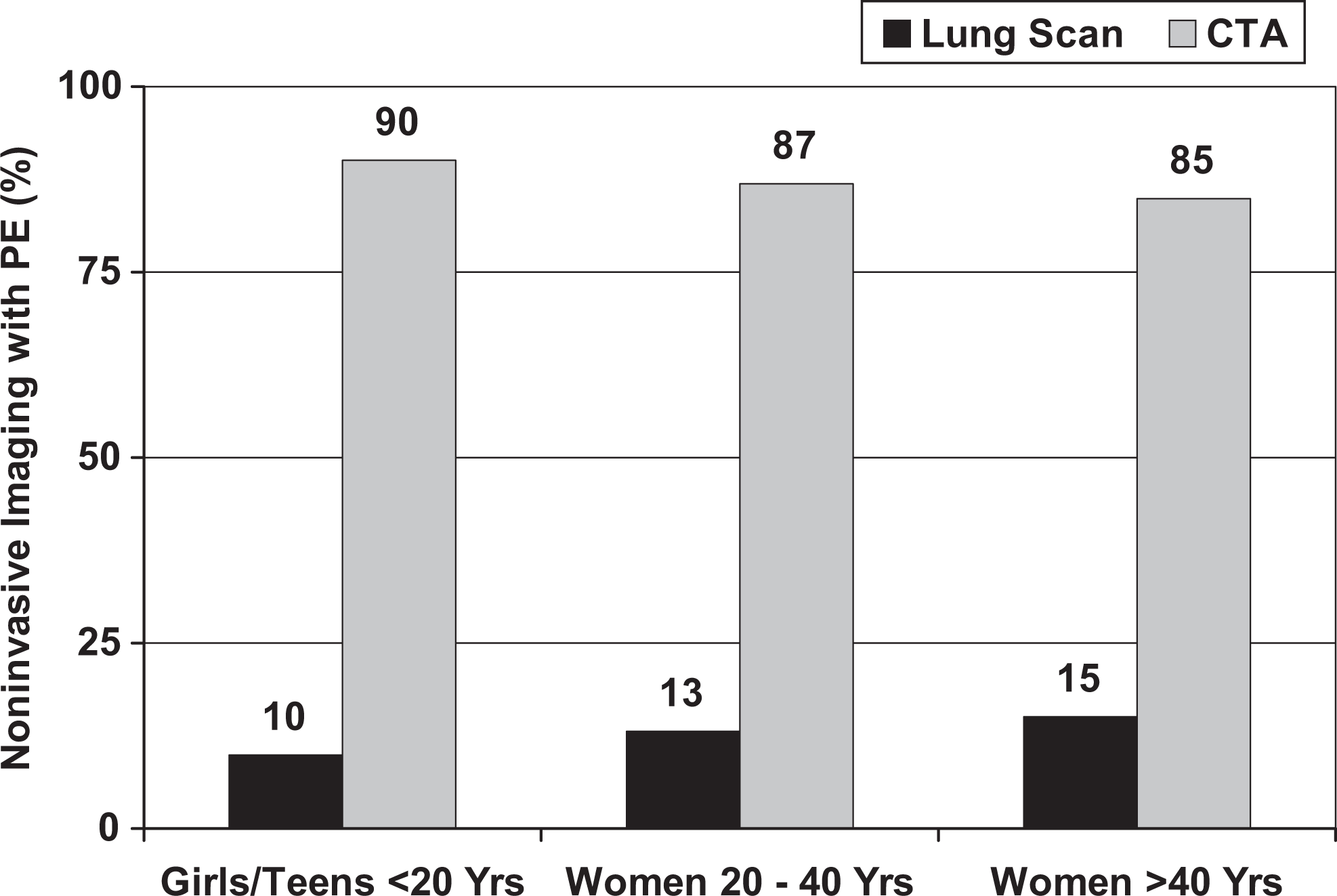
Proportion of girls and women with pulmonary embolism (PE) diagnosed in 2006 to 2009 by computed tomographic pulmonary angiography (CTA) and by lung scans according to age.
The proportion of male teenagers and boys with pulmonary embolism who were imaged with CT angiography from 2006 to 2009 was higher than the proportion of men >40 years of age (P < .01; Table 2, Figure 3). The proportion of men aged 20 to 40 years who were imaged with CT angiography from 2006 to 2009 was also higher than the proportion of men > 40 years of age (P < .0001; Table 2, Figure 3).
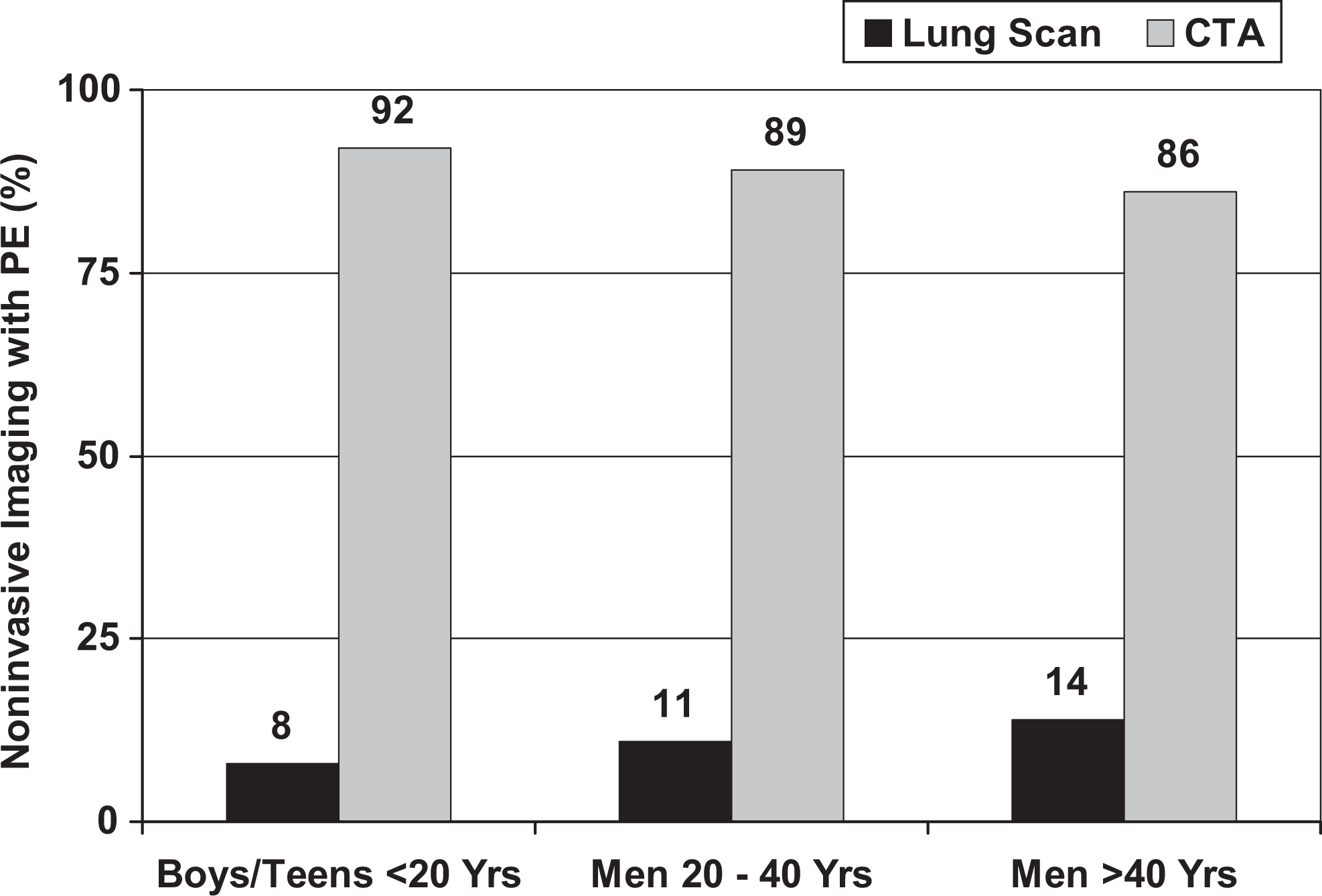
Proportion of boys and men with pulmonary embolism (PE) diagnosed in 2006 to 2009 by computed tomographic pulmonary angiography (CTA) and by lung scans according to age.
The proportion of male teenagers and boys imaged with CT angiography did not differ significantly from that of female teenagers and girls (Table 2). The proportion of women aged 20 to 40 years who were imaged with CT pulmonary angiography was less than that of men aged 20 to 40 years (P = .02), but the difference was small and probably not clinically important (Table 2).
Discussion
The use of lung scans declined and the use of CT pulmonary angiography increased from 1998 to 2009. Among males and females (<20 years of age) with pulmonary embolism, the proportion of noninvasive imaging tests by CT pulmonary angiography during the 4 most recent years of data acquisition, 2006 to 2009, was 90% to 92%. The proportion of diagnostic imaging tests by CT angiography was higher in teenagers and children than that in patients >40 years of age. There was no evidence of a less frequent use of CT angiography in patients with high risk of radiation-induced cancer.
The effective (whole-body) dose of a CT pulmonary angiogram has been reported to range from 3 to 27 mSV, 11 but based on studies in a phantom, the effective dose of a 64-detector CT pulmonary angiogram may be as high as 12 to 32 mSV. 12 The effective dose of a 99mTc-macroaggregated albumin perfusion lung scan is 0.44 to 1.65 mSv, and a 133Xe ventilation scan is 0.14 to 0.53 mSv. 13 The lifetime attributable risk of cancer with CT imaging is higher in women than in men 14 and higher in younger patients than in older, 14,15 the highest risks being in young women. 14 It was estimated that 1300 to 5000 future cancers might have been caused by CT pulmonary angiography in 2007. 16
If pulmonary embolism cannot be excluded by a clinical/
If pulmonary embolism cannot be excluded by a clinical/
Strengths of this investigation are the large number of patients, which permitted stratification according to age and gender. Coding for pulmonary embolism is sensitive. Review of Medicare hospitalizations showed that 92% of codable cases for pulmonary embolism were on the abstract. 18 A 0.4% prevalence of pulmonary embolism in hospitalized patients >20 years of age throughout the United States, based on data from the National Hospital Discharge Survey 19 , was similar or the same as the prevalences in individual investigations, 0.3% to 0.4%. 20 –22
Weaknesses include a low sensitivity of procedure codes for CT angiography and pulmonary scintigraphy. From 1998 to 2009, only 6.5% of patients with pulmonary embolism had a listed procedure code for either CT angiography or a radionuclear scan. Our data are from these patients. We assumed that the sensitivity for coding, although low, did not change over the period of investigation and the sensitivity of coding was similar among all age groups and both sexes. We also assumed that the sensitivity of coding pulmonary scintigraphy and CT angiography were similar. If the sensitivity of coding of pulmonary scintigraphy and CT angiography were dissimilar, the proportion of tests comparing CT angiography to lung scans would be changed, but relative differences in the use of CT angiography according to age would not be affected.
Another weakness is that the data did not permit analysis of serial noninvasive leg tests. Coding did not distinguish between a single venous ultrasound test of the lower extremities and serial venous ultrasound examinations. Also, among patients with pulmonary embolism who had no code for CT angiography or pulmonary scintigraphy, it was not possible to determine whether venous ultrasound was performed instead of lung imaging or in addition, although lung imaging was not coded. Finally, procedure codes did not distinguish between ventilation-perfusion lung scans and perfusion lung scans alone.
In conclusion, the proportion of CT pulmonary angiograms obtained in children and young women with pulmonary embolism was not lower than the proportion of CT pulmonary angiograms obtained in patients >40 years of age. Although consensus opinion by some is that children and young adults with a normal chest radiograph should be imaged with lung scans rather than CT angiography to minimize the risks of radiation, our data show that CT angiograms in the United States are not obtained less frequently in such patients.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.