
Abstract
We aimed to determine whether red cell distribution width (RDW) and mean platelet volume (MPV) values differ between patients with reactive amyloid A (AA) amyloidosis due to chronic inflammatory disease and in healthy participants. In this study, 33 patients with AA amyloidosis and 40 age- and sex-matched healthy controls were enrolled. Erythrocyte sedimentation rate (ESR), RDW, platelet count (PLT), and MPV levels were retrospectively obtained from our computerized patient database. We found RDW, ESR, and PLT levels to be significantly higher in patients with AA amyloidosis compared with the controls (P < .0001). Mean platelet volume was significantly lower in patients with amyloidosis (P < .0001). Inflammatory diseases such as AA amyloidosis may demonstrate low MPV and high RDW levels.
Introduction
The amyloidoses constitute a group of diseases characterized by extracellular tissue deposition of fibrils, composed of several low-molecular-weight protein subunits. 1 Amyloid A (AA) amyloidosis is a reactive type, usually secondary to chronic infectious and inflammatory disease (rheumatoid arthritis [RA], juvenile RA, other inflammatory arthritis, Crohn disease, familial Mediterranean fever [FMF], and other hereditary periodic fever syndromes). 1,2 Amyloidosis is a multisystemic disease, with varied manifestations in involved organs depending on the amount of amyloid fibrils deposited. Amyloid fibrils are most commonly deposited in the kidneys but may also involve the heart, peripheral nerves, thyroid, gastrointestinal system, and bone marrow. Heart and kidney involvement is the most important predictor of survival. 1
Red cell distribution width (RDW) is usually assessed as part of the hemogram and relates to variability in the size of circulating erythrocytes. 3 The first role for RDW is in the differential diagnosis of anemia and microcytosis. However, recent studies suggest that RDW is not a reliable index for differentiating microcytic anemias. 4 High levels of RDW are also closely associated with adverse cardiovascular outcomes in heart failure and coronary heart disease. 5,6 Moreover, RDW is predictive of mortality from all causes in patients aged 45 years or older. 7 The RDW data are valuable for prognostication in obstructive sleep apnea syndrome 3 and acute kidney injury patients in the intensive care unit. 8 The RDW may also be increased in chronic inflammation. 9
Platelet volume, a marker of platelet function and activation, is generally measured as mean platelet volume (MPV). 10 Mean platelet volume is helpful in discriminating between hyperdestructive thrombocytopenia, like idiopathic thrombocytopenic purpura and hypoproductive thrombocytopenia; MPV is higher in hyperdestructive thrombocytopenia. 11 An elevated MPV has been proposed as a cardiovascular risk factor and has been recognized as an independent risk factor for myocardial infarction and adverse cardiovascular events such as recurrent ischemia or death. 12,13 Low MPV levels could be present in high-grade inflammatory diseases such as active RA or attacks of FMF. 14
We aimed to determine whether RDW and MPV values differ between patients with reactive AA amyloidosis due to chronic inflammatory disease and healthy controls.
Methods
A total of 33 patients with reactive AA amyloidosis and 40 healthy controls were analyzed. Patients presented in the outpatient setting and were diagnosed with amyloid deposits on colon or renal biopsies. The underlying disorders in patients with AA amyloidosis included FMF (n = 22), RA (n = 3), ankylosing spondylitis ([AS]; n = 2), bronchiectasis (n = 1), and unknown causes (n = 5). There were no patients with diabetes mellitus, hypertension, chronic heart failure, asthma, chronic obstructive pulmonary disease, hematological malignancies, cirrhosis, portal hypertension, or malignancies; their estimated glomerular filtration rate was >70 mL/min per 1.73 m2. None of the patients with amyloidosis were on anticoagulant therapy. We included all patients with amyloidosis who did not meet any of the exclusion criteria. Age- and sex-matched healthy controls were chosen from renal transplant donor candidates.
The laboratory parameters of the patients with amyloidosis were recorded at diagnosis and prior to treatment. Patient laboratory data were collected from a computerized patient database and included erythrocyte sedimentation rate (ESR), white blood cell count (WBC), platelet count (PLT), MPV, RDW, serum fasting glucose, serum creatinine, total cholesterol, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, triglyceride levels, and 24-hour urine protein. Complete blood count analyses were performed using the same analyzer (Advia 2120i, Siemens). Standard tubes with constant amounts of ethylenediaminetetraacetic acid were used.
The Kolmogorov-Smirnov test was used to determine whether the continuous variables were normally distributed. Descriptive analyses were presented as means and standard deviations for normally distributed variables and as medians with interquartile ranges for nonnormally distributed variables. The Student t test or Mann-Whitney U test were used to compare groups, with the chi-square test used for categorical variables. A P value of less than .05 was considered statistically significant.
Results
Table 1 shows the demographic features and laboratory results of the patients with amyloidosis and control groups. Age and gender were similar in both the patient and control groups (P > .05). There was no difference in serum fasting glucose and creatinine between patients with amyloidosis and controls. Patients with amyloidosis had lower serum albumin and significant proteinuria; they also had lower MPV levels (P < .0001) and higher RDW (P < .0001) and ESR (P < .0001; Table 1).
Patient Demographics.a
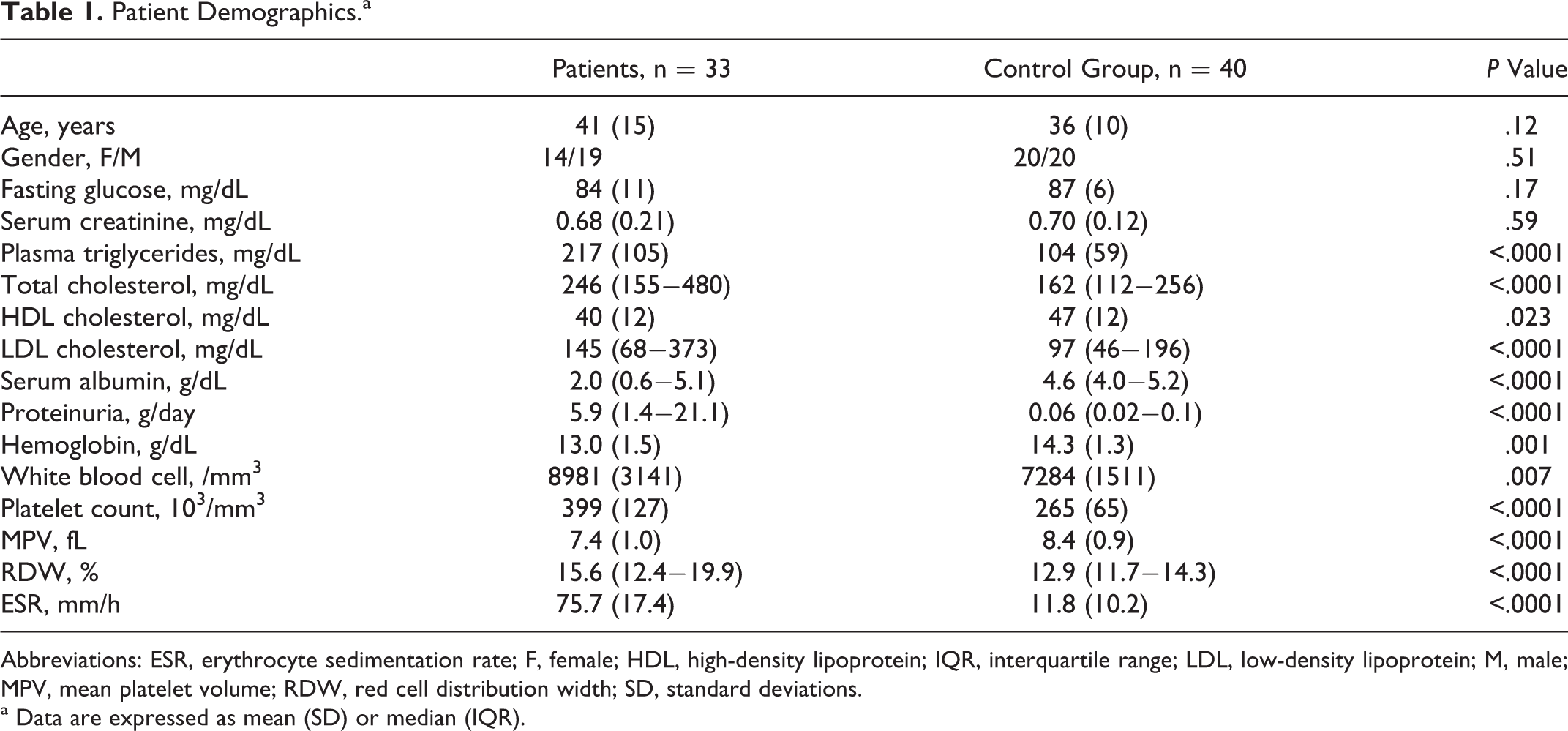
Abbreviations: ESR, erythrocyte sedimentation rate; F, female; HDL, high-density lipoprotein; IQR, interquartile range; LDL, low-density lipoprotein; M, male; MPV, mean platelet volume; RDW, red cell distribution width; SD, standard deviations.
a Data are expressed as mean (SD) or median (IQR).
Discussion
Many studies have investigated the association of RDW and MPV with cardiovascular and other diseases. 3,5,6,8,9,12 –14 However, to our knowledge, RDW and MPW have not been studied in relation to amyloidosis. The present study demonstrates that patients with an inflammatory condition, such as reactive systemic AA amyloidosis, have higher RDW and lower MPV.
The RDW reflects the variability in the size of circulating red cells (anisocytosis). It is elevated in conditions of ineffective red cell production, increased red cell destruction, and following blood transfusion. Thus, an elevated RDW indicates heterogeneity in the cell size of the peripheral blood smear. 8,15 The RDW is significantly associated with increased risk of adverse outcomes in patients with heart failure and coronary heart disease. 5,6 It is also a strong predictor of mortality in adults aged 45 years or older. 7 Higher RDW values are strongly correlated with higher systolic and diastolic blood pressures 16 and are associated with increased cardiovascular disease and nephropathy in patients with diabetes mellitus. 17 The RDW may be a predictor of mortality from all causes, in patients with acute renal failure in the intensive care unit. 8 It may also be increased due to chronic inflammation. 9
In our study, we found the RDW levels to be higher in patients with amyloidosis, compared with the healthy controls. The patients with amyloidosis did not have diabetes mellitus, hypertension, or renal failure, which could explain the elevated RDW. Some studies have reported a correlation between RDW and both ESR and C-reactive protein (CRP). Red cell distribution width increases during inflammation, similar to the increase seen in other inflammatory parameters, suggesting that RDW may be increased due to chronic inflammation. 18,19 Förhécz reported that acute phase-reactant CRP was highly significant, positively correlating with RDW. For negative acute-phase reactant prealbumin, a strong negative correlation was observed in the highest RDW group consisting of patients with heart failure. 19 Lippi showed a strong, graded association of RDW with CRP and ESR in a large cohort of unselected adult outpatients. 9 Being an inflammatory disease, 1 amyloidosis could cause increased RDW levels. Also, PLT, WBC, and ESR in patients with amyloidosis were higher than in controls, which may be the result of inflammation.
Platelets are heterogeneous in size and density. Mean platelet volume, the most commonly used measure of platelet size, is a potential marker of platelet reactivity. Larger platelets are metabolically and enzymatically more active and have greater prothombotic potential. Elevation in MPV is associated with other markers of platelet activity, including increased platelet aggregation, increased thromboxane synthesis and b-thromboglobulin release, and increased expression of adhesion molecules. 20 An elevated MPV is a cardiovascular risk factor that is associated with adverse cardiovascular events. 20 In contrast to the association found between MPV and myocardial infarction, there was no association found between MPV and stroke outcome or stroke severity. There may be several reasons for this. First, different automated cell counters were used in the studies. Second, the time of MPV measurement varied between the studies, ranging from admission to 48 hours after the onset of the events. 21 Furthermore, a higher MPV is observed in patients with diabetes mellitus, 22 impaired fasting glucose, 23 hypertension, 24 hypercholesterolemia, 25 obesity, 26 and smoking. 27 Low MPV levels may be present in high-grade inflammatory diseases. 14
In this study, MPV levels were lower in patients with amyloidosis compared to healthy individuals. High-grade inflammatory diseases, such as active RA or active FMF, present with low levels of MPV. 14 Makay reported that MPV was significantly lower in patients with FMF during attacks than in attack-free periods. On the other hand, CRP and ESR levels were higher during an attack. 28 Kisacik demonstrated that MPV was significantly lower in active AS and RA. 29 Kapsoritakis found that MPV was significantly reduced in active versus inactive inflammatory bowel disease. 30 Thus, MPV levels can be decreased because of inflammation.
Interleukin 6 (IL-6) is an important proinflammatory cytokine that can induce thrombocytosis and also affect platelet volume. Administration of IL-6 was shown to cause an increase in platelet number, accompanied by a significant fall in MPV in patients with cancer. 31 Reactive systemic AA amyloidosis is characterized by increased production of serum AA protein (SAA), an acute phase protein produced in response to inflammation. 1,2 Serum AA is produced by inflammatory signals, IL-1β, tumor necrosis factor-α, and IL-6. 1 This can explain the higher PLT and lower MPV observed in patients with amyloidosis.
Our study has certain limitations. Because of its retrospective design, the initial CRP of the patients with amyloidosis at the diagnosis could not be established completely. Thus, we could not compare the relationship of CRP with RDW and MPV. It may be useful to investigate the relation of SAA and IL-6 with MPV and RDW in patients with amyloidosis, which was not evaluated in this study.
In conclusion, this study found RDW to be higher and MPV to be lower in patients with AA amyloidosis compared to the healthy controls. Although high RDW and low MPV levels are correlated with chronic inflammation, this relationship has not been thoroughly examined in AA amyloidosis, an inflammatory condition that may demonstrate these findings.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.