
Abstract
Recent or continued immobility is a significant risk factor for venous thromboembolism (VTE) in acutely ill medical patients. Patients may benefit from thromboprophylaxis; however, its optimal duration remains unclear. The Extended Clinical Prophylaxis in Acutely Ill Medical Patients (EXCLAIM) study was the first trial to systematically investigate how the degree of immobilization relates to the risk of developing VTE. EXCLAIM offers insights into the duration of VTE risk associated with reduced mobility and helps identify which patients would benefit most from extended-duration thromboprophylaxis. Further recent studies suggest that extended-duration thromboprophylaxis may be in order in certain high-risk patients to protect the patients from the risk of VTE events occurring, particularly in the posthospitalization period. Baseline
Introduction
Immobility or reduced independent mobility is an important and highly prevalent risk factor for venous thromboembolism (VTE)—both deep vein thrombosis (DVT) and pulmonary embolism (PE).1 –4 A sustained period of immobility leads to vascular stasis, one of the cornerstones of Virchow’s triad in the pathology of thrombosis.5,6
Immobility in Surgical Patients
In surgical patients, the risk of VTE associated with immobilization is well recognized. However, limited data are available that quantify the level of risk conferred by immobility in these patients.7,8 Postoperative immobility is an inherent consequence of the surgery itself and, therefore, it is difficult to separate the relative contributions of surgery and immobility as they are not strictly independent variables. Nevertheless, the importance of immobility in VTE is understood and early mobilization postsurgery in addition to anticoagulant therapy is a key strategy for reducing VTE incidence.7,8 Historically, a 10-day course of thromboprophylaxis was recommended in high-risk surgical patients. 9 However, studies have indicated that extending the duration of thromboprophylaxis up to 35 days can further reduce the incidence of VTE in high-risk surgical patients, such as those undergoing hip replacement or major abdominal surgery.10–12 Therefore, the latest (2012) guidelines from the American College of Chest Physicians (ACCP) recommend prophylaxis beyond 10 days and up to 35 days in patients undergoing major orthopedic surgery, 8 and for 4 weeks for those undergoing abdominal or pelvic surgery for cancer. 7
Immobility in Medical Patients
Immobility is a well-recognized VTE risk factor not only in surgical patients, but also a potential risk factor in medical patients. Heit et al showed that patients previously confined to bed rest, whether in a hospital or nursing home, have an 8-fold increase in the odds of developing VTE complications (odds ratio [OR] 7.98; 95% confidence interval [CI] 4.49-14.1). 13 More recently, a meta-analysis of epidemiological studies identified a 2- to 3-fold increase in VTE risk in immobilized medical patients (overall OR 2.52; 95% CI 1.70-3.74; P < .001). 3 Medical patients often have a history of immobilization upon admission due to the morbidity associated with their presenting illness, or comorbid conditions for example, respiratory failure, heart failure (HF), advanced age, or obesity. 14 Furthermore, many elderly patients are likely to have reduced mobility, and these patients may also present with asymptomatic VTE upon admission to hospital (18% of patients aged >80 years). 15
As immobility in medical patients is not necessarily directly attributable to their presenting condition, it is easier to assess immobility as an independent variable and determine how the degree of immobility can contribute to the magnitude of the VTE risk. Although the major clinical trials of VTE prophylaxis in medical patients have included definitions of immobility in their inclusion criteria, few specifically investigated the effects of immobility on VTE risk per se, or whether immobilized medical patients would benefit from extended-duration thromboprophylaxis.
This review examines the differing definitions of immobility used in studies of medical patients and the effect of VTE prophylaxis on outcomes in patients with recent or ongoing immobility. This will lead to a discussion on the optimum duration of thromboprophylaxis in medical patients with reduced mobility.
Definitions of Immobility in Clinical Trials of VTE Prophylaxis in Medical Patients
Many trials and registries of hospitalized medical patients have defined immobility in their enrollment criteria. However, there are numerous ways of defining immobility. For example, immobility could be classified as a dichotomous variable (mobile or immobile), or using different levels (partial or severe), although the exact criteria used to delineate these 2 levels should be clearly defined and enforced. Also, there are other factors that need to be taken into consideration such as the time period over which immobility is assessed. Many of the trials and registries that included “immobilized” medical patients used definitions that are specific to each individual study (Table 1).16 –28
Definitions of Immobility and Their Duration Across Studies in Acutely Ill Medical Patients With Restricted Mobility.
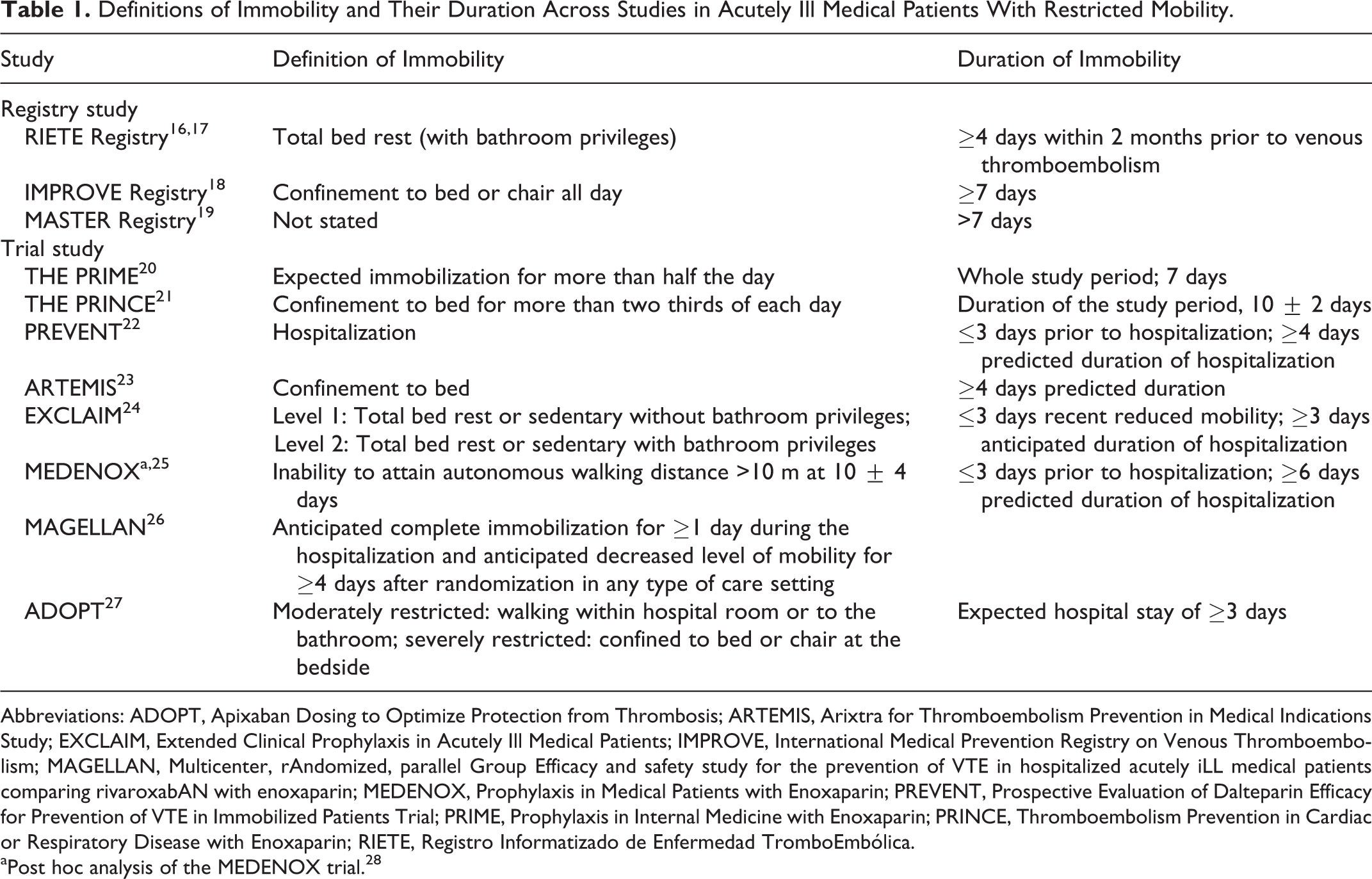
Abbreviations: ADOPT, Apixaban Dosing to Optimize Protection from Thrombosis; ARTEMIS, Arixtra for Thromboembolism Prevention in Medical Indications Study; EXCLAIM, Extended Clinical Prophylaxis in Acutely Ill Medical Patients; IMPROVE, International Medical Prevention Registry on Venous Thromboembolism; MAGELLAN, Multicenter, rAndomized, parallel Group Efficacy and safety study for the prevention of VTE in hospitalized acutely iLL medical patients comparing rivaroxabAN with enoxaparin; MEDENOX, Prophylaxis in Medical Patients with Enoxaparin; PREVENT, Prospective Evaluation of Dalteparin Efficacy for Prevention of VTE in Immobilized Patients Trial; PRIME, Prophylaxis in Internal Medicine with Enoxaparin; PRINCE, Thromboembolism Prevention in Cardiac or Respiratory Disease with Enoxaparin; RIETE, Registro Informatizado de Enfermedad TromboEmbólica.
aPost hoc analysis of the MEDENOX trial. 28
Differences in Definitions
For example, in the Thromboembolism Prevention in Cardiac or Respiratory Disease with Enoxaparin (PRINCE) study, which compared enoxaparin and unfractionated heparin use in hospitalized medical patients, immobility was defined as “confinement to bed for more than two-thirds of each day” during the study period. 21 In contrast, other studies focused principally on specifying its duration rather than describing the nature of the immobility. For example, The Prophylaxis in Medical Patients with Enoxaparin (MEDENOX) study specified that only patients who had ≤3 days of immobilization prior to hospital enrollment and who were predicted to spend ≥6 days in hospital were included, although this study did not initially qualify what constituted “immobilization.” 28 Thus it appeared that the definition of immobility could have been interpreted as “hospitalization.” However, a post hoc analysis of the MEDENOX study population defined nonambulatory patients as those unable to attain an autonomous walking distance of >10 m at the end of the treatment period (day 10 ± 4). 25 The Extended Clinical Prophylaxis in Acutely Ill Medical Patients (EXCLAIM) study was designed to evaluate the efficacy and safety of extended prophylaxis with enoxaparin (40 mg once daily for 28 ± 4 days) compared with placebo after an initial standard enoxaparin regimen (40 mg once daily for 10 ± 4 days), in acutely ill medical patients with recent reduced mobility.24,29 The EXCLAIM eligibility criteria specify a history of recent reduced mobility of up to 3 days, and an anticipated period of reduced mobility of at least 3 days with either a prespecified medical or intrinsic risk factor (Table 2). 24 Patients were classified as either level 1 (total bed rest or sedentary without bathroom privileges) or level 2 (total bed rest or sedentary with bathroom privileges) mobility. Following a planned and blinded interim analysis for futility, the Data Safety Monitoring Board recommended that the steering committee change the enrollment criteria to refocus on patients with a high risk of VTE. The amended inclusion criteria were as above, except that level 2 mobility had to be accompanied by at least 1 of 3 other high-risk VTE factors: age over 75 years and/or prior VTE and/or diagnosed cancer.24,29 The EXCLAIM study is unique in that it is the first trial to prospectively delineate more than 1 level of immobility. This allowed investigators to determine whether the level of immobility is associated with an increased risk of VTE. Furthermore, by including a broad range of medical illnesses investigators were able to perform additional subgroup analysis to identify which patients would benefit most from extended-duration prophylaxis. The Apixaban Dosing to Optimize Protection from Thrombosis (ADOPT) trial also defined 2 levels of restricted mobility: moderate (walking around hospital room or to bathroom) and severe (confined to bed or chair at bedside). 27 The Multicenter, rAndomized, parallel Group Efficacy and safety study for the prevention of VTE in hospitalized acutely iLL medical patients comparing rivaroxabAN with enoxaparin (MAGELLAN) which evaluated the efficacy and safety of extended-duration prophylaxis included a definition of immobility that included both the type and duration of reduced mobility. 26 As an inclusion criterion, immobility was defined as complete confinement to bed or chair, with or without bathroom privileges, for more than 1 day during hospitalization with anticipated decreased mobility (bed or chair rest for more than half of daytime hours in any type of care setting) for 4 or more days with additional ongoing reduced mobility. 26
Final Eligibility Criteria for the EXCLAIM Study.a
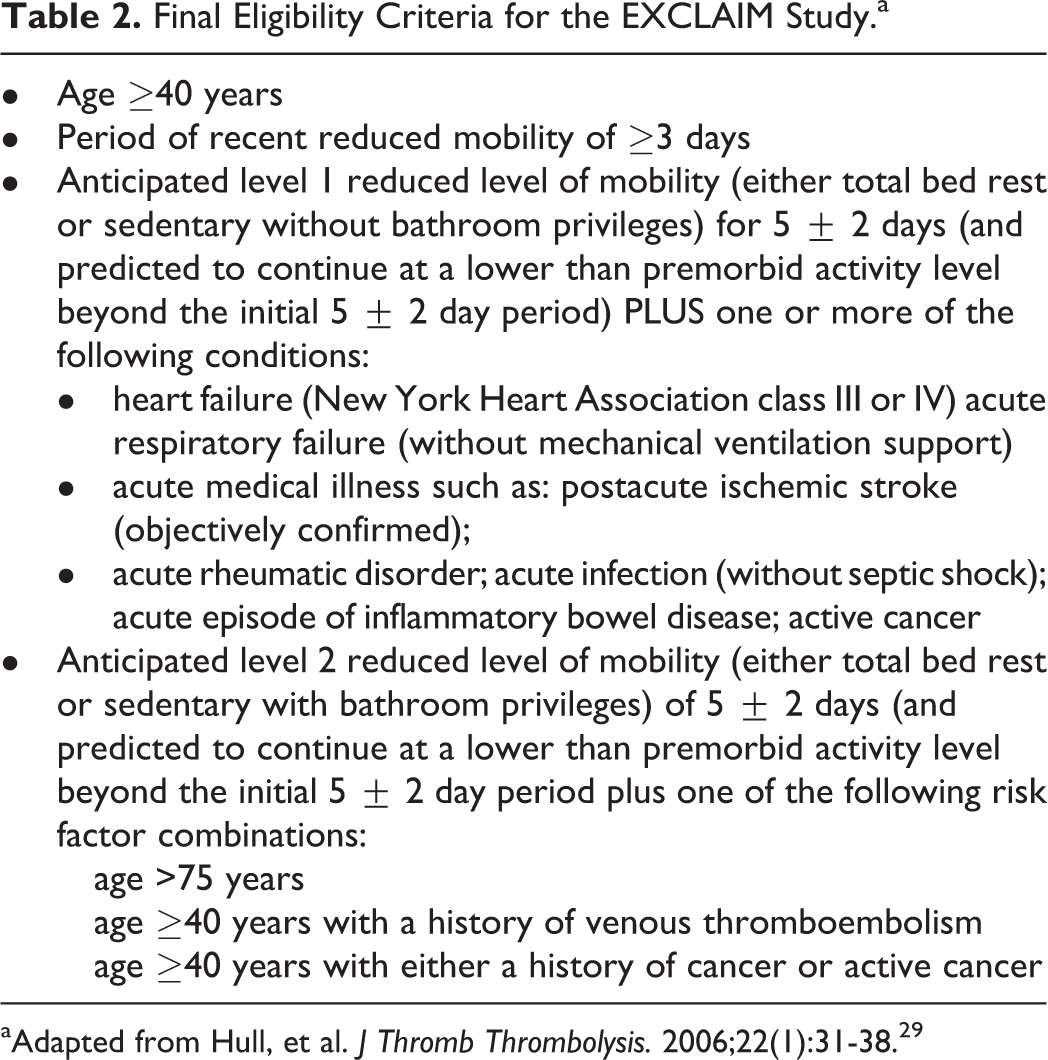
aAdapted from Hull, et al. J Thromb Thrombolysis. 2006;22(1):31-38. 29
Benefit of Prophylaxis in Medical Patients With Reduced Mobility
As many of the definitions used in trials of immobilized medical patients are both qualitatively and quantifiably different, drawing comparisons between the study outcomes is difficult. The key findings regarding mobility of the studies/registries are summarized in Table 3.20 –27,30 The Prospective Evaluation of Dalteparin Efficacy for Prevention of VTE in Immobilized Patients Trial (PREVENT) was designed to investigate the efficacy and safety of dalteparin in the prevention of VTE in acutely ill medical patients. 22 In patients who had been immobilized for at most 3 days prior to a predicted hospitalization-induced immobilization period of at least 4 days, dalteparin prophylaxis (5000 IU subcutaneously once daily) reduced the incidence of the primary composite outcome (objectively verified symptomatic DVT, symptomatic PE, asymptomatic proximal DVT, sudden death by day 21) to 2.8% (42 of 1518) versus 5.0% (73 of 1473) with placebo. This corresponded to a relative risk reduction (RRR) of 45% (relative risk [RR] 0.55; 95% Cl 0.38-0.80; P = .0015). The incidence of major bleeding was 0.5% with dalteparin and 0.2% with placebo (P = .15). 22 The Arixtra for Thromboembolism Prevention in Medical Indications Study (ARTEMIS) of prophylaxis in elderly (839 evaluable medical patients aged ≥60 years) acutely ill patients with immobility due to predicted bed rest of at least 4 days showed that prophylaxis with fondaparinux (2.5 mg once daily) almost halved the relative risk of VTE compared with patients who received placebo (RRR 46.7%; 95% Cl 7.7-69.3; P = .029), with minimal risk of major bleeding complications (1 patient [0.2%] in each group). 23 In the MEDENOX trial of hospitalized, acutely ill medical patients (a large proportion of whom had immobility due to their illness) thromboprophylaxis reduced the incidence of VTE from 14.9% (43 of 288) in patients treated with placebo to 5.5% (16 of 291) in those treated with enoxaparin (40 mg once daily), corresponding to a 63% risk reduction (RR 0.37; 97.6% CI 0.22-0.63; P < .001). 28 Major bleeding occurred in 2.0% of patients in the placebo group, 3.4% of patients treated with 40 mg enoxaparin, and 1.2% of patients receiving 20 mg enoxaparin. The recent subgroup analysis of MEDENOX data specifically investigating the impact of immobility (defined as the inability to walk >10 m unaided) on VTE risk reported an incidence of VTE of 19.7% (25 of 127) in nonambulatory patients compared with 10.6% (17 of 160) in ambulatory patients (RR 0.46; 95% CI 0.23-0.91; P = .02). 25 In nonambulatory patients, enoxaparin 40 mg once daily reduced the incidence of VTE to 9.0% (10 of 111), with no significant increase in the risk of major bleeding complications. 25
Further to these individual trials, a meta-analysis of trials in patients with immobilization of the lower extremity demonstrated that prophylaxis with a low-molecular-weight heparin (LMWH) resulted in a highly significant and clinically relevant reduction in the rates of asymptomatic VTE when compared with placebo or untreated controls, 31 with a relative risk of 0.58 (95% CI 0.39-0.86; P=.006). The difference in bleeding was not significant (RR 1.22; 95% CI 0.61-2.46; P = .57).
Other Factors to Influence Outcomes
Although the definitions of immobility vary among studies, there are also other differences such as composition of the study populations (eg, presenting conditions, age), study design and methodology, and the clinical interventions used (eg, prophylaxis strategies, regimens, ascertainment methods for VTE), all of which can impact the study outcomes. Moreover, many studies are underpowered to detect significant differences in the VTE rates among risk factor subgroups. Most major clinical trials have enrolled specific subgroups of patients at risk (eg, elderly patients and other high-risk groups), which hinders the extrapolation of their findings to heterogeneous populations of immobilized medical patients. For example, the MEDENOX 28 and PREVENT 22 studies had similar patient populations and defined both recent immobilization (≤3 days) and anticipated length of hospitalization, whereas ARTEMIS 23 included more elderly patients and did not specify the length of recent immobilization. Studies that enrolled specific types of medical patients (eg, cancer, recent stroke) also included patients with reduced mobility. It should be emphasized, however, that the effect of immobilization on outcomes is hard to isolate across all these studies without comparing the results to a treatment group of patients within the same study also diagnosed with the primary condition (eg, cancer), but who are independently mobile.
Outcomes of Thromboprophylaxis Studies in Acutely Ill Medical Patients With Reduced Mobility.
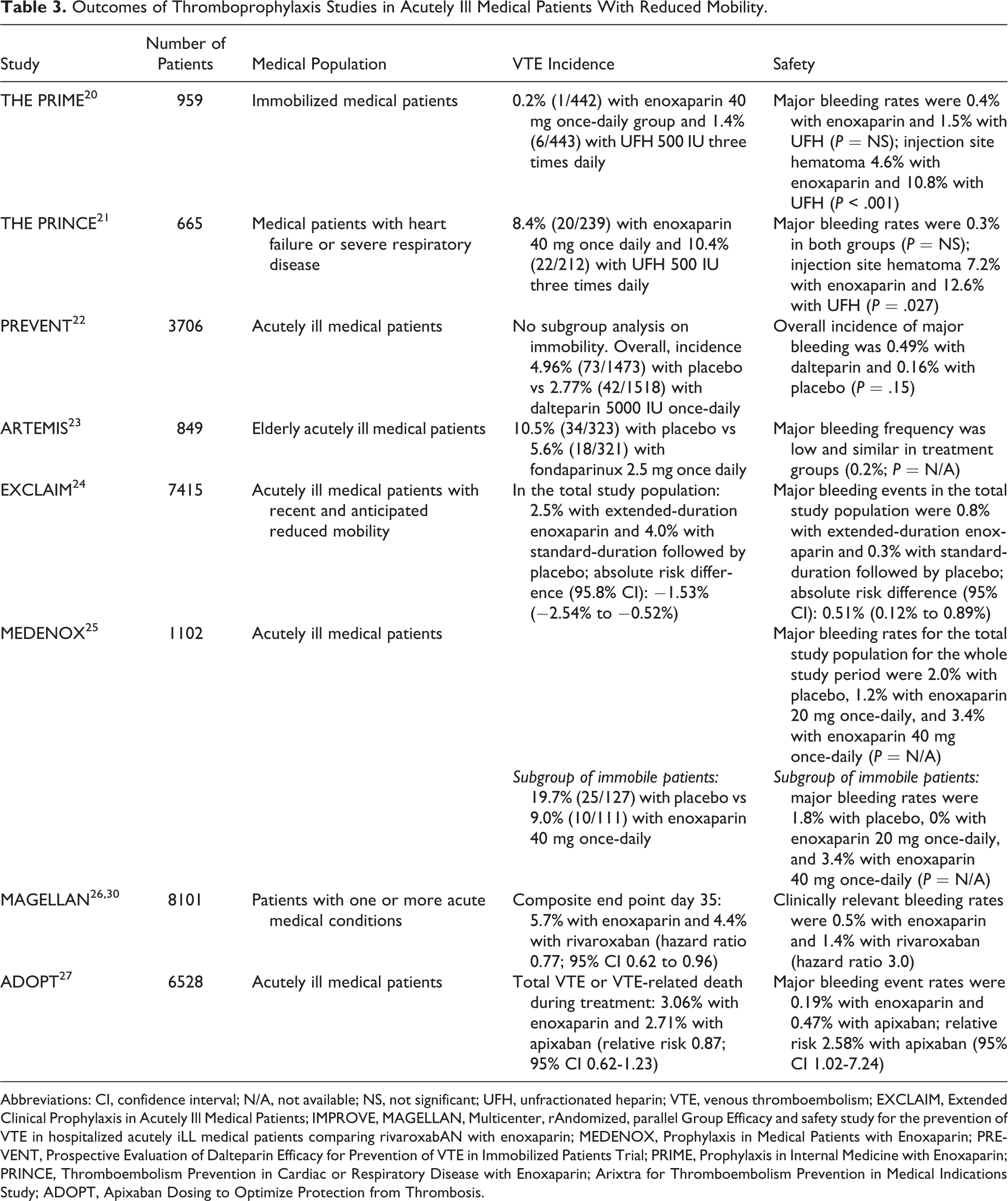
Abbreviations: CI, confidence interval; N/A, not available; NS, not significant; UFH, unfractionated heparin; VTE, venous thromboembolism; EXCLAIM, Extended Clinical Prophylaxis in Acutely Ill Medical Patients; IMPROVE, MAGELLAN, Multicenter, rAndomized, parallel Group Efficacy and safety study for the prevention of VTE in hospitalized acutely iLL medical patients comparing rivaroxabAN with enoxaparin; MEDENOX, Prophylaxis in Medical Patients with Enoxaparin; PREVENT, Prospective Evaluation of Dalteparin Efficacy for Prevention of VTE in Immobilized Patients Trial; PRIME, Prophylaxis in Internal Medicine with Enoxaparin; PRINCE, Thromboembolism Prevention in Cardiac or Respiratory Disease with Enoxaparin; Arixtra for Thromboembolism Prevention in Medical Indications Study; ADOPT, Apixaban Dosing to Optimize Protection from Thrombosis.
Optimal Duration of VTE Prophylaxis in Patients with Immobility
Without prophylaxis, acutely ill hospitalized medical patients develop VTE at a rate of about 5% to 20%.22,23,25,28 Although the need for VTE prophylaxis in this patient population is well established, the optimal duration of prophylaxis in these patients is less clear.1,14,32,33 Current guidelines from the ACCP, 14 and International Union of Angiology 32 recommend that acutely ill medical patients hospitalized with congestive HF or severe respiratory failure, or who are confined to bed and have one or more additional risk factors should receive VTE prophylaxis. Specifically, the 2012 ACCP guidelines state “For acutely ill hospitalized medical patients at increased risk of thrombosis, we recommend anticoagulant thromboprophylaxis with LMWH, low-dose unfractionated heparin 2 or 3 times-a-day, or fondaparinux and suggest against extending the duration of thromboprophylaxis beyond the period of patient immobilization or acute hospital stay.” 14 Similarly, there is broad international consensus that all hospitalized patients with cancer with reduced mobility should receive anticoagulant prophylaxis in the absence of bleeding contraindications.34,35 In its recent practice guideline, 33 the ACCP recommends assessing the risk of VTE and bleeding in hospitalized medical (including stroke) patients and then to provide pharmacologic prophylaxis with heparin or a related drug unless the bleeding risk outweighs the likely benefits, thus, emphasizing on risk assessment management (RAM) in medical patients and the balance of benefit and harm. However, the optimal duration of prophylaxis in medical patients with reduced mobility remains unknown and is not clearly specified within the guidelines.1,32 –35
Examination of the findings of key trials such as MEDENOX, PREVENT, and ARTEMIS reveals that many VTE events occur after the standard period of prophylaxis (6-14 days of duration), suggesting that current prophylaxis regimens may be too short.22,23,28 Table 4 summarizes the incidence of late VTE after discontinuation of prophylaxis in these studies.22,23,28,36
Incidence of Late Venous Thromboembolism (VTE) Events After Discontinuation of Prophylaxis in Hospitalized Medical Patients From MEDENOX, PREVENT, and ARTEMIS Trials.a
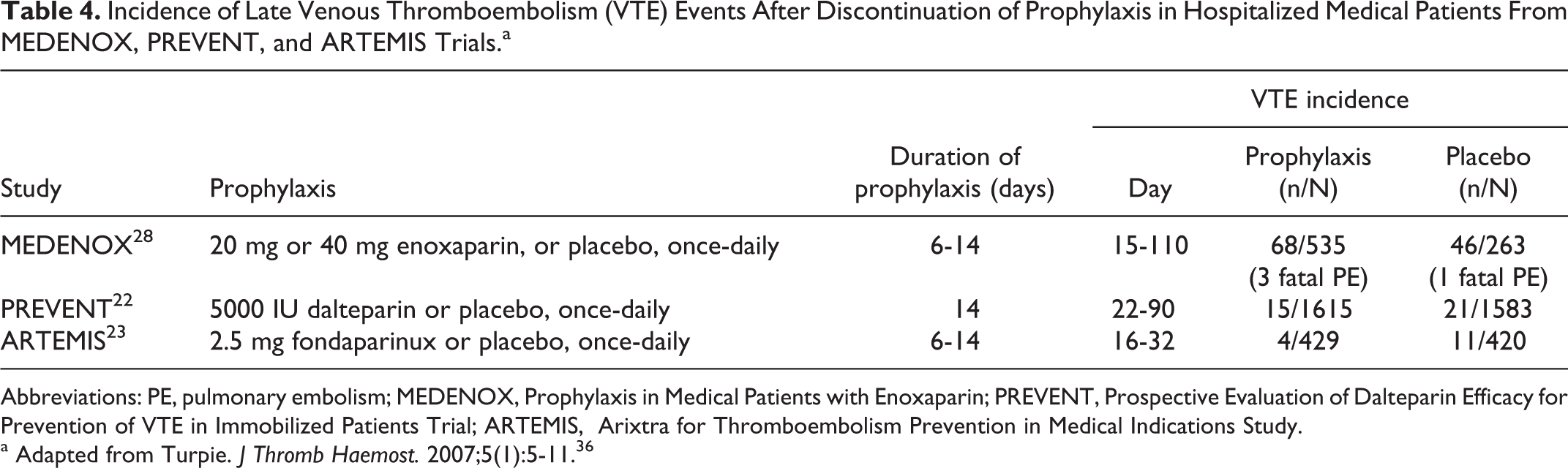
Abbreviations: PE, pulmonary embolism; MEDENOX, Prophylaxis in Medical Patients with Enoxaparin; PREVENT, Prospective Evaluation of Dalteparin Efficacy for Prevention of VTE in Immobilized Patients Trial; ARTEMIS, Arixtra for Thromboembolism Prevention in Medical Indications Study.
a Adapted from Turpie. J Thromb Haemost. 2007;5(1):5-11. 36
Extended-Duration Prophylaxis in Surgical Patients
In high-risk surgical patients, extended-duration prophylaxis has already been proven to be effective and well tolerated, reducing the risk of late VTE complications by up to 63% in major orthopedic surgery.10,36 –40 Meta-analyses of randomized controlled trials in hip and knee replacement surgery have confirmed that extended prophylaxis with a LMWH significantly reduced the risk of symptomatic VTE by 50% to 64% (ORs ranging from 0.36 to 0.50 in 2 meta-analyses and 2 systematic reviews) for up to 3 months postsurgery.10,11,41,42 Extended-duration prophylaxis has also been shown to reduce the incidence of asymptomatic VTE; in a meta-analysis of 9 studies in hip and knee replacement by Eikelboom et al, 11 the incidence of clinically silent, venographically detected DVT was reduced from 19.6% to 9.6% (OR 0.48; 95% CI 0.36-0.63). The reduction in VTE incidence is gained without increasing the risk of major bleeding complications, although the meta-analysis reported an increase in minor bleeding events from 2.5% to 3.7% (OR 1.56; 95% CI 1.08-2.26). 11 Extended-duration prophylaxis with fondaparinux has also been shown to be effective in reducing the risk of postoperative symptomatic VTE in patients undergoing hip fracture surgery from 2.7% (placebo group) to 0.3%, although a nonsignificant increase in major bleeding was observed in the fondaparinux group. 43
Extended-Duration Prophylaxis in Medical Patients
Extended-duration prophylaxis may also improve outcomes and reduce the incidence of late-occurring VTE in the high-risk medical patients, such as those with prolonged immobility. Studies with enoxaparin, 24 rivaroxaban, 26 and apixaban 27 have all investigated the extended-duration prophylaxis in acutely ill medical patients. The EXCLAIM study, was the first large clinical trial to assess the benefits of extended-duration prophylaxis in acutely ill medical patients with reduced mobility. 24 In the overall population of EXCLAIM, the administration of extended-duration enoxaparin to medical patients with decreased mobility reduced the incidence of VTE compared with standard-duration prophylaxis with enoxaparin (2.5% vs 4.0%; absolute risk difference of −1.53% in favor of enoxaparin; 95.8% CI −2.54% to −0.52%). This difference was attributed largely to a decrease in the incidence of symptomatic DVT. The incidence of major bleeding increased during extended-duration prophylaxis compared with standard-duration prophylaxis (0.8% vs 0.3%; absolute risk difference of 0.51% favoring placebo; 95% CI 0.12%-0.89%), but the overall level of bleeding complications was low in both groups and similar to the values reported in previous studies.28,44
The MAGELLAN study compared the efficacy and safety of the oral direct factor X inhibitor rivaroxaban as extended-duration thromboprophylaxis (35 days) compared with the standard-duration enoxaparin (10 days followed by placebo) in hospitalized acutely ill medical patients. 30 The composite primary end point (asymptomatic proximal DVT, symptomatic DVT, symptomatic nonfatal PE, and VTE-related death) at day 35 was 4.4% with rivaroxaban and 5.7% with enoxaparin (hazard ratio [HR] 0.77; 95% CI 0.62-0.96; P = .02). However, rivaroxaban was associated with higher rates of clinically relevant bleeding (1.4% vs 0.5%; HR 3.0; P ≤ .0001), leading to a net clinical benefit favoring enoxaparin (7.8 vs 9.4). 30
In the ADOPT trial, patients who were hospitalized for ≥3 days with congestive HF, respiratory failure, or other medical disorders with 1 additional risk factor for VTE received either apixaban for 30 days or enoxaparin for at least 6 days (followed by placebo). 27 The primary 30-day efficacy outcome (death related to VTE, PE, symptomatic DVT, or asymptomatic proximal-leg DVT) was met by 2.71% patients in the apixaban group and 3.06% patients receiving enoxaparin (RR 0.87; 95% CI 0.62-1.23; P = .44). Major bleeding was reported in 0.47% of patients with apixaban and 0.19% with enoxaparin. 27
On the basis of these results, it seems that extended-duration prophylaxis may not be justified for a broad population of medically ill patients. However, there may be specific subpopulations of patients in which it may be warranted.
Benefits of Extended Prophylaxis Specific to Subgroups of Patients—Role in VTE Risk Assessment
The results of the EXCLAIM study help to identify which medical patients would benefit most from extended-duration prophylaxis by analyzing the effect of various levels of immobility on outcomes within the same patient population. The EXCLAIM study identified that extended-duration enoxaparin reduced the risk of VTE more than it increased the risk of major bleeding complications in acutely ill medical patients with age >75 years, women, and who were confined to bed or sedentary due to an acute medical illness. An analysis of several major subgroups of patients according to their primary diagnosis, comorbid conditions, or baseline characteristics consistently showed reductions in the risk of VTE in the patients who received extended-duration enoxaparin compared with placebo. 24 The effects on VTE reduction and bleeding of extended-duration prophylaxis compared with standard-duration prophylaxis were consistent across all these subgroups. 24 In a sub-analysis of patients who met the amended inclusion criteria, patients with level 2 immobility (with bathroom privileges), but without other predefined risk factors for VTE (age >75 years, prior VTE, or history of cancer) had a low incidence of VTE (1.9% with enoxaparin and 2.0% with placebo) and a smaller reduction in VTE risk (RRR 5%; RR 0.95; 95% CI 0.46-1.93). Within this subgroup, the rates of total bleeding were 7.5% with enoxaparin and 4.0% with placebo (RR 1.87; 95% CI 1.27-2.74). 24 Additionally, level 1 immobility was associated with an OR of 0.51 (95% CI 0.31-0.83) for VTE risk, and level 2 immobility was associated with an OR of 0.71 (95% CI 0.46-1.10), suggesting that increasing degrees of immobility are associated with a higher risk of VTE. Furthermore, the data demonstrate that the risk conferred by immobility is compounded by the presence of additional risk factors. Accordingly, the data suggest that extended-duration prophylaxis would reduce the risk of VTE in all subgroups of patients with level 1 immobility or level 2 immobility with risk factors for VTE but may not be justified in patients with level 2 immobility (with bathroom privileges) without other predefined risk factors for VTE.
A subgroup analysis of the MAGELLAN trial identified that patients with higher baseline
Considering that it seems that patients at highest risk of VTE benefit most from extended-duration prophylaxis with enoxaparin (EXCLAIM) and rivaroxaban (MAGELLAN), perhaps patients in the ADOPT trial were not “high risk enough” to show a beneficial effect of extended-duration apixaban. There is increasing evidence to suggest that our current definitions may not be sufficient to characterize patients at high risk of VTE. A study in Canada of medical records for 1134 consecutive high-risk medical patients followed for 100 days post-discharge showed that despite in-hospital standard mechanical or pharmacological prophylaxis, 21% of patients received medical care for symptoms associated with VTE. 46 Only 4% had diagnostically confirmed VTE and tests were negative or inconclusive for the remaining 17%. The mean time to confirmed VTE event was 34.1 days postadmission. These data suggest that the real-life rates of VTE are higher compared with randomized clinical trials. Further data from the same source found that the risk of confirmed symptomatic VTE increased from 2.9% in patients with no more than 2 risk factors to 6.1% of patients with over 2 VTE risk factors, to 8.7% in patients with over 3 risk factors. 47 The mean length of time to first VTE event was 33.5 days, most (80%) of the first events occurred by day 57 after hospital admission and almost all events (90%) by day 69.
Collectively these data suggest that extended-duration prophylaxis may be in order in certain high-risk patients to protect the patients from the risk of VTE events occurring, particularly in the posthospitalization period. Baseline
Conclusions
Immobility is an important risk factor for VTE. 13 Many acutely ill medical patients have a history of immobilization or ongoing reduced mobility due to either their presenting illness or comorbid conditions such as respiratory failure, HF, and obesity. However, although clinical studies of VTE prophylaxis in medical patients have incorporated varying definitions of immobility in their inclusion criteria, immobility as a specific VTE risk factor per se has not been extensively studied. There are gradients in the level of immobilization so definitions need refining, especially as regional hospital practice may vary in promoting mobilization. What is clear from studies to date is that thromboprophylaxis with an LMWH or fondaparinux significantly reduces the risk of VTE in at risk acutely ill medical patients with recent immobility with no significant increase in the risk of major bleeding complications.
The optimal duration of prophylaxis in medical patients with reduced mobility has not been established. The results of large-scale clinical trials such as MEDENOX and PREVENT indicate that the current 10-day regimen of prophylaxis may be too short, with late VTE events occurring more than 1 month after the start of the acute illness. However, extended prophylaxis may not be appropriate for all acutely ill medical patients. The EXCLAIM trial has shown that extended-duration prophylaxis with enoxaparin benefits acutely ill medical patients with level 1 immobility (bed rest or sedentary without bathroom privileges), who are female and older than 75 years of age. A subgroup analysis of the MAGELLAN trial identified patients with baseline
Footnotes
Author’s Note
The author received editorial/writing support in the preparation of this manuscript funded by sanofi-aventis US, Inc. Anne Ozog, PhD, of Excerpta Medica provided the editorial/writing support. The author is fully responsible for all content and editorial decisions, and received no financial support or other form of compensation related to the development of the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Hull has received grants/research support from Bayer Pharmaceuticals Corporation, LEO Pharma Inc, and sanofi-aventis; been a consultant for Bayer Pharmaceuticals Corporation, LEO Pharma, Inc, Pfizer Inc, GlaxoSmithKline, and Wyeth Pharmaceuticals; and sat on advisory boards for Bayer Pharmaceuticals Corporation, Pfizer Inc, and sanofi-aventis.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.