
Abstract
Venous thromboembolism (VTE) in adolescents is a serious condition that requires prompt recognition and optimal management to prevent mortality and long-term morbidity. Adolescents account for a large proportion of cases of VTE in children. As teenagers transition from childhood to adulthood, they are at risk of developing medical conditions and exposure to risky habits that predispose them to VTE. This review focuses on the variety of risk factors and comorbidities seen in adolescent VTE and takes a quick look into risk-based preventive strategies for primary and secondary prevention.
Introduction
The incidence of venous thromboembolism (VTE) in the pediatric population is rising in parallel with, and likely due to, increased awareness and advances in diagnostic modalities, therapeutic approaches, technologic support, and supplemental care for illnesses, both simple and complex. Several studies have shown 3- to 10-fold increases in the frequency of VTE diagnosed in hospitalized children during the past 2 decades. 1 Most studies also show a bimodal peak distribution, with neonates and adolescents reported to be at the greatest risk of development of VTE.
Although reports have addressed risk factors for VTE among adolescents with individual medical conditions, the overall prevalence and risk factor profile in adolescent VTE has not been clearly delineated. This review is an attempt to summarize the available literature about risk factors in adolescent VTE. The epidemiology of adolescent VTE and its prevalence in various medical conditions are discussed, emphasizing the need for increased awareness among health-care professionals and patient families about the panel of health disorders that predispose adolescents to the development of VTEs. This review also highlights the need for a comprehensive approach to consider timely prophylactic measures in high-risk scenarios in adolescents in order to prevent this serious complication.
Epidemiology of Adolescent VTE
Several recent analyses of nationally representative data for pediatric VTE in the United States have shown an increased rate and risk of VTE in the adolescent population. The Pediatric Hospital Information System (PHIS) database report from 2001 to 2007 showed that of 13,449 VTE admissions among 2,920,000 hospitalized children, teenagers, and neonates accounted for the majority of VTE admissions. 2 Adolescents in the age-group of 13 to 18 years accounted for 30% of all VTE admissions (n = 4003/13,449). The rate of admissions for VTE increased 49% among teenagers during this study period. In addition, the proportion of patients with recurrent VTE was significantly higher among teenagers. The report from Kid’s Inpatient Database 2006 evaluating children aged 18 years and younger with in-hospital VTE in a large array of pediatric and community hospitals found adolescents older than 15 years of age form the greatest proportion (37.8%) of this population. 3 When standardized against the entire database of discharges, a greater risk of developing VTE was noted in both early teenagers aged 10 to 14 years (relative risk [RR] 1.62; 95% confidence interval [CI] 1.45-1.80) and late adolescents aged 15 to 18 years (RR 1.89; 95% CI 1.73-2.07) when compared to younger children. The Nationwide Inpatient Sample Data report documented an overall increase of 102% in VTE in hospitalized children from 1994 to 2009, with adolescents ranking next to infants in increase of VTEs and having the highest odds (OR 6.25; 95% CI: 5.66-6.89) for a diagnosis of VTE. 4 Stein and colleagues analyzing National Hospital Discharge Survey database over a 23-year period also showed that, similar to infants, the rate of VTE in adolescents is higher than in other children (11.4 VTE of 100,000 children/year; P < .001). 5 The study from Canadian pediatric registry showed that between 1990 and 1992, the frequency of VTE was highest among teenagers aged 11 to 18 years when compared to other children (n = 69 of 137; 50%). 6 The nationwide population-based study in Denmark in children aged 0 to 18 years with first-ever noncerebral VTE and or arterial thromboembolism (TE) between 1994 and 2006 showed highest incidence rates for VTE among adolescents aged 15 to 18 years (8.46; 95% CI: 7.50-9.55). 7 The results of these reports with regard to adolescent VTE are summarized in Table 1. With such increased incidence of VTE in adolescents, it is incumbent upon physicians to understand and appropriately address the thrombogenic risk factors for clot prevention and management.
Published Results on the Epidemiology of Adolescent VTE.
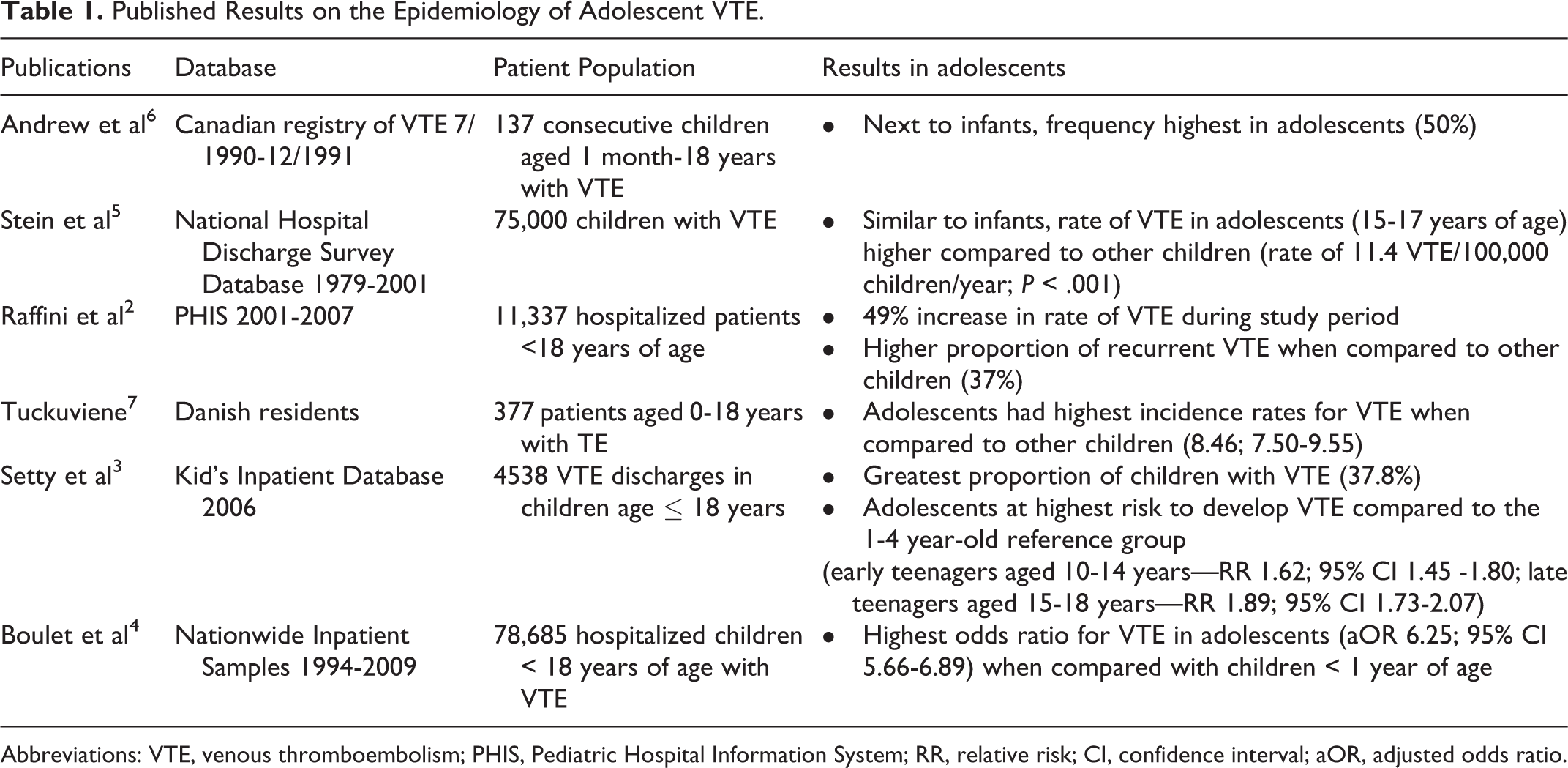
Abbreviations: VTE, venous thromboembolism; PHIS, Pediatric Hospital Information System; RR, relative risk; CI, confidence interval; aOR, adjusted odds ratio.
Risk Factors
Comorbidities in Adolescent VTE
In the Kids Inpatient Database 2006 report, 3 both acute and chronic medical conditions were associated with adolescent VTE. Several publications 8 –52 have addressed the associations of VTEs in a variety of medical conditions in adolescents. These conditions include congenital or inherited abnormalities such as anatomic abnormalities and inherited thrombophilia; acquired conditions including antiphospholipid antibody syndromes (APSs), cancer, inflammatory bowel disease (IBD), trauma, pregnancy, and iron deficiency; and modifiable risk factors such as obesity, continuous video/computer gaming, and hormone therapy (Table 2).
Prothrombotic Risk Factors in Adolescent VTE.
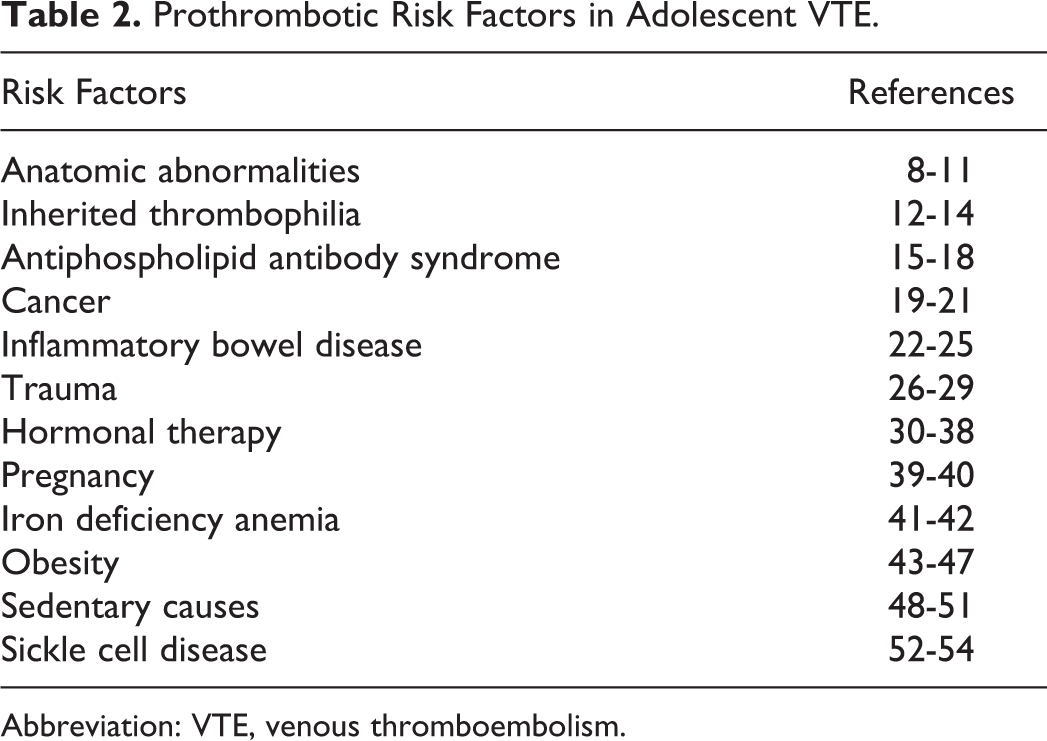
Abbreviation: VTE, venous thromboembolism.
Anatomic Abnormalities
Abnormal anatomy may be the primary predisposing risk factor in adolescents presenting with idiopathic VTE, but it often is not considered and systematically investigated in clinical practice. Very few articles address this issue; in 1 article reporting on 5 adolescents with VTE and anatomic abnormalities, the authors undertook a MEDLINE search to identify all cases of VTE reported in patients 21 years old or younger. 8 Interestingly, 95% of patients reported with anatomic abnormalities, including May-Thurner syndrome, Paget-Schroetter syndrome, and inferior vena cava (IVC) anomaly, were adolescents.
Paget-Schroetter syndrome causing VTE of upper extremity, typically occurs in the adolescent-young adult (AYA) population; it is seen more often in males taking part in sports or music causing strenuous activity of the upper limbs. 9 The repetitive activity of the extremity leads to hypertrophy of the pectoral muscles and damages the vein wall, causing thrombosis. Typically, the dominant limb is affected, presenting as acute or chronic deep vein thrombosis (DVT). Often other risk factors such as inherited thrombophilia, dehydration, and hormone therapy coexist. Lack of recognition of this entity can lead to chronic obstruction, postthrombotic syndrome, disabling venous hypertension, and risk of pulmonary embolism (PE). Prompt diagnosis and aggressive medical and/or surgical management are essential to establish venous flow and to avoid debilitating long-term issues.
May-Thurner syndrome, an anatomic abnormality of the lower extremity leading to VTE caused by extrinsic venous compression of the left common iliac vein by the right common iliac artery, is again frequently reported in patients in the second and third decades of life, often in association with other coexisting risk factors. 10 Females are more commonly affected than males, and lack of recognition can lead to prolonged venous obstruction, including the rarely reported left common iliac vein rupture.
Agenesis of the IVC has been reported in as many as 5% of patients with VTE younger than 30 years of age. 11 The presenting features are quite homogenous with young adult men presenting with low back pain, usually after a period of physical exertion. Some patients have additional risk factors including inherited thrombophilia. Bilateral lower extremity thrombosis is reported in as many as one-third of the patients. The risk of PE is lower, as the embolus has to travel through the azygos and the hemiazygos systems, wherein it is prone to be trapped.
Because DVT due to anatomic abnormalities is invariably reported in adolescents, a high index of suspicion and evaluation with appropriate imaging is required in patients presenting with typical clinical features. Once diagnosed, institution of proper medical and/or surgical management can prevent VTE recurrence, improve quality of life, and enable continued use of the affected limb.
Inherited Thrombophilia
Inherited thrombophilia, well known risk factors for VTE, have increasingly gained interest since they were first described by Egeberg in 1965. 12 The questions of which population is at risk and who should be tested have been well debated, as detection of an inherited thrombophilia may have implications for the patient and his or her family members. A recent publication analyzing the MAin-ISar-THROmbosis registry data for prevalence of thrombophilia according to age at first VTE sheds some light on the prevalence of inherited thrombophilia in the AYA population and their risk of developing a VTE. 13 This single-center, cross-sectional registry from 2000 to 2010 analyzed data on a total of 1490 patients with VTE who underwent testing for inherited thrombophilia. The median age of this cohort was 43 years (range 8 to 87 years). This study showed that the prevalence of thrombophilia in patients with VTE decreased with age, with a prevalence of 49.3% in those younger than 20 years of age, compared to 21.9% in those older than 70 years of age (P < .001). Also, when compared to patients without thrombophilia, VTE occurred prematurely, with an average of 11, 17, and 9 years earlier, in those with factor 5 R506Q mutation, protein C, or S deficiencies, respectively.
In adolescents with unprovoked VTE, there are clear recommendations to test for inherited thrombophilia. 14 Future studies focusing on adolescents with VTE are needed to determine whether these patients have increased prevalence of inherited thrombophilia when compared to younger children, and whether testing is warranted in adolescent VTE in the presence of other underlying risk factors.
Antiphospholipid Antibody Syndrome
The APS, an autoimmune prothrombotic condition comprised of primary and secondary APS, can cause arterial, venous, and small vessel thrombosis. 15 The APS is reported often in adolescents and is recognized to be the most common autoimmune thrombotic state in children, with a predominance of deep vein thrombosis (DVT) and stroke when compared to adults.
A report on 121 patients (median age 10.7, range 1.0-17.9 years) with APS from the international Pediatric APS registry compiled information on previously published and new cases from 24 pediatric centers from 14 countries. This publication showed an exceedingly high prevalence rate of thrombosis in all reported patients: 60% with venous thrombosis, 32% with arterial thrombosis, 6% with small-vessel thrombosis, and 2% with both arterial and venous thrombosis. 16 Arterial thrombosis and ischemic stroke were seen more commonly in the younger patients with primary APS, whereas VTE was seen frequently in the older patients with secondary APS. The site of thrombosis was diverse, affecting the vascular tree at any level and in any organ. Cerebrovascular thrombosis was noted in one-third of the patients. As 45% of patients tested had one or more inherited thrombophilic risk factors, multifactorial pathogenesis for VTE was implicated in this study. The recurrence rate was high at 19%, and mortality caused by VTE was 5.7%.
The life-threatening variant of APS is catastrophic APS (CAPS) defined by the development of multiple thromboses over a short period of time. 17 The pediatric CAPS registry reports on 45 patients with a mean age of 11 years, with 46 catastrophic events before the age of 18 years. 18 In addition to multiorgan involvement, peripheral vein thrombosis was noted more often in children when compared to adults. Also, CAPS was the first manifestation of APS in 86.6% of children.
Cancer
Recent years have seen an increasing trend in the number of admissions for the cancer in AYA in US pediatric hospitals. This increase could be an effect of increasing recognition, shift in referral of adolescent oncology patients to pediatric centers, more clinical trials developed for this population, or general growth of the population in this age-group. Although there is information about VTE complications in children with cancer overall, 19 data on the adolescent subset with cancer have been lacking. A single-institution retrospective cohort study of 726 children with cancer evaluating for the epidemiology and clinical risk factors for VTE showed increased incidence in patients older than 10 years when compared to younger patients (OR 1.82; 95% CI 1.0-3.2; P = .036). 20 This increased risk on multivariate analysis was not explained by the type of cancer or intensity of treatment and was attributed to the physiologic changes in the adolescent’s hemostatic system with reduction in fibrinolytic factors and response resulting in reduced fibrinolysis.
The study by O’Brien and colleagues specifically addressed this issue by evaluating the AYA oncology inpatient admissions recorded in the PHIS database from 2001 to 2008 for the prevalence of VTE. 21 Of 51,498 hospital admissions of 9721 AYAs with cancer between the ages of 15 and 24 years, the study showed that 5.3% experienced VTE. In multivariate analysis, the type of cancer was strongly associated with VTE, with patients with leukemia, lymphoma, and sarcoma having a higher likelihood of developing a VTE when compared to patients with brain tumors and other malignancies. In addition, VTEs were found to occur more often in patients aged 18 years and older. These data may not be representative of AYAs cared for in nonfreestanding pediatric centers and adult centers and provide less information about certain common AYA malignancies such as testicular cancer, thyroid cancer, melanomas, and tumors managed predominantly in the outpatient setting such as Hodgkin’s lymphoma. Nonetheless, this large study provides the first characterization of this serious complication in the AYA oncology population.
Inflammatory Bowel Disease
Although several studies in adults suggest an increased risk of developing VTE in adults with IBD, 22 few reports in children have addressed this concern. A single-institution, retrospective review of hospitalized children and young adults with IBD showed increased risk, with an incidence of 1.9% for VTE among 532 patients aged 8 to 23 years. 23 A systematic review estimated a 4- to 20-fold increased risk in children with IBD compared to those without, with 60% occurring in the 12- to 18-year-old age-group. 24 Nylund and colleagues analyzed the triennial Healthcare Cost and Utilization Project Kids’ Inpatient database across 5 time periods (1997-2009) and showed an RR of 2.36 (95% CI 2.15-2.58) for VTE in hospitalized children and adolescents with IBD. 25 The etiology as shown in these studies is often multifactorial, with a combination of inherited and acquired risk factors for VTE; however, in the systematic review, 50% of patients had no other risk factors, showing that IBD per se ought to be considered an RF. Venous thromboembolism has been reported predominantly in hospitalized and acutely ill patients, with severe events including frequent cerebral VTE, PE, Budd-Chiari syndrome, portal vein thrombosis, and DVT. In addition, these patients often had increased morbidity and mortality rates caused by VTE and persistence and recurrence of VTE.
Trauma
Although hospitalized adult patients with trauma are well reported to be at high risk of having a VTE, data are lacking on the prevalence and risk factors for VTE in children in general and specifically in adolescents after trauma. The study by Grandas et al evaluated children younger than 16 years of age with trauma and stated that VTE is unusual in this population, with a rate of 0.1%. 26 Vavilala and colleagues collated pediatric trauma data in the administrative databases from 19 states across the United States and reported a rate of 0.8% for VTE in 58,716 trauma-related discharges in children younger than 15 years. 27 In addition to increased risk of VTE with higher injury severity scores and the use of central venous catheters, they also found greater risk of VTE in older children.
The lack of data on VTE in adolescent trauma victims is also reflected in the lack of consensus in using prophylactic measures in these patients. The survey of the Society of Trauma Nurses with responses from 133 institutions showed that pharmacoprophylaxis was never or rarely used by 60% of these centers in children 11- to 15-year olds, and use was variable among older adolescents. 28 This finding is in contrast to adults in whom, in patients without contraindications, use of pharmacoprophylaxis is a well-established practice.
A recent large study of the National Trauma Data Bank data analyzed a total of 402,329 hospitalized patients with trauma aged 21 years or younger from 2008 to 2010 and found DVT and/or PE in 0.4% of these patients. 29 These authors reported 2-fold higher odds of being diagnosed with VTE in adolescents aged 13 to 15 years and a dramatic 4-fold higher odds in those 16 years or older. This age-related risk was found to be independent of other risk factors such as obesity, central line placement, surgery, length of hospital stay, or injury severity.
Hormonal Therapy and Other Risk Factors in Female Adolescents
Hormonal therapy is prescribed frequently for adolescent teens for a variety of medical conditions, in addition to contraception. 30 The thrombotic risk with use of hormonal therapy has received considerable attention. 31 In addition, the combined effect of thrombogenesis with hormonal therapy in several settings such as inherited thrombophilia, obesity, APS, and other risk factors is also well recognized (Table 3). 32 This concern has led to provision of guidelines and practice bulletins by the American College of Obstetricians and Gynecologists, 33 the World Health Organization, 34 and the Centers for Disease Control 35 to guide practitioners when choosing hormonal therapies for patients with high-risk medical conditions. The medical eligibilty criteria (MEC) addresses various thrombophilic medical conditions affecting the use of hormonal therapy and other contraceptive methods, dividing them into categories 1 to 4 in the order of increasing health risk. In general, estrogen containing hormonal therapy is to be avoided in patients with VTE. The MEC category 2 is assigned for the use of various progestin-only methods in patients with past history of VTE or underlying inherited thrombophilia. In the setting of acute VTE, the use of progestin-only therapy falls into the higher risk category 3. Another contraceptive option for such patients is the copper intrauterine device (IUD), as it is placed in the lowest risk category of 1. Several long-acting reversible contraceptives are available and include levonoregestrel IUD, copper IUD, etonogestrel implant, and depo medroxyprogesterone acetate injections, which have been shown to be safe, not to increase the risk of thrombosis, and to be reasonable options to prevent unintended pregnancy, a condition which escalates the risk of thrombosis even further beyond baseline. 30,36
Relative Risk of Thrombosis in Adolescent Females in Health Conditions. 32
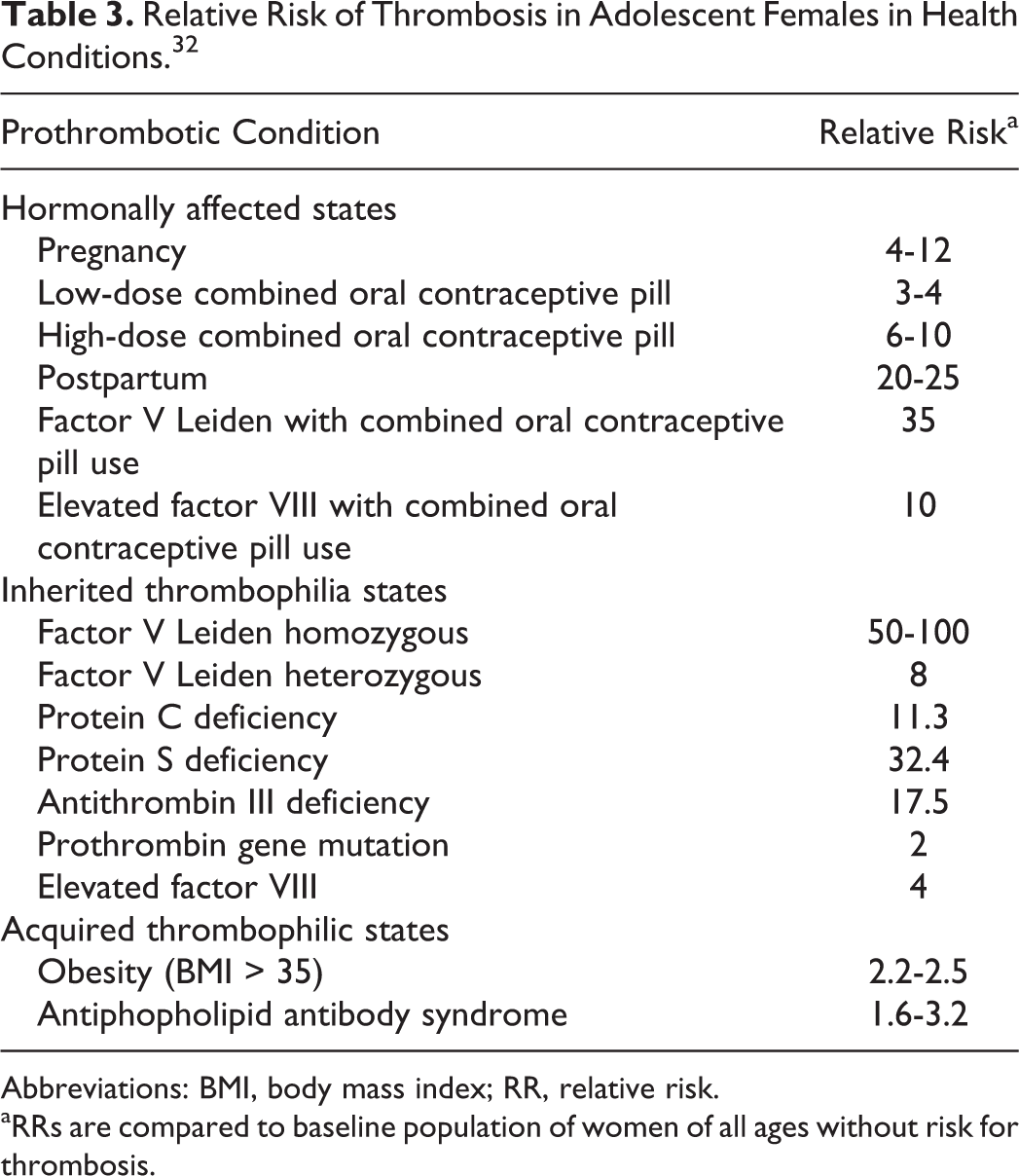
Abbreviations: BMI, body mass index; RR, relative risk.
aRRs are compared to baseline population of women of all ages without risk for thrombosis.
The current literature suggests that it is not cost effective to mass screen females for underlying inherited thrombophilia prior to initiating hormonal therapy. 37 Screening is recommended only in the settings of active VTE, strong family history of VTE, and when the screening results could affect the management. 38 Other factors to consider include the patient’s age and the baseline risks of thrombosis for certain populations as well as the risk in the setting of hormone use. In patients with a known thrombophilic condition, estrogen therapy generally is contraindicated. However, in certain situations that require estrogen therapy (eg, delayed puberty occurring with Turner Syndrome), 38 it should be initiated only after careful patient counseling about the risks and benefits of such therapy. Otherwise, several safe progestin-only options that do not increase the risk of thrombosis are available to manage conditions related to menses or functional ovarian cyst activity.
Pregnancy with multiple physiologic prothrombotic changes, including hypercoagulable state, decreased mobility, mechanical obstruction of vessels, and vascular injury, is a well-recognized risk factor for thrombosis (Table 2). In a patient who already has risk of developing a VTE, an unplanned pregnancy could result in a compounded thrombotic risk. 39 A recent analysis of Nationwide Inpatient Sample from 1994 to 2009 showed increasing trend in VTE diagnosis in pregnant adolescent and adult women, likely contributed by a rise in comorbid conditions such as obesity and hypertension. 40 The occurrence of cerebral sinovenous thrombosis in adolescents with iron deficiency anemia caused by heavy menstrual bleeding and other causes is an interesting association. 41,42 The pathophysiology of this association has not been fully elucidated, although thrombocytosis and decreased red cell deformability in iron deficiency have been proposed as contributing to thrombogenesis.
Obesity
Obesity in children and adolescents is a public health concern in Western societies and has been linked to cardiovascular disease and increased risk for thrombosis. 43 Hypercoagulable state in an obese individual is evidenced by the presence of elevated factor VII level, thrombin and thrombin–antithrombin complexes, tissue factor procoagulant activity, γ-fibrinogen concentration, and increased platelet activation. 43,44 In the pediatric population, studies have shown increased risk for development of VTE in patients with cardiovascular and cerebrovascular diseases because of enhanced atherogenesis and thrombogenesis in the setting of obesity. 45 –47 The combination of obesity with other risk factors such as inflammatory mediators and estrogen therapy in young women has been shown to further heighten the risk of developing a VTE. Further elucidation of the complex interactions between obesity and thrombogenesis will help to identify potential therapeutic targets in the future.
Sedentary Causes
Due to the evolving behavior of extreme, continuous video and/or computer gaming for several hours, youth are facing an emerging threat of developing “Gamer’s thrombosis” caused by venous stasis resulting from extended periods of sitting. 48 –50 Information in the medical literature is scarce, with only a few case reports citing extreme cases in otherwise healthy adolescents with VTE, including bilateral and recurrent DVT and PE requiring aggressive surgical interventions in addition to medical management. These case reports raise the concern that continuous gaming may be a thrombotic risk factor of clinical significance. Although few educational Web sites address physical and social issues related to extreme gaming, increased awareness is needed among the medical personnel about the potential risk for developing VTE in this population. 51 Further research is also required to understand the true frequency of Gamer’s thrombosis, as preventive strategies, such as taking frequent breaks and doing leg exercises similar to those advised for air travelers, may help to avert this “e-thrombosis.”
Sickle Cell Disease
An example for cross-talk between inflammation and coagulation is perhaps the increased propensity for development of VTE in patients with sickle cell disease (SCD). Although it is not exclusive to adolescents, the heightened association of PE in acute chest syndrome and increased incidence of DVT in pregnant patients with SCD encompasses adolescents, with the risk increasing in association with other coexisting factors such as hormonal therapy, indwelling catheters, and infections. 52,53 Whether VTE plays a role as cause or effect in sickle-cell-related pulmonary disorders has not been fully elucidated and remains an under-recognized complication. A recently published retrospective cohort study 54 analyzing data from the Cooperative Study of Sickle Cell Disease has shown that patients older than 15 years who have SCD are at increased risk for VTE and those with VTE are at higher risk for death than those without. Increased awareness of VTE associated with SCD is important and further studies to unravel the pathophysiology of TE in these patients are needed to institute timely interventions.
Thromboprophylaxis
The American College of Chest Physicians evidence-based clinical practice guidelines for antithrombotic therapy in neonates and children 55 recommends primary prophylaxis for VTE in patients with certain underlying conditions including cardiac catheterization, specific cardiac surgeries, cardiomyopathy, primary pulmonary hypertension, long-term total parenteral nutrition, hemodialysis with central venous access device (CVAD) or arteriovenous fistula, and Kawasaki disease with moderate or giant coronary artery aneurysm. Secondary prophylaxis is recommended for patients with CVAD or with other ongoing risk factors for TE until they resolve.
No uniform practice exists for thromboprophylaxis in adolescents managed in pediatric hospitals, although it is strongly recommended for hospitalized critically ill adults without a contraindication for anticoagulation. A multinational study of thromboprophylaxis practice (including pneumatic/sequential compression devices or graduated compression stockings as mechanical prophylaxis and aspirin, clopidogrel, low-molecular-weight heparin, subcutaneous unfractionated heparin, intravenous unfractionated heparin >10U/h, or coumadin as pharmacoprophylaxis) in critically ill children showed that even though 86.9% of children in the pediatric intensive care unit studied had ≥ 1 risk factor for thrombosis, only 12.4% of the patients received pharmacoprophylaxis, and only 23.8% received mechanical prophylaxis. The study documented high variations and lower rates of practice of both mechanical and pharmacologic prophylaxis in critically ill children when compared to adults, which were seen more often but not consistently in teens older than 13 years of age. 56 Raffini and colleagues undertook the implementation of a patient-safety and quality-improvement project in adolescents older than 14 years of age in their institution to use risk-based pharmacologic (enoxaparin or unfractionated heparin) and/or mechanical thromboprophylaxis (pneumatic compression device and/or graduated compression stockings). 57 Hospitalized teens were risk stratified depending on their mobility status and VTE risk factors, including acute and chronic medical conditions and past and/or family history of VTE. For ambulatory patients without additional VTE risk factors, early ambulation was recommended, whereas the interventions for patients at high risk (VTE risk factor and altered mobility) and at risk (at least 1 risk factor for VTE) included pharmacologic and/or mechanical thromboprophylaxis, the former administered to patients without contraindications for anticoagulation. This initiative resulted in no patient developing noncatheter-related VTE, with low incidence of bleeding overall. 58 In addition, from a baseline of 22%, the rate of VTE prophylaxis at their institution increased to an average rate of 82%, with intermittent improvements up to 100%. Similar strategy for VTE prevention has been proposed by Meier and colleagues 59 based on their recent review of pediatric literature on VTE prophylaxis in adolescents.
There is a need for multi-institutional studies to better define the role of pharmacologic and/or mechanical thromboprophylaxis in the prevention of adolescent VTE in hospitalized patients. Studies incorporating risk stratification of hospitalized adolescents based on underlying thrombotic risk factors and institution of measures such as early ambulation, pneumatic/sequential compression devices, or graduated compression stockings in patients at lower risk for VTE and pharmacologic prophylaxis with low-molecular-weight or unfractionated heparin for high risk patients will enable assessment of clot prevention benefits and bleeding risks in hospitalized children and help reach a consensus guideline for adolescent thromboprophylaxis. Risk-stratified approaches can then be applied uniformly in pediatric institutions to identify and provide thromboprophylaxis for at-risk hospitalized adolescents. Further work is required to understand the true epidemiology and risk association in adolescent thrombosis in order to develop effective risk-adapted strategies. These approaches might not only lead to recognition and management of at-risk adolescents with VTE prophylaxis but also help identify adolescents who may benefit from minimal intervention such as early ambulation. In the out-patient setting, increased awareness among providers of high-risk situations for adolescent VTE may lead to teen education to avoid or modify risk factors to prevent VTE.
Conclusion
The prevalence of VTE in adolescents is high and has been increasing in recent years. Focused evaluation and management of teenagers with VTE is needed, as often the etiology is multifactorial requiring specific measures to manage the underlying risk factors for VTE and preventing recurrence. Further research focusing on adolescents with VTE will help us to better understand the true epidemiology and risk association and enable us to develop effective risk-adapted strategies for at-risk adolescents. This approach can in turn lead to routine risk-based institution of mechanical and/or pharmacologic prophylaxis in adolescents with acute illness and chronic health conditions. In addition, educating teens about the various risk factors and life-style modification strategies can lead to a positive impact in the future in reducing the rate of VTE in these youngsters, who have a long life ahead of them.
Footnotes
Authors’ Note
LS drafted, reviewed, edited, and revised the manuscript. JED drafted, reviewed, edited, and revised the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.