
Abstract
The aim of this study is to investigate the association between neutrophil to lymphocyte ratio (NLR) and severity of coronary atherosclerosis. A total of 172 patients undergoing coronary angiography were included in the study. Control group consisted of patients with normal coronary arteries. Patients with coronary stenosis were divided into 2 groups by use of Gensini scores. The NLR was higher in severe atherosclerosis group compared with mild atherosclerosis and control groups (P < .001). In correlation analysis, NLR showed significant correlation with Gensini score. A cutoff value of 2.5 for NLR predicted severe atherosclerosis with a sensitivity and specificity of 62% and 69%, respectively. After multivariate analysis, high levels of NLR were independent predictors of severe atherosclerosis together with glucose and high-density lipoprotein. Our study suggests that the NLR is a predictor of severe atherosclerosis that may be useful for cardiac risk stratification in patients with coronary artery disease.
Introduction
Atherosclerosis is a complex inflammatory disease. 1 Inflammation plays a major role at all stages of coronary artery disease (CAD). 2 White blood cell count and its subtypes have been studied as inflammatory biomarkers to predict adverse cardiovascular outcomes. 3,4 Neutrophil to lymphocyte ratio (NLR) has recently emerged as new prognostic marker. 5 A number of studies have suggested that NLR was associated with adverse outcomes in patients undergoing coronary angiography, 4 in those with stable and unstable CAD, 6,7 and also in patients undergoing percutaneous coronary intervention 8 or coronary artery bypass grafting. 9 The relationship between NLR and CAD has been shown in several studies, but there are no data available with severity of coronary atherosclerosis measured using Gensini scores. In the present study, we evaluated the association between NLR and severity of coronary atherosclerosis in patients undergoing coronary angiography.
Methods
Study Population
The present study is a single-center, observational study. The study population consisted of 172 eligible consecutive patients who underwent coronary angiography for suspected or known coronary atherosclerosis. Exclusion criteria were clinically significant valvular heart disease, significant congestive heart failure, hematological disease, cancer, severe renal or liver disease, ongoing infection or systemic inflammatory conditions, and autoimmune disease. All participants gave an informed consent and the study was approved by local ethics committee.
Clinical Variables and Cardiovascular Risk Factors
Patients enrolled in the study underwent detailed clinical examination for the assessment of the cardiac status and were asked for smoking, family history of CAD, previous myocardial infarction, hypertension, diabetes mellitus, and noncardiac diseases. Arterial hypertension was considered in patients with repeated blood pressure measurements >140/90 mm Hg or active use of antihypertensive drugs. Diabetes mellitus was defined as fasting plasma glucose levels more than 126 mg/dL in multiple measurements or active use of antidiabetic medications. Smoking was defined as current smoking. The family history of CAD was considered as a history of CAD or sudden cardiac death in a first-degree relative before the age of 55 years for men and 65 years for women. Acute coronary syndrome (ACS) was defined as presentation with symptoms of ischemia in association with qualifying electrocardiographic changes or positive cardiac enzymes.
Biochemical and Hematological Parameters
Peripheral venous blood samples were drawn after patients overnight fasting. Total and differential leukocyte counts were measured by an automated hematology analyzer (Abbott Cell-Dyn 3700; Abbott Laboratory, Abbott Park, Illinois). Absolute cell counts were used in the analyses. Total and high-density lipoprotein (HDL) cholesterol, triglycerides, and fasting glucose were measured using the Abbott Architect C16000 autoanalyzer (Abbott Laboratory). Concentrations of low-density lipoprotein were calculated using Friedewald equation. 10
Coronary Angiography and Severity of Coronary Atherosclerosis
Coronary angiography was performed by Judkins technique through femoral artery access using the Allura Xper FD10 (Philips, Amsterdam, The Netherlands). Each angiogram was evaluated by 2 interventional cardiologists who were blinded to the study plan and to each other. A thorough review of each index coronary angiogram established lesion location and percentage of stenosis among all the coronary lesions.
The CAD was defined as the presence of significant stenosis, at least 50% of the vessel diameter, in any of the main coronary arteries, in accordance with the American College of Cardiology/American Heart Association lesion classification. 11
The Gensini scoring system was used to determine the severity of CAD. 12 This method defines narrowing of the lumen of the coronary arteries as 1 for 1% to 25% stenosis, 2 for 26% to 50%, 4 for 51% to 75%, 8 for 76% to 90%, 16 for 91% to 99%, and 32 for total occlusion. The score is then multiplied by a factor representing the importance of the lesion’s location in the coronary artery system. For the location scores, 5 points were given for left main lesion; 2.5 for proximal left anterior descending (LAD) or left circumflex (LCX) artery; 1.5 for the mid-segment LAD and LCX; 1 for the distal segment of LAD and LCX, first diagonal branch, first obtuse marginal branch, right coronary artery, posterior descending artery, and intermediate artery; and 0.5 for the second diagonal and second obtuse marginal branches.
Coronary angiography revealed that there were coronary stenosis in 126 patients and normal coronary arteries in remaining 46 (control group). The 126 patients with coronary stenosis were divided into 2 groups according to Gensini scoring 13 : those with mild atherosclerosis (n = 63; Gensini score 1-29) and severe atherosclerosis (n = 63; Gensini score ≥30).
Statistical Analysis
Continuous variables were defined means ± standard deviation; categorical variables were given as percentages. The Kolmogorov-Smirnov test was used to verify the normality of distribution of continuous variables. The independent sample t test or the Mann-Whitney U test was used for the continuous variables and the chi-square test for categorical variables. One-way analysis of variance or Kruskal-Wallis tests were used to compare 3 groups. Correlations were assessed using Spearman rank test. Receiver–operating characteristic (ROC) curve analysis was used to determine the optimum cutoff levels of NLR to predict the severity of CAD. Multivariate logistic regression analysis was performed to assess the independent predictors of severe atherosclerosis. All variables which were found significant in univariate analysis were included in the model of logistic regression model and results are shown as an odds ratio (OR) with 95% confidence intervals (CIs). Statistical analyses were performed using SPSS 15.0 (SPSS Inc, Chicago, Illinois). A 2-tailed P < .05 was considered as statistically significant.
Results
The study population consisted of 126 patients with coronary stenosis (men 66%, mean age: 61 ± 13 years) and control group of 46 patients with normal coronary arteries (men 65%, mean age: 58 ± 11 years). Baseline demographic, biochemical and hematological characteristics of mild and severe atherosclerosis, and control study groups are outlined in Table 1. According to age, gender, and coronary risk factors, there was no difference between groups. Serum glucose (P < .001) and creatinine levels (P = .002) were significantly higher in patients with severe atherosclerosis, whereas HDL levels were lower than controls (P < .001).
Baseline Characteristics of the Study Population.a
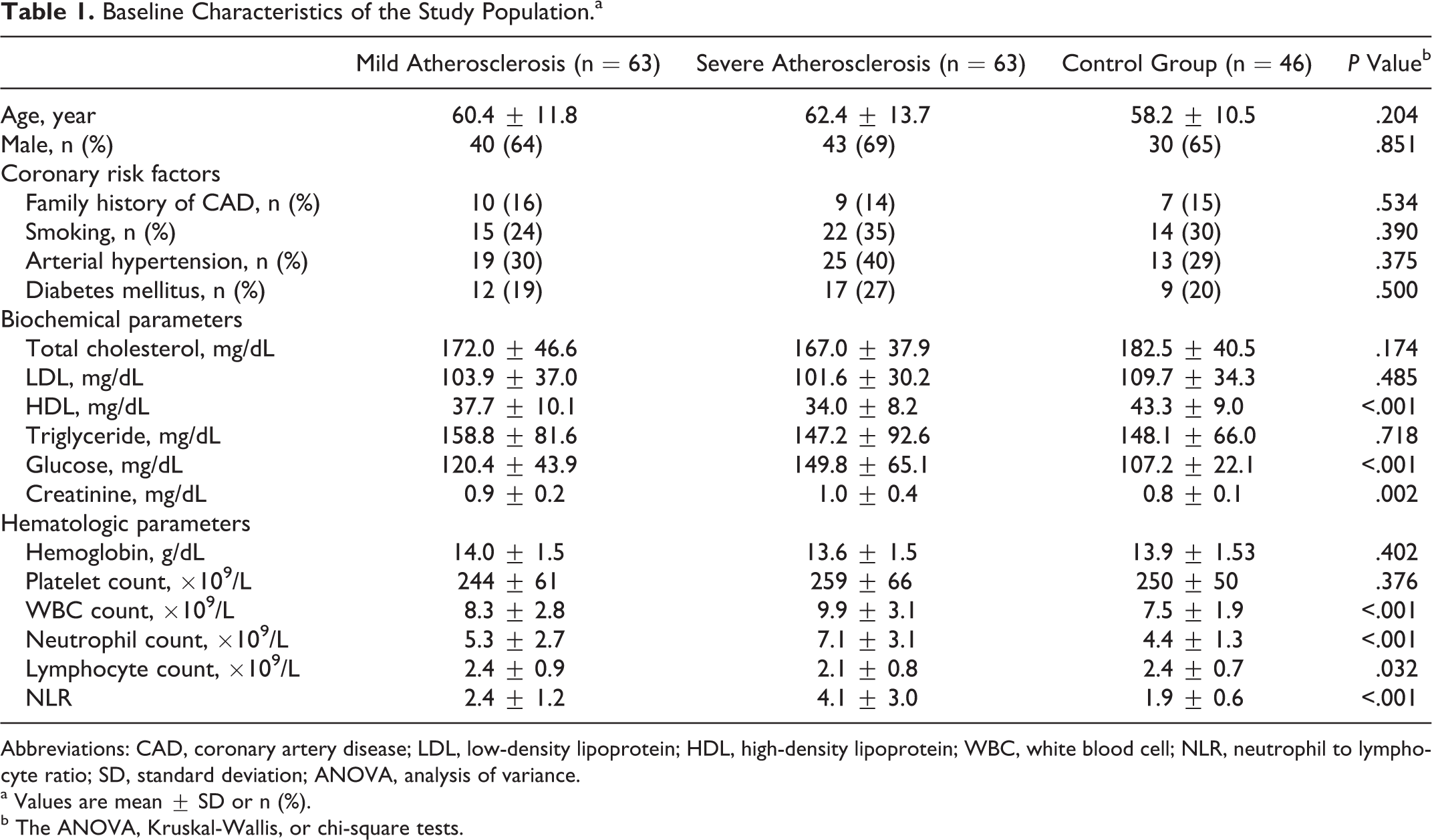
Abbreviations: CAD, coronary artery disease; LDL, low-density lipoprotein; HDL, high-density lipoprotein; WBC, white blood cell; NLR, neutrophil to lymphocyte ratio; SD, standard deviation; ANOVA, analysis of variance.
a Values are mean ± SD or n (%).
b The ANOVA, Kruskal-Wallis, or chi-square tests.
Hemoglobin and platelet counts were similar between groups. Compared with controls, patients with severe atherosclerosis showed a higher leukocyte (P < .001) and neutrophil counts (P < .001) and lower lymphocyte counts (P = .032) while mild atherosclerosis group did not differ. The NLR was significantly higher in severe atherosclerosis group compared with mild atherosclerosis and control groups (4.1 ± 3.0, 2.4 ± 1.2, and 1.9 ± 0.6, respectively, P < .001; Figure 1).
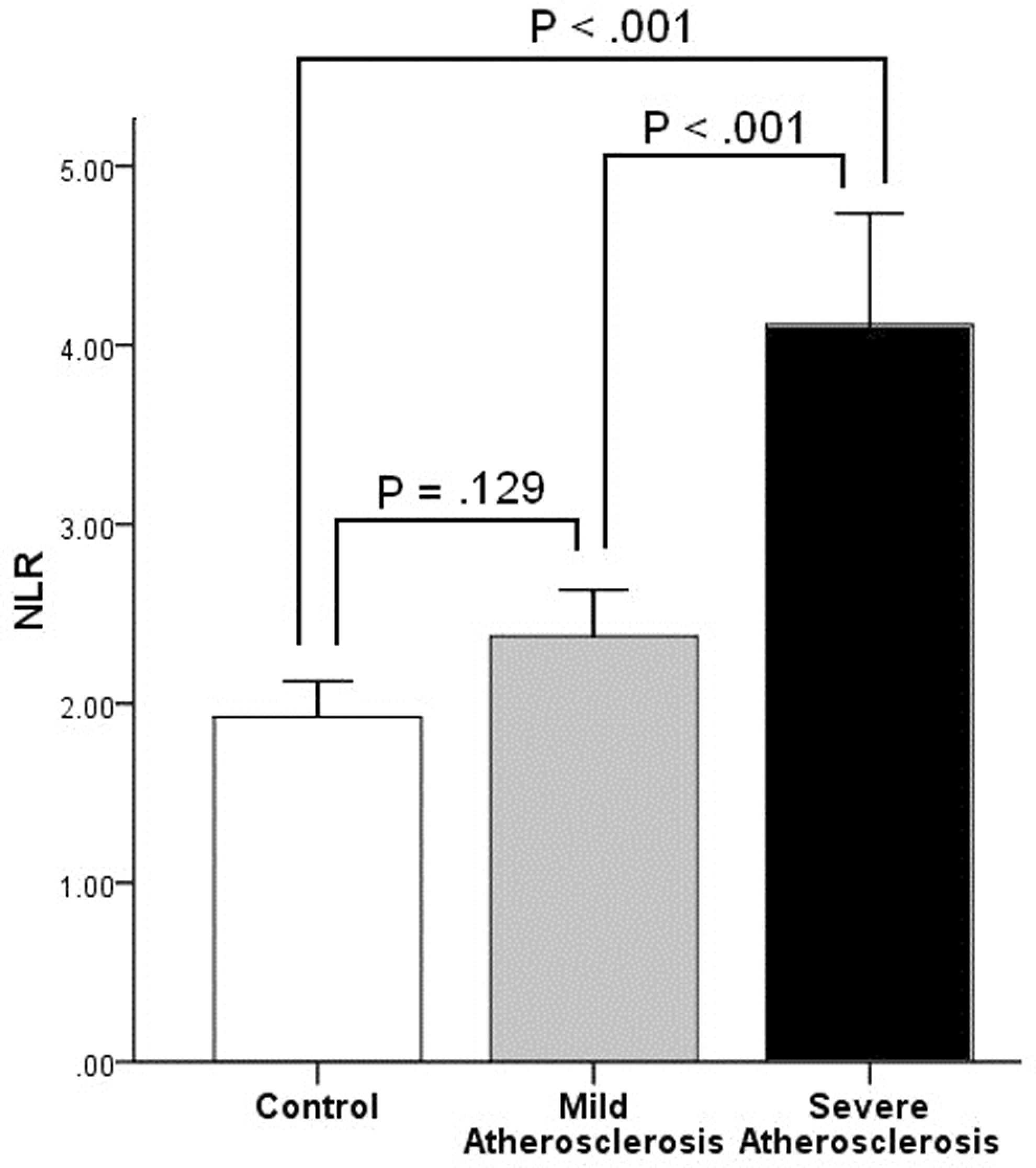
Neutrophil to lymphocyte ratio in members of the control, mild, and severe atherosclerosis groups.
In correlation analysis, NLR showed significant correlations between age (r = .165, P = .030) and Gensini score (r = .422, P < .001). Using a cutoff level of 2.5, NLR predicted severe atherosclerosis with a sensitivity of 62% and specificity of 69% (ROC area under curve: 0.730, 95% CI: 0.648-0.813, P < .001; Figure 2).
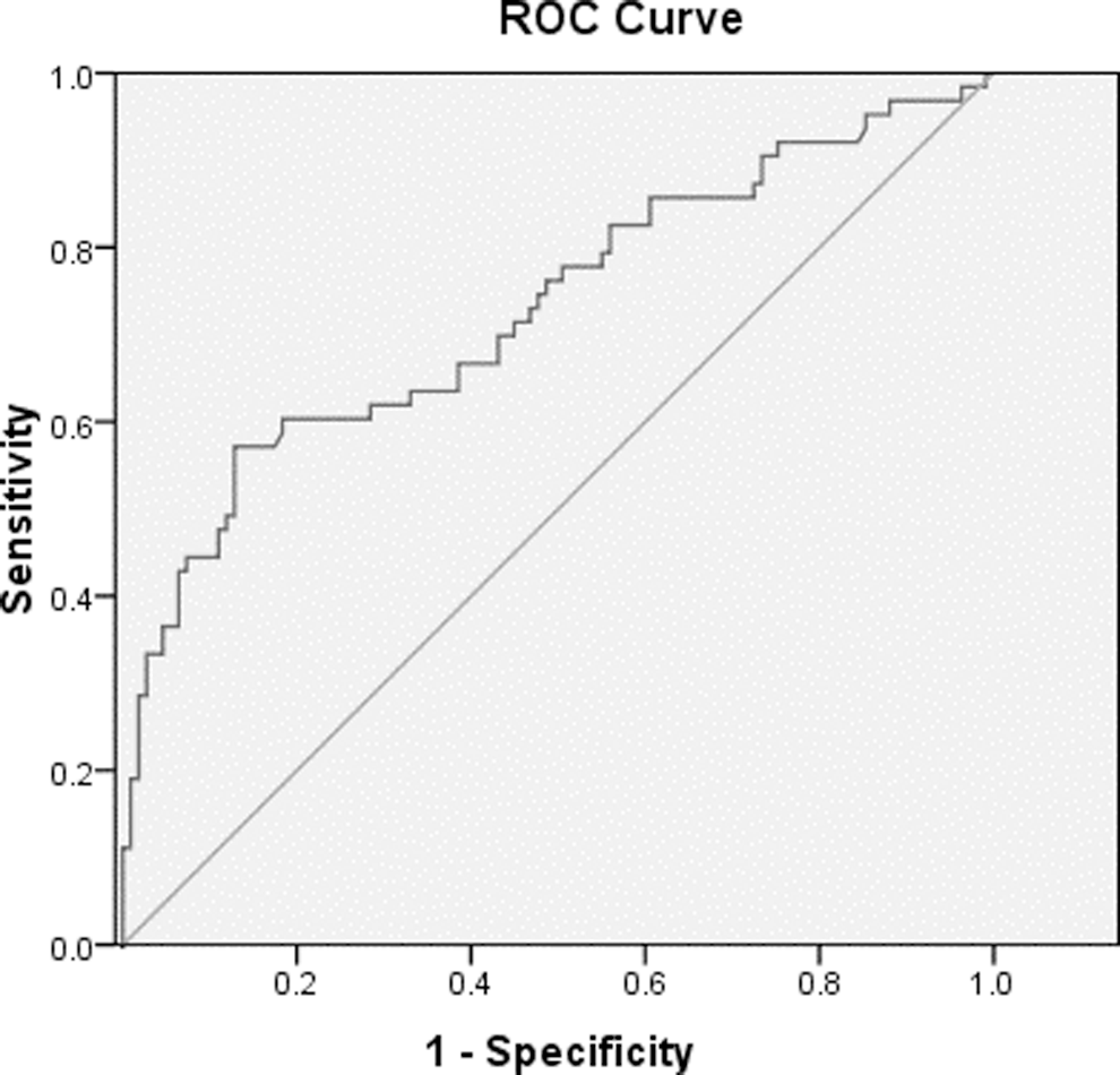
The receiver–operating characteristic (ROC) curve analysis of neutrophil to lymphocyte ratio for predicting severe atherosclerosis.
After multivariate analysis, high levels of NLR were independent predictors of severe atherosclerosis (OR: 1.798, 95% CI: 1.348-2.399, P < .001) together with glucose (OR: 1.010, 95% CI: 1.002-1.017, P = .020) and HDL (OR: 0.927, 95% CI: 0.884-0.971, P = .001; Table 2).
Multivariate Logistic Regression Analysis to Assess Predictors of Severe Atherosclerosis.
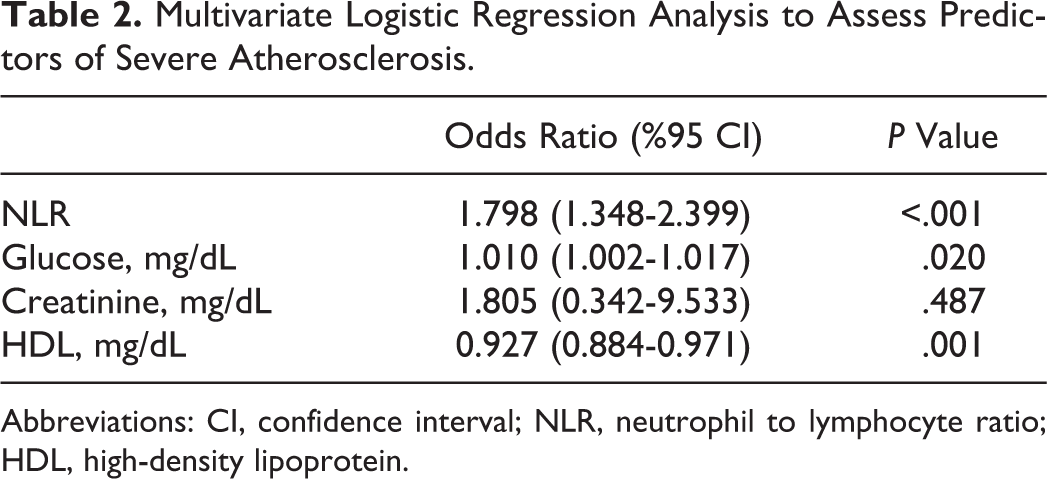
Abbreviations: CI, confidence interval; NLR, neutrophil to lymphocyte ratio; HDL, high-density lipoprotein.
Discussion
In the present study, we demonstrated the independent association between NLR and severity of coronary atherosclerosis, which were measured using Gensini scores in patients undergoing coronary angiography. There was a correlation between NLR and Gensini scores. Moreover, our study showed that an NLR >2.5 predicted severe atherosclerosis with a sensitivity of 62% and specificity of 69%. To our best knowledge, our study is the first report focusing on the relationship between NLR and the severity of atherosclerosis.
The development and progression of atherosclerosis is a multifactorial process. Inflammation plays a major role at all stages of atherosclerosis from initiation through progression and finally in the thrombotic complications of this disease. 2,14 White blood cell count and its subtypes have been investigated as inflammatory biomarkers to predict future adverse cardiovascular events. 3,4 Increased number of circulating neutrophils and decreased lymphocytes are risk indicators of future cardiovascular events. 15,16 Elevated NLR integrates the predictive risk of these 2 leukocyte subtypes into a single risk factor. 7 Recently, NLR has emerged as new prognostic marker. 5
Several studies have shown a relationship between NLR and CAD. It has been shown that NLR measured on admission was an independent predictor of adverse cardiac events in patients with ACS 7,17 and stable CADs. 6 Of note, Gibson et al 9 have shown that NLR associated with a poorer survival after CABG. Similarly, Duffy et al 8 showed that preprocedural NLR was an independent predictor of all-cause death in patients undergoing percutaneous coronary interventions. Horne et al 4 demonstrated that NLR was confirmed to be an independent predictor of death/myocardial infarction in patients with CAD. Kalay et al 18 investigated the determinants of progression of coronary atherosclerosis and showed NLR as a predictor of progression.
Similar to previous studies, our current study has confirmed the relationship between NLR and CAD. However, there have been no reports on association between severity of atherosclerosis and NLR. In the present study, NLR was found to be an independent predictor of the severity of coronary atherosclerosis.
Papa et al 6 demonstrated that lower HDL was independent prognostic factor for mortality in patients with stable CAD. Yan et al 19 showed fasting glucose as a significant determinant of Gensini score in nondiabetic participants. In a recent study, Kocaman et al 20 showed that NLR was independently related with increased age, glucose, and serum uric acid levels. As shown in previous studies, we found that glucose, HDL, and NLR are independently related with severity of atherosclerosis.
Study Limitations
The main limitations of this study are the limited number of study participants, and participants were from 1 center rather than multiple centers and cross-sectional study design. We evaluated atherosclerosis only by coronary angiography. Angiography also has its limitations since only the lumen is displayed and the information it provides about the coronary plaque burden is not extensive. Therefore, further studies with intravascular ultrasound and coronary computerized tomography may provide more accurate information on the amount of coronary atherosclerosis. Another limitation of this study is that it provides no information regarding cause or effect relationship between NLR and atherosclerosis. Although we found significant associations, further studies are needed to investigate clinical significance of NLR on atherosclerosis.
Conclusion
To our knowledge, our study is the first report focusing on the relationship between NLR and the severity of atherosclerosis. We found NLR as a risk variable for severity of atherosclerosis, and NLR was correlated with Gensini score. Unlike many other inflammatory markers and bioassays, NLR is an inexpensive and readily available marker that may be useful for cardiac risk stratification in patients with CAD.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.