
Abstract
Keywords
Introduction
Since the first description of Virchow’s triad in 1856, significant advances have been made in the comprehension of hypercoagulable states. Inherited thrombophilias are some of the most readily available genetic tests in our health care system today, but they can be difficult to interpret. Each test has unique clinical and technical considerations. It is estimated that one or more thrombophilic states are present in a quarter of patients with deep vein thrombosis (DVT) but can also be found in a considerable proportion of healthy controls. The prevalence of factor V Leiden by itself in a caucasian population of less than 70 years of age with the first objective DVT in the absence of malignancy was 21% compared to 5% in healthy controls. 1 The exact role played by each inherited thrombophilia risk factor is unclear but in general is thought to be a complex interaction of gene–gene and gene–environment variables. At present, the screening of asymptomatic low-risk populations is not recommended due to issues of variable penetrance, high prevalence, and lack of evidence that prophylaxis of thrombophilias is effective.2,3 Recent studies have shown that thrombophilia testing does not reduce the risk of recurrence. 4 Moreover, thrombophilia testing is not entirely benign. Beyond the costs of the tests, which in Calgary, Alberta, Canada, are approximately $700 (CAD) for a complete thrombophilia panel, there are psychological and financial implications for participants with positive testing.5,6
At our center, physicians ordering thrombophilia tests are not required to provide the indication for testing, nor document whether or not informed consent has been received. Family physicians (FPs) order approximately 50% of all thrombophilia tests. The objective of this study was to understand, by using the Script Concordance method, the types of clinical circumstances that motivate FPs to order thrombophilia testing, and identify whether these factors are in agreement with expert opinion from the field of thrombosis and hemostasis. The Script Concordance method allows one to assess the respondent’s perception about the probability of an event in relation to that of the expert and has been used successfully to assess clinical reasoning in the context of uncertainty.7,8 We also wanted to assess the nature of counseling that FPs perform. Finally, we wanted to integrate an educational component in an effort to make thrombophilia ordering more evidence-based among study participants through the use of an educational Web site. We hypothesized that FPs would order more tests than thrombosis experts on the basis of the ease of testing availability, and that this would be inconsistent with expert opinion. Last, we hypothesized that pretest counseling would be infrequent.
Methods
A total of 835 FPs actively practicing (full time or part time) in the Calgary, Alberta, Canada health region were contacted by mail and electronically to participate in an online survey between March 2009 and March 2010. No compensation for participation was provided. The survey consisted of 2 sections: part A involved 5 hypothetical clinical scenarios for which thrombophilia testing might be considered (Table 1 ); in part B, the FPs self-reported the frequency and type of counseling they routinely performed in their offices. The survey was approximately 15 minutes long.
Description of Scripts Included by Scenario
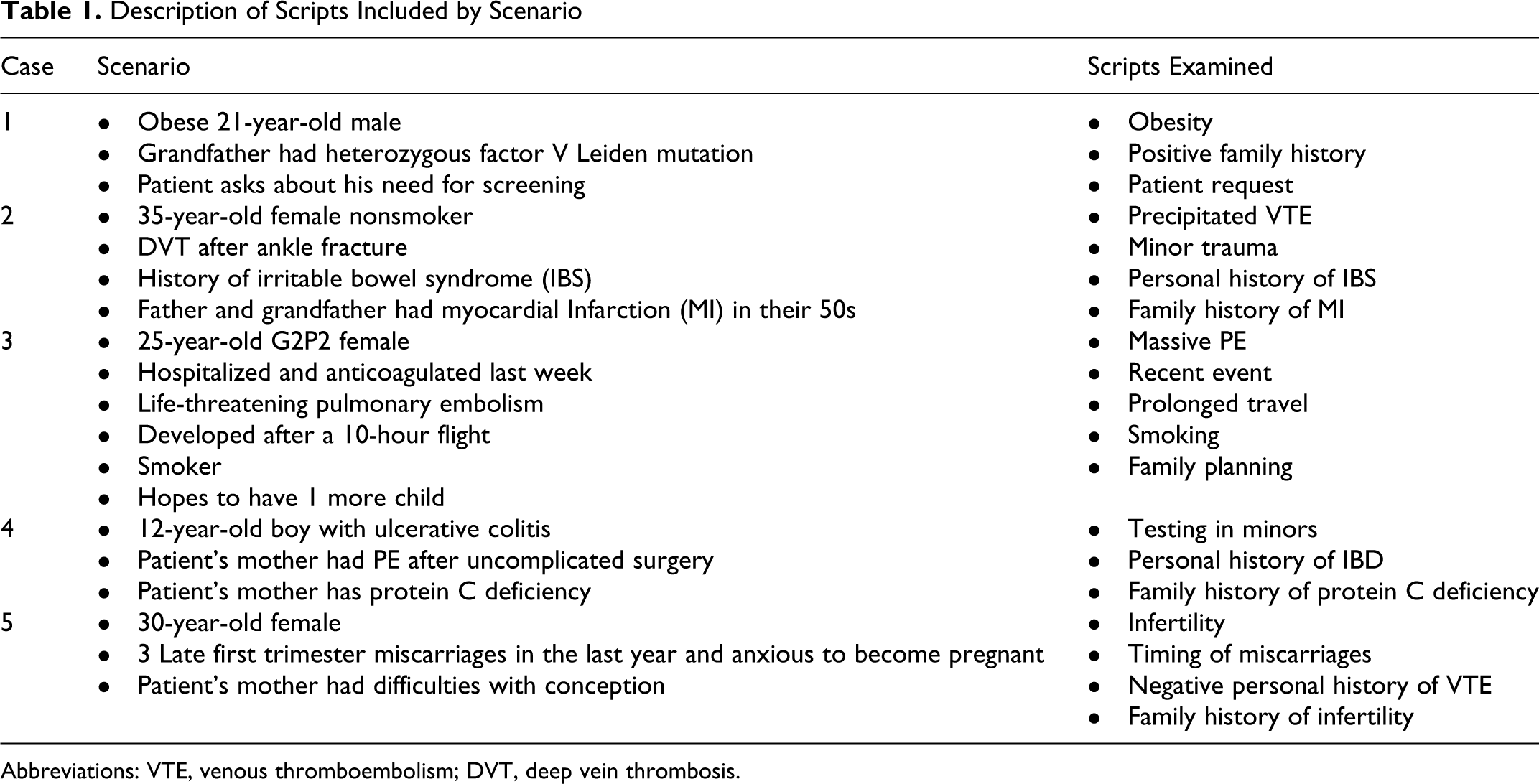
Abbreviations: VTE, venous thromboembolism; DVT, deep vein thrombosis.
Part A of the survey was also sent to 15 local and national experts in thrombosis and hemostasis selected by the research committee, including adult and pediatric hematologists as well as general internists with specialization in thrombosis and hemostasis. Selection of experts was based purely on the availability of contact information and known involvement in clinical care of thrombosis patients. The survey responses of these individuals comprised the expert response with which the FP responses were compared. The utility of and current evidence behind thrombophilia testing was not discussed with experts prior to their participation in the study.
The content of each clinical scenario was designed to look at specific indications for thrombosis testing such as positive family history, modifiable risk factors including long-distance travel and minor surgery, testing of minors, and fertility-related issues. After reading the clinical scenario, participants were asked to identify which, if any, of the available thrombophilia tests (Table 2 ) they would order for that particular set of circumstances. Respondents who chose the option “I don’t know” with respect to whether testing was indicated were excluded from analysis of that data set in an effort to ensure respondents were reasonably confident of their responses regarding appropriateness of testing. Physicians were then asked what factors in the case made them more or less likely to order testing according to the Script Concordance approach, which is used to assess clinical reasoning in the context of uncertainty. This approach allows one to assess the respondent’s perception about the probability of an event in relation to that of the expert. This technique, based on script theory, was first created in 2000 and has subsequently been validated in several medical disciplines. 9 Script concordance utilizes clinical vignettes, which might readily be encountered in real-world medicine, to examine different knowledge sets, also termed scripts, such as investigation or diagnosis that one might utilize to solve a problem. The scoring system of the test is used to identify what knowledge gaps might exist between examinees and expert panels. In this way, we assessed the clinical reasoning of FPs in relation to thrombosis and hemostasis experts.
Thrombophilia Tests Available in Calgary, Alberta, Canada
After completing the survey, participants were provided with a link to a Web site (www.ucalgary.ca/thrombophilia) developed by the investigators and reviewed by experts. It was designed to provide immediate feedback for participants as part of an educational initiative to raise awareness about the complexities of thrombophilia ordering in the Calgary region. This Web site included a statistical summary of expert responses for each scenario as well as a brief literature review of each topic.
Statistical Analysis
Data were first summarized by calculating frequencies and percentages for each variable for both groups of participants. The FP and expert responses were then compared using chi-square test (Fisher exact test for low cell counts). The FP responses to topics counseled before and after testing were compared first using chi-square tests and again using Wilcoxon rank sum tests to preserve the ordinal scale of the responses (ie, 1 = Never; 2 = Sometimes; 3 = Often; and 4 = Always). A significance level of .05 was used for all analyses. All results were calculated using SAS (version 9.2).
Results
Eighty-four FPs (11% of those solicited) completed the survey, while 100% (n = 15) of expert survey responses were collected. The results of part A of the survey are summarized in Table 3 . The FPs indicated a preference to refer 35.9% of all cases to hematologists. Referral rates differed significantly by clinical scenario (P = .028), with the third scenario being most commonly referred (odds ratio [OR] = 1.77 [1.24, 2.54]. A mean of 15.9% of FPs indicated “I don’t know” in response to the question “Is testing indicated?” in each scenario and were excluded from analysis of that question. No experts were excluded. In 2 of the 5 scenarios, there was disagreement between groups as to whether testing was indicated (P ≤ .037). In both scenarios, FPs responded that testing was indicated more frequently than experts. However, the number of tests ordered in each scenario did not differ greatly by physician group. In the first scenario only, differences in testing patterns reached statistical significance. Specifically, the FPs ordered on average 1 more test than experts (P = .007). There was a wide variation between respondents in the number of tests ordered per scenario with large standard deviations. If testing was chosen, FPs tended to order complete panels. In scenario 1 through 3, on average, more than 4 of the possible 6 tests were ordered by those who felt testing was indicated. Testing was somewhat more selective in scenario 4 and 5, with a mean of 2.03 and 3.31 tests ordered, respectively, by FPs who chose to test. This pattern of ordering was also seen among experts.
Summary of Results From Part A of the Survey as Listed by Scenario
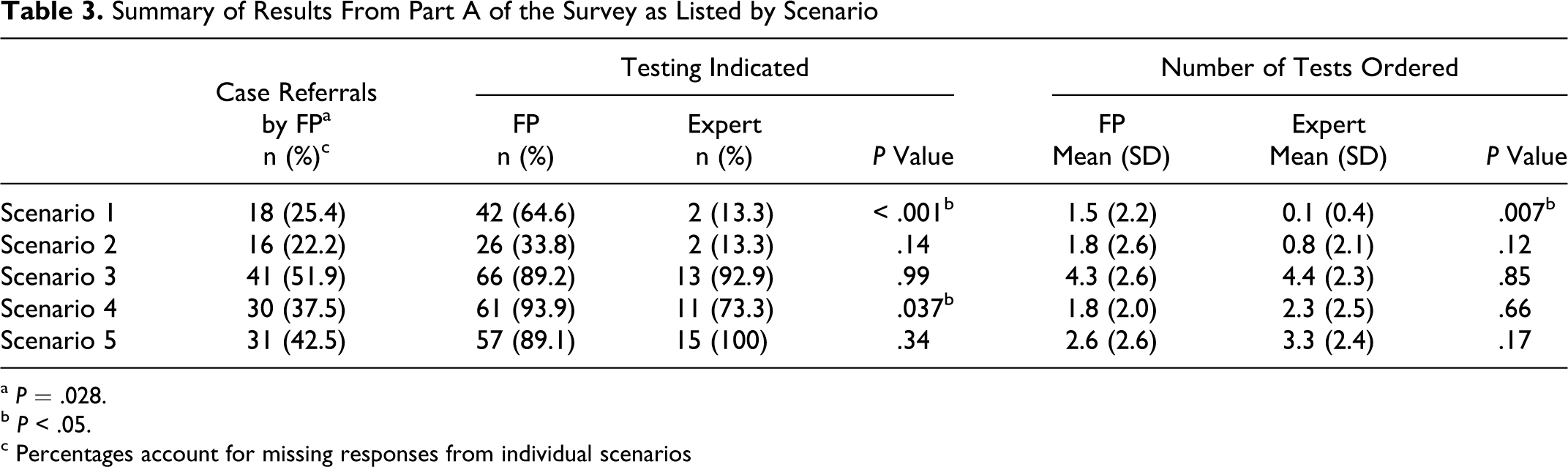
a P = .028.
b P < .05.
c Percentages account for missing responses from individual scenarios
The effect of different scripts on physician testing is presented in Figure 1. Seven of the 20 chosen scripts affected testing patterns differentially. Compared to experts, FPs were significantly more likely to test male, obese, or pediatric patients, patients with a family history of myocardial infarction or infertility, and patients with a recent event compared to experts (P ≤ .043). The FPs were significantly less likely to test patients with a venous thromboembolism (VTE) in the context of prolonged travel (P = .038).
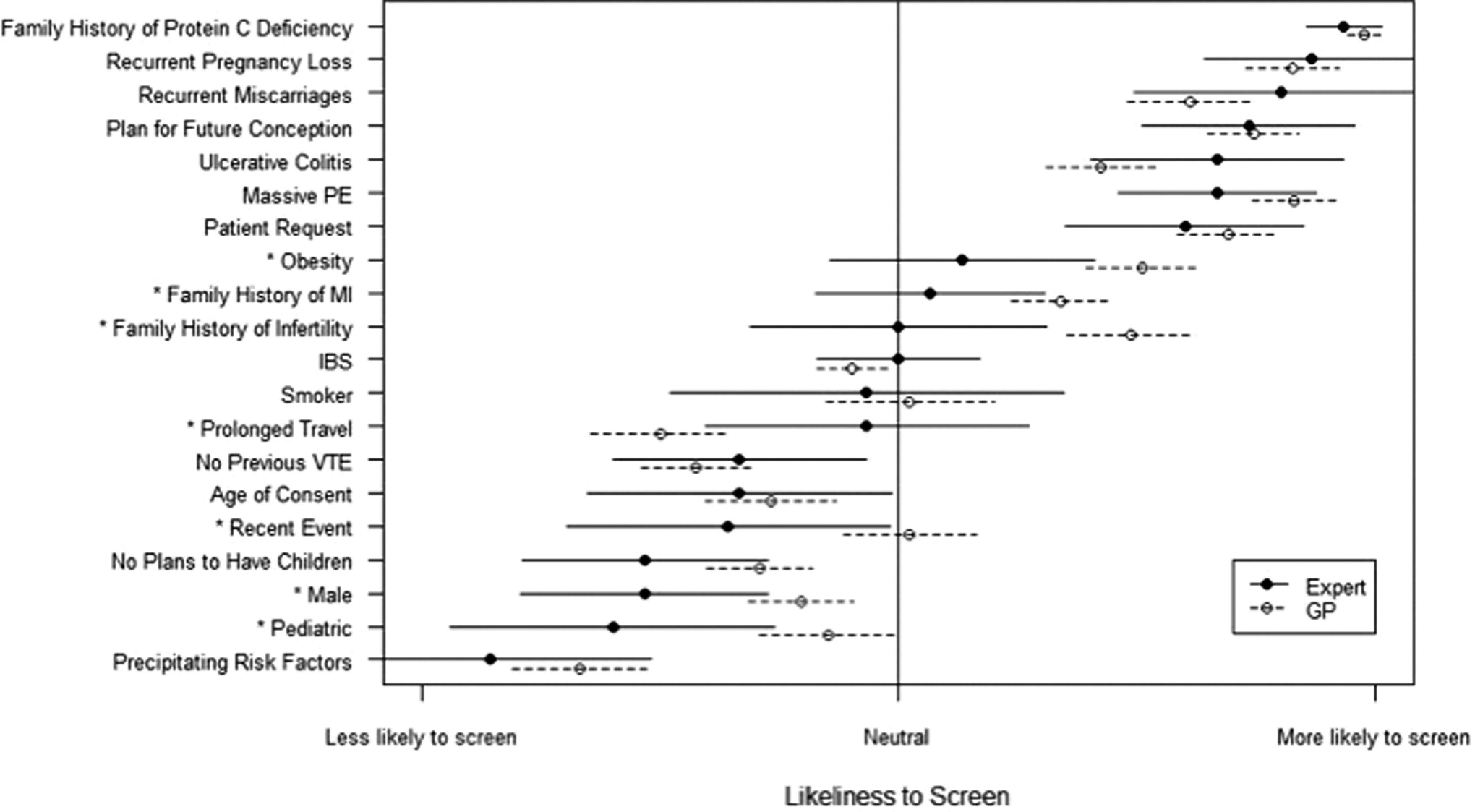
Effect of individual scripts on likelihood to order thrombophilia testing. *P < .05. PE indicates pulmonary embolism; MI, myocardial infarction; IBS, irritable bowel syndrome; VTE, venous thromboembolism; GP, general practitioner.
Counseling patterns are presented in Figure 2. The FPs most frequently reported counseling about implications for oral contraceptive pill (OCP), risk of recurrent VTE, and family testing. Topics infrequently discussed included implications for life insurance or getting mortgages. In 4 of 7 counseling topics, the FPs were statistically more likely to counsel patients after testing had been carried out and positive results returned. This trend existed in all remaining topics but did not meet statistical significance.
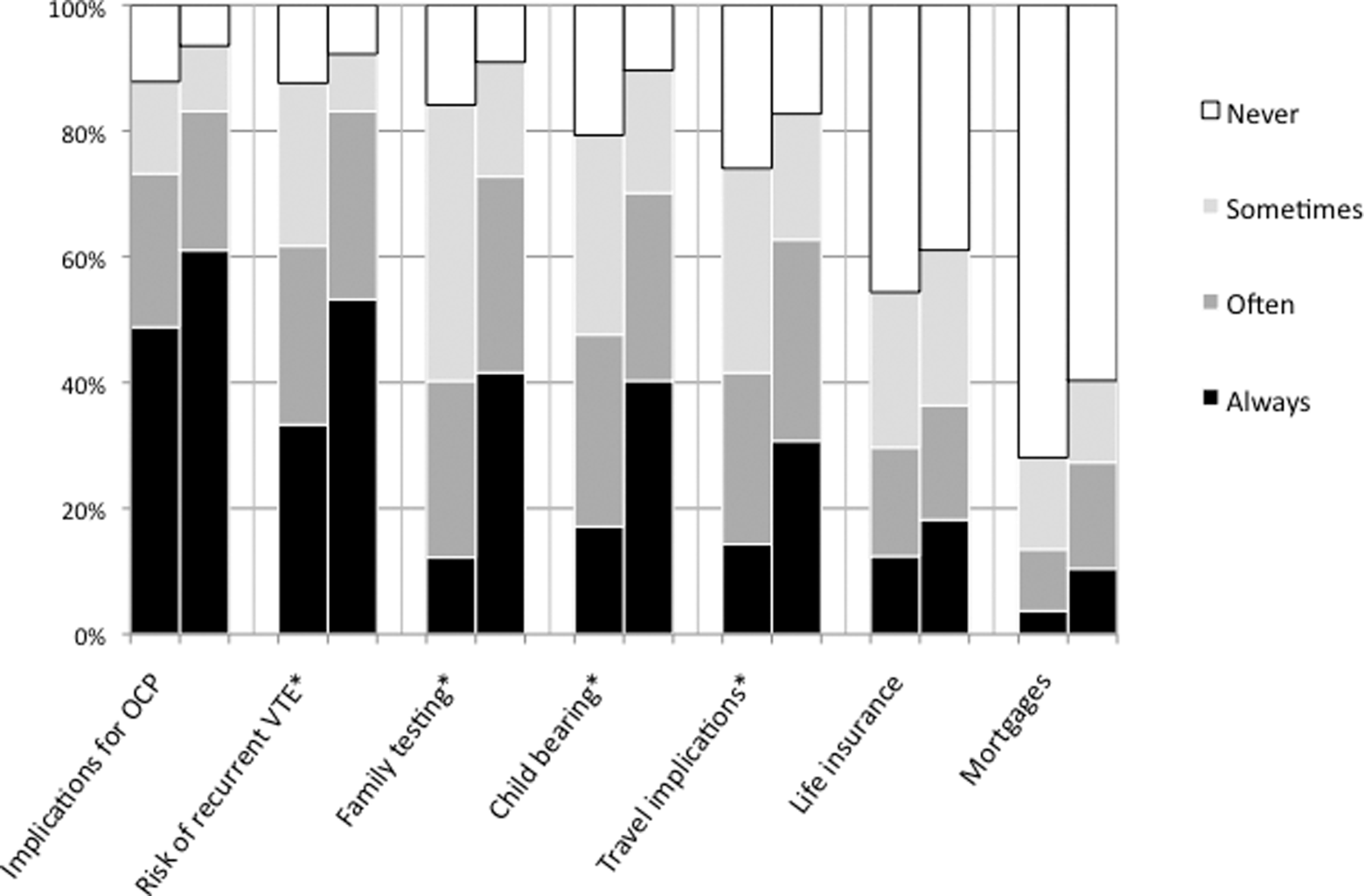
Counseling patterns in FPs offices before and after thrombophilia testing (left and right column respectively). *P < .003.
Discussion
Currently, the utility of routine thrombophilia testing remains highly controversial even among experts in the area. Indications for testing may be very unclear for physicians who see only a few cases each year. While one of our objectives was not to provide guidelines for routine thrombophilia testing, we wanted to measure in a practical way how similar or different experts and FPs were in their assessment of possible clinical scenarios. The ordering practices of FPs in our hypothetical cases did not correlate with expert opinion with 2 of 5 clinical scenarios resulting in disagreement. In both cases, FPs responded that testing was indicated when experts did not. In our small study, this did not translate into significantly increased resource utilization on a laboratory level, but our study may have been underpowered to examine resource usage. A considerable percentage of those surveyed responded with “I don’t know” to the question of testing indication, and over one third chose to refer hypothetical patients to hematologists. This finding may indicate lack of familiarity with thrombophilia testing in certain clinical circumstances. We did not examine why FPs chose to refer patients, but possible explanations include inadequate appointment time for complex scenarios and counseling, or perhaps low frequency of clinical encounters leading to discomfort with current evidence for thrombophilia testing.
This study also had the added unintentional benefit of exploring the differences in expert responses. In all but 1 scenario (scenario 4), more than 85% of the experts agreed on the basic question of whether testing was indicated. We felt this was an adequate degree of agreement to make the comparison with FPs meaningful. However, there was only complete agreement in 1 of the 5 scenarios, which likely speaks to the complexity of the hypothetical scenarios and the lack of evidence-based guidelines for thrombophilia testing. The small size of the expert population of only 15 in our study makes it difficult to generalize this level of agreement on thrombophilia testing among experts as a whole.
The motivations behind thrombophilia testing are not always clear. In a recent study from the Netherlands, ordering physicians indicated that 20% of the tests they sent were done for a patient with a single VTE. In 24% of all tests sent, regardless of indication, there was no influence of testing on the patient regardless of whether it was positive or negative. 10 Overall, our study showed a considerable level of discomfort among FPs for thrombophilia testing.
With respect to case scripts, there were several clinical factors that were handled differently by FPs as compared with thrombosis experts. Currently, the degree of correlation between nonexperts and experts required to denote competency in an area is unknown. However, the use of script concordance to assess learning has been shown in studies of immediate impact to improve clinical reasoning and participant knowledge. Research in this area is ongoing. 11
This study is one of the first to our knowledge that looks at specific patterns of knowledge for thrombophilia testing using the script concordance method. It allowed us to identify factors that may be motivating FPs to order testing in a nonevidence-based manner. For example, FPs were less likely to test patients with VTE in the context of prolonged travel. However, it has been shown that there is a high prevalence of thrombophilia states in participants who acquire VTEs while travelling over long distances. In the LONFLIT study, which looked at flights over 10 hours, no VTE were identified in 355 patients without additional risk factors such as previous DVT, documented coagulation disorders, or neoplasms, suggesting that prolonged travel merely uncovers underlying risk factors and in and of itself is not enough of an explanation for development of VTE. 12 A second study identified thrombophilia in 72% of patients with travel-related VTE. About 30% of these patients had factor V Leiden mutation. 13
This study demonstrates how research can be used to make continuing medical education more accessible for different populations of physicians. It is neither practical nor reasonable to expect FPs to learn the entire body of evidence around thrombophilia testing when there are many other areas of medicine that may be more common or relevant to their practice. Instead, the script concordance method allows us to identify “common pitfalls” in thrombophilia testing, so that education can be targeted to key areas where FPs tend to practice differently from experts. For example, this research could be used to create educational guides regarding the utility of thrombophilia testing in patients with VTE after prolonged travel, or the cost-effectiveness of delaying thrombophilia testing after recent events. In this study, we provided immediate educational feedback through a linked Web site while the case scenarios were still fresh in mind.
Finally, self-reported counseling patterns showed a clear predilection for discussion after receipt of testing results. This pattern may reflect the efficiency required for FP offices. Lengthy discussion of test implications may not be useful if testing is ultimately negative. However, thrombophilia testing can cause harm. It may induce significant anxiety and impact patient costs including life insurance.14–16 Hellmann et al found that 64% of patients stated that they had not received adequate information prior to factor V Leiden testing, with 68% still having many questions after testing was sent. 17 Our study highlights the need to make genetic counseling convenient for real-world medicine use so that it better correlates with the ease of test ordering. The reasoning behind failure to counsel prior to testing merits further study including initiatives designed to improve informed consent from patients.
There were several limitations to the current study. Most notably, there was a low response rate from FPs. This may have been due to the length of survey, lack of participation incentive (other than educational credits), or the limited ability to advertise. Efforts to increase study participation included attendance at FP meetings with paper handouts and e-mail reminders in local FP newsletters. It is difficult to speculate how this may have affected the study results. We collected a number of informal reviews of the survey from FPs alongside the survey. Comments ranged from FPs indicating complete familiarity with these clinical scenarios to those who felt the survey was far too specialized to be relevant to general family practice. Therefore, we would speculate the participants included physicians with varying levels of comfort with the material and that it can at least be extrapolated to a larger population of FPs with varying levels of comfort. Additionally, not all FPs in our region are involved in primary care and may not find the survey relevant for completion. This data is unavailable to us but would imply that the response rates among those actually practicing primary care was higher than 11%. Because of the low participation rates, it is difficult to generalize the results of this survey to all FPs. Moreover, the utility of testing may be different among low prevalence populations. The study does however indicate that thrombophilias are an area of genetic testing that merits further investigation. Until patterns of thrombophilia testing can be shown to be similar between physician groups, it may be advisable to limit access to testing or provide guidelines with which to order thrombophilia testing. Algorithms have recently been published for this purpose. 18 Last, the survey was self-reported and was subject to recall bias.
Given the paucity of evidence for understanding how thrombophilias interact with other clinical factors and the exact role played by each thrombophilia in VTE, thrombophilia testing remains a very difficult area of medicine to navigate. Using the strategy employed by this survey, one may be able to identify specific pieces of knowledge motivating those ordering thrombophilia tests to create educational initiatives to better align testing patterns with current evidence. Whether such initiatives can impact the usefulness of thrombophilia testing remains to be seen, and more study in this area is encouraged.
Conclusion
Disagreement exists between FPs and thrombosis experts about appropriate indications for thrombophilia testing. The script concordance method can be used to identify differences in clinical reasoning in an effort to create targeted educational initiatives. Self-reported lack of pretest counseling among FPs warrants further study.
Footnotes
Acknowledgments
We thank Farah Khandwala, MSc, who performed our statistical analysis, Herta Fidler, who helped in the initial phases of the project and with statistical revisions, Hassan Dibadj who provided feedback on statistical analysis, and Annabella Montero who was of great assistance in creating our educational website.
Declaration of Conflicting Interests
The author(s) declared a potential conflict of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported in part by the Calgary Laboratory Services research and development fund. The funder does not have an influence on the design and conduct of the study.