
Abstract
The utility of thrombophilia testing in clinical practice is still a matter of debate because studies have not shown a benefit in the reduction of recurrent venous thromboembolism (VTE) risk in patients with thrombosis, despite the clearly higher VTE risk for first thrombosis. Screening for thrombophilia is indicated in selected patients. Particularly in selected young patients, especially women of childbearing age, the knowledge of the genetic thrombophilic defect may help in specific situations to decrease the risk of VTE events. Avoidance of modifiable risk factors and/or prophylactic thromboembolic procedures may be evaluated in selected patients. A comprehensive workup including personal and familial history, clinical examination, and laboratory test results including hereditary thrombophilia remains helpful in assessing the cumulative risk and the management of this group of selected patients.
Introduction
Thrombophilia is an imbalance in hemostasis with an increased tendency to form intravascular pathologic venous or arterial thrombus. Predisposing factors for venous thrombosis are inherited or acquired, and venous thromboembolism (VTE) is considered a multifactorial disease. 1 The so-called Virchow triad describes the factors contributing to VTE, including endothelial injury or activation, reduced blood flow, and hypercoagulability of the blood. The latter is often present on the basis of an inherited genetic predisposition. On the other hand, a genetic predisposition is not like illness. Not all patients with such mutations of coagulation factors will develop VTE throughout life. Therefore, diagnosing a prothrombotic state in clinical practice is difficult and it is usually done only after a VTE. In addition, screening for inherited thrombophilic conditions in clinical practice is still a matter of debate because studies have not shown a benefit in the reduction of recurrent VTE risk in patients with thrombosis, despite the clearly higher VTE risk for first thrombosis.
Although evidence suggests in specific situations against screening tests, patients may be anxious and unwilling to skip the thrombophilia screening. In the situation where the patient is willing to know the risk for—or the cause of—VTE, the physician may have difficulty to reconcile 2 different opinions. We believe that guidelines for thrombophilia screening are helpful for clinical decisions and may help to reduce tests that are not indicated. In this review, we discuss indications for screening in selected patients with VTE based on consensus guidelines and personal experience.
Inherited Thrombophilia
Inherited thrombophilia is a genetic predisposing condition to VTE. The clinical manifestations of inherited thrombophilia are heterogeneous concerning severity and type of events. Manifestations consist of superficial thrombophlebitis, VTE on classical (deep venous thrombosis of the legs, pulmonary embolism) or atypical localizations (splanchnic, hepatic, upper limbs, cerebral venous thrombosis), and complications of pregnancy or puerperium.
In the past 50 years, our knowledge on the etiology of VTE has improved, starting in 1965 with the first description of inherited thrombophilia caused by antithrombin deficiency. 2 The deficiency of this naturally occurring anticoagulant protein was for many years the only identified cause of inherited thrombophilia. Over time the description of protein C deficiency, 3 protein S deficiency, 4 activated protein C resistance associated with a point mutation in the factor V gene, 5 and prothrombin gene mutation 6 improved our knowledge of the pathogenesis of VTE. Following the discovery of these proteins, the possibility to identify an inherited cause in patients with VTE increased (Table 1). 7 For example, it was reported recently that missense mutations in the gene encoding prothrombin corresponding to Arg596 cause antithrombin resistance and thrombomodulin resistance-related thrombophilia. 8 Other genetic risk factors for VTE are dysfibrinogenemia (FGG, fibrinogen γ′), 11 F11 gene, 9 and non-O blood group. 12 –14 The initial observation that an elevated factor VIII level is a risk factor for venous thrombosis 15 is now supported by robust evidence. Over the past years, research to identify genetic variants associated with VTE focused on hundreds of single-nucleotide polymorphisms. 16 Recently, a genome-wide association study approach led to the identification of 2 VTE-associated loci, TSPAN15 and SLC44A2. The odds ratio for VTE are 1.31 for TSPAN15 and 1.21 for SLC44A2. 10
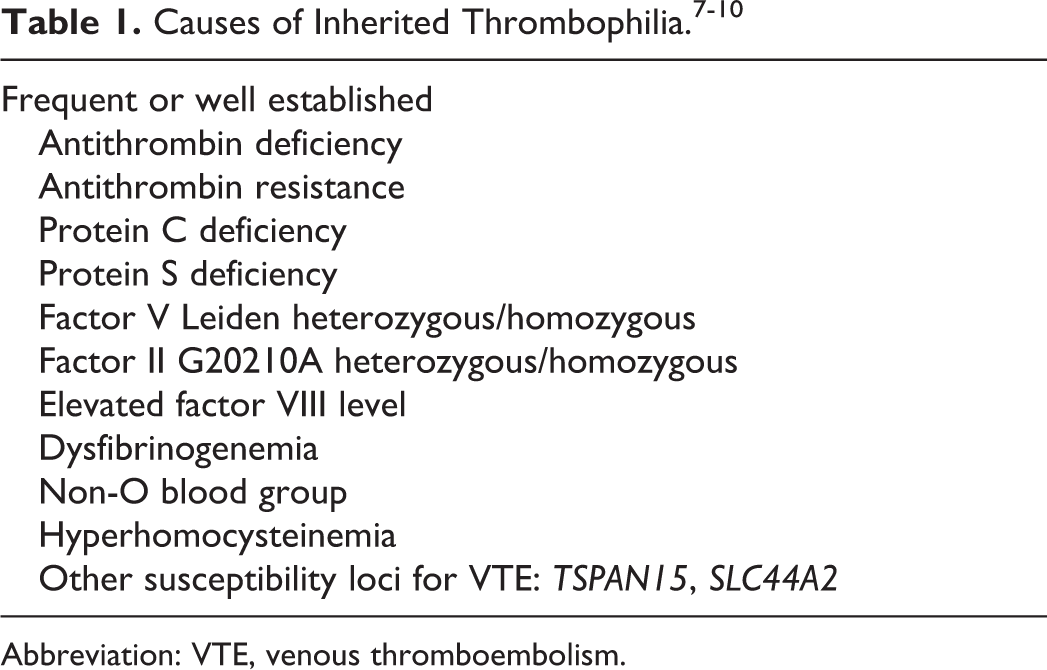
Abbreviation: VTE, venous thromboembolism.
Inherited thrombophilia affects the risk of a first thrombosis lifelong. However, the first episode of VTE occurs frequently at a young age (before 40 years) without apparent causes. Gradually, clinical studies elucidated the role of inherited thrombophilia in first and recurrent VTE. Over time it became evident that these inherited risk factors impact differently the relative risk for the first 17 –24 and recurrent VTE (Table 2). 25 –35
Main Thrombophilic Defects: Relative Risk of First and Recurrent VTE.
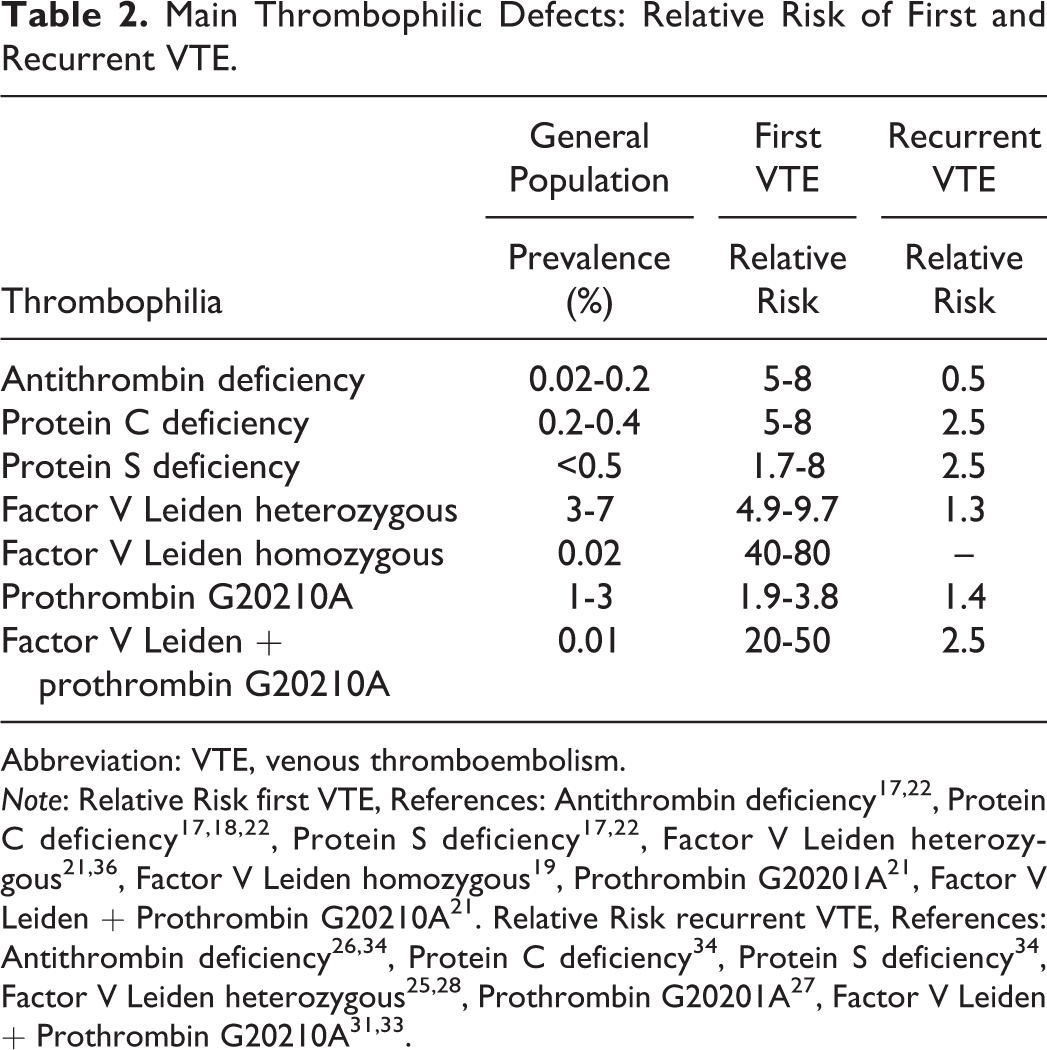
Abbreviation: VTE, venous thromboembolism.
Note: Relative Risk first VTE, References: Antithrombin deficiency 17,22 , Protein C deficiency 17,18,22 , Protein S deficiency 17,22 , Factor V Leiden heterozygous 21,36 , Factor V Leiden homozygous 19 , Prothrombin G20201A 21 , Factor V Leiden + Prothrombin G20210A 21 . Relative Risk recurrent VTE, References: Antithrombin deficiency 26,34 , Protein C deficiency 34 , Protein S deficiency 34 , Factor V Leiden heterozygous 25,28 , Prothrombin G20201A 27 , Factor V Leiden + Prothrombin G20210A 31,33 .
Acquired Thrombophilia
Clinical evidence supported the hypothesis that VTE is due to interactions of inherited and/or acquired thrombophilic traits (Table 3). 1,37 –39 The thrombotic event is the final clinical sign of interactions of single or multiple genetic and/or acquired predisposing factors such as age, elevated body mass index (BMI), immobility, trauma, use of oral contraceptives or hormone replacement therapy, and pregnancy–puerperium. Evidence concerning the role of other risk factors or diseases in VTE is growing (Table 3). Contribution of these modifiable factors on VTE is variable during different age segments and depends on acquired risk factors, which can overcome a threshold resulting in VTE.
Causes of Acquired Thrombophilia.
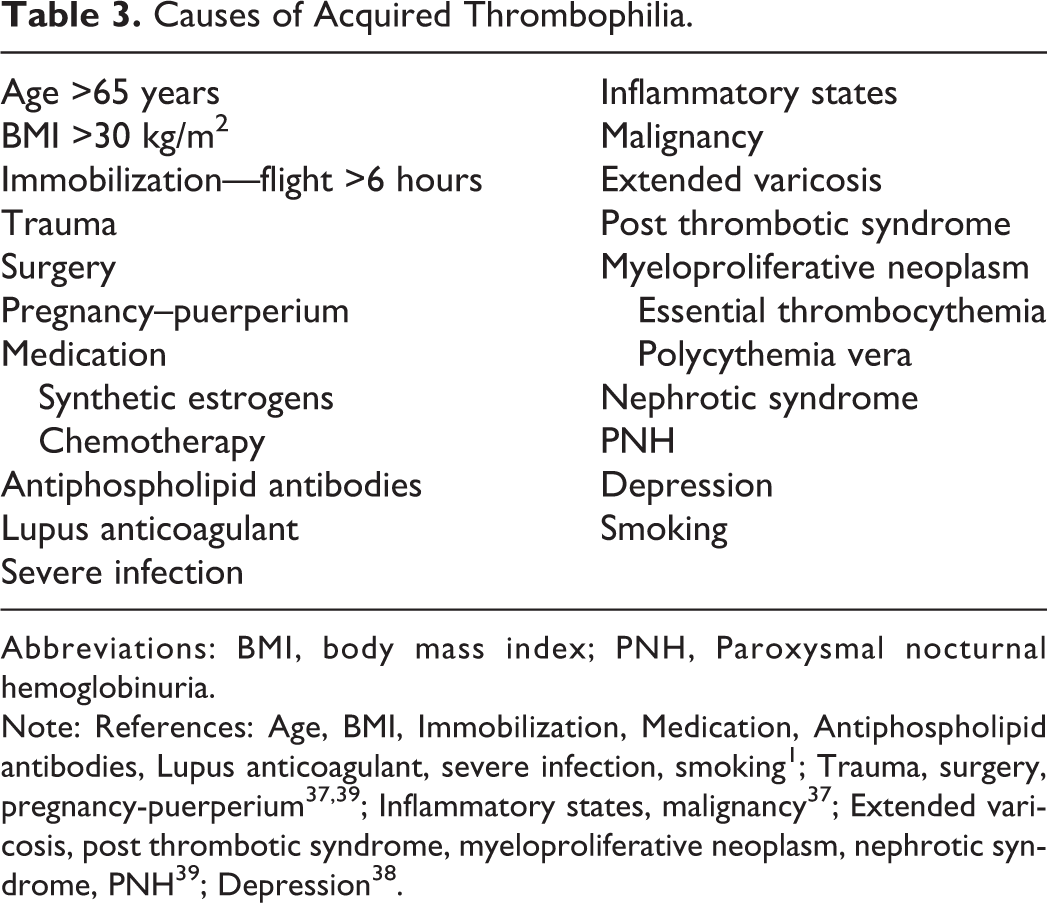
Abbreviations: BMI, body mass index; PNH, Paroxysmal nocturnal hemoglobinuria.
Note: References: Age, BMI, Immobilization, Medication, Antiphospholipid antibodies, Lupus anticoagulant, severe infection, smoking 1 ; Trauma, surgery, pregnancy-puerperium 37,39 ; Inflammatory states, malignancy 37 ; Extended varicosis, post thrombotic syndrome, myeloproliferative neoplasm, nephrotic syndrome, PNH 39 ; Depression 38 .
Universal or Selected Thrombophilia Screening?
Idiopathic VTE is a diagnosis of exclusion by ruling out known causes. In young patients, diagnosis of idiopathic VTE should be done or ruled out because it has important consequences concerning the duration of therapy. Therefore, we suggest thrombophilia screening in selected patients with VTE, selective family member, and against an universal screening. To argue against thrombophilia screening in any case is contrary to medical knowledge and to helpfulness to the patients. Thrombophilia screening should be a comprehensive evaluation of patient’s prothrombotic state. A merely laboratory analysis without careful consideration of personal and familial anamnesis, past clinical history, acquired risk factors for VTE, associated diseases, prognosis, and therapy’s adverse effects does not reflect the screening sense. Accordingly, testing all women at random before prescribing estrogen medications (oral contraceptives or hormone substitution) is not indicated. 40
Patients With First Symptomatic Venous Thrombosis
Because the prevalence of thrombophilic defects in the general population is low (Table 2), testing for heritable thrombophilia in unselected patients with a first episode of VTE is normally not indicated. 41,42 In line with the model of multifactorial nature of VTE, according to which the thrombotic event is the sum of multiple gene–gene and gene–environment interactions, inherited thrombophilia interacts with other established acquired predisposing factors for VTE (Table 3). 43,44 Recognition of gene–gene and/or gene–environmental interactions may be important in selected patients for therapeutic decisions and for prevention of VTE in patients and family member. The most common inherited thrombophilic defects (deficiency of antithrombin, protein C, protein S, activated protein C (APC) resistance due to factor V Leiden mutation, and prothrombin G20210A mutation) and hyperhomocysteinemia are diagnosed in about 50% of patients with VTE. Non-O blood group is the commonest mild genetic risk factor for VTE and is associated with an approximately 2-fold increase in VTE risk. 12 –14 Not all patients with an inherited thrombophilia develop a VTE, but the risk becomes particularly high in the presence of additional acquired risk factors. In this setting, the risk of VTE may increase in a multiplicative way.
Pregnancy- and Puerperium-Associated VTE
The physiological changes in hemostasis and the physical changes in women during pregnancy are responsible for a prothrombotic state and an increase in blood stasis. These result in an increased risk of VTE during pregnancy. The antenatal VTE risk in pregnant women is at least 4-fold higher (5-10 fold) compared to age-matched nonpregnant women. The antenatal VTE risk is further increased in cases of BMI ≥30 kg/m2, age >35 years, multiple births, and varicose veins. The postpartum VTE risk is 2- to 5-fold higher compared to antenatal and up to 20-fold (15-35 fold) compared to age-matched nonpregnant women. The risk is high for 6 weeks postpartum and returns to baseline at 12 to 18 weeks postpartum. The postpartum VTE risk is further increased in cases of BMI ≥25 kg/m2, cesarean delivery, obstetrical hemorrhage, and preterm delivery (<36 gestational weeks). 45 –49 The rate of VTE complicating pregnancy and puerperium among women with antithrombin, protein C, and protein S deficiency is 37.8%, 14.7%, and 17.1%, respectively. 50 The risk of VTE during pregnancy and puerperium increases 8-fold in women with a deficiency of natural coagulation inhibitors. The risk is particularly high in cases with positive family history (Table 4).
Relative Risk of First and Recurrent VTE in Pregnancy on the Background of Genetic Thrombophilia.
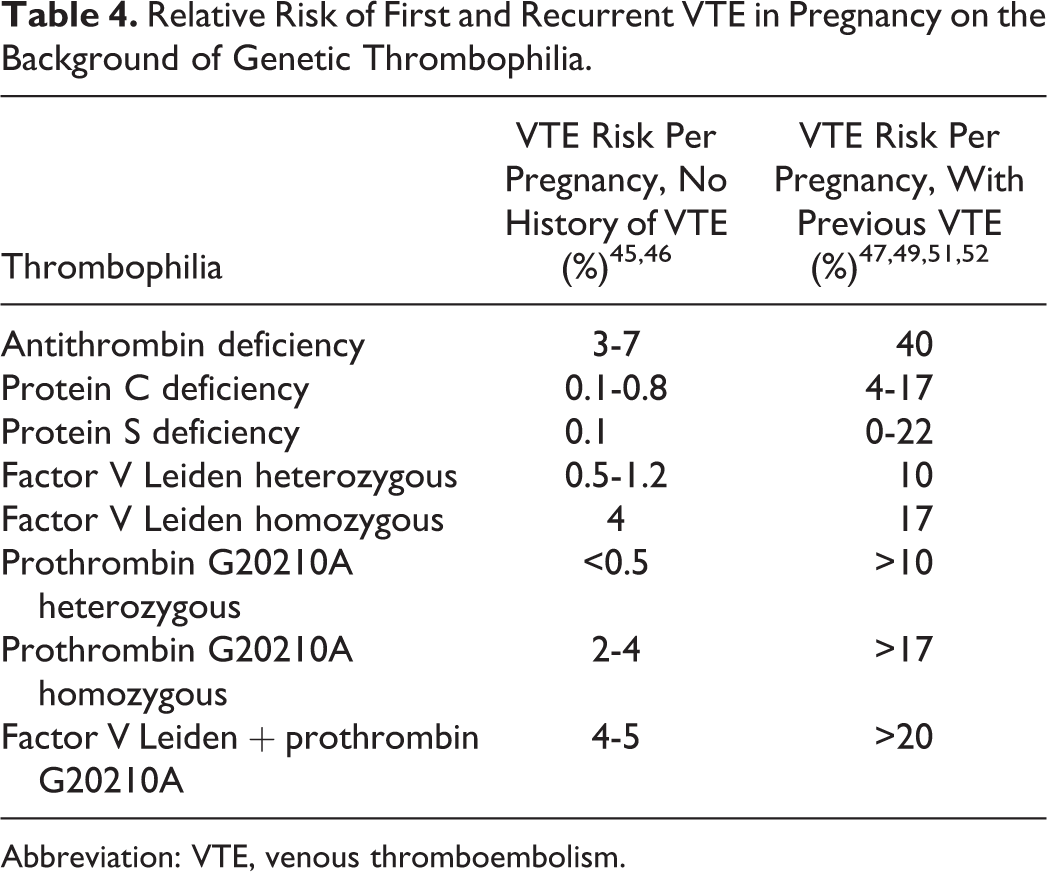
Abbreviation: VTE, venous thromboembolism.
Inherited Thrombophilia and Risk of Obstetric Complications
Complications other than thrombosis in the presence of inherited thrombophilia are pregnancy-induced hypertension, preeclampsia (increased risk of 11-fold in protein S–deficient women), fetal loss (overall risk of stillbirth and miscarriage increased 3.6- and 1.3-fold, respectively), fetal growth retardation (risk increased 5- to 6-fold in prothrombin G20210A mutation and 7-fold in factor V Leiden mutation), and abruptio placentae. 51 –58 Recent prospective cohort studies showed that carriers of factor V Leiden or prothrombin gene mutations are not at significantly increased risk of placenta-mediated pregnancy complications (ie, pregnancy loss, preeclampsia, and/or placental abruption). 59,60 Then the risk of obstetric complications in women with inherited thrombophilia is further influenced by personal characteristics, personal and familial history, circumstantial risk factors, and type of genetic defect. A comprehensive assessment is indicated to estimate the risk of first or recurrent VTE or other complications in pregnancy. With this prerequisite, it appears important to know the thrombophilic defect in women with a previous VTE or a positive familial history.
Thrombophilia Testing in Selected Patients
Thrombophilia screening should be avoided in the acute phase after the thromboembolic event. It should be performed 1 month after the end of the anticoagulation therapy or otherwise 3 months after the VTE, under consideration of the current therapy and the possible interference with the laboratory test results.
Testing selected patients may help to predict the risk of recurrence following completion of anticoagulation therapy, for example, in young patients (<50 years), in member of thrombosis-prone families, and pregnant women. Although no controlled clinical trials have assessed the benefits of testing for thrombophilia on the risk of recurrent VTE, 61 in pregnant women the risk is particularly high (Table 4) and information about the thrombophilic factors may be of clinical utility. Thrombophilia screening for women with pregnancy complication is controversial and The American College of Obstetricians and Gynecologists Women’s health-care physicians recommend against routine thrombophilia testing for such women. 62 Because a causal link between inherited thrombophilia and adverse pregnancy outcome has not been established, 59,60 thrombophilia screening should not be routinely performed for such women; otherwise thrombophilia screening can help women with multiple inexplicable pregnancy losses. For example, in case of 3 or more unexplained consecutive spontaneous miscarriages before the 10th week of gestation, we would recommend to perform a thrombophilia screening, among others for exclusion of the antiphospholipid syndrome. Patients with a recognized and transient clinical risk factor such as surgery (Table 3) with a first VTE have a low risk of recurrence.
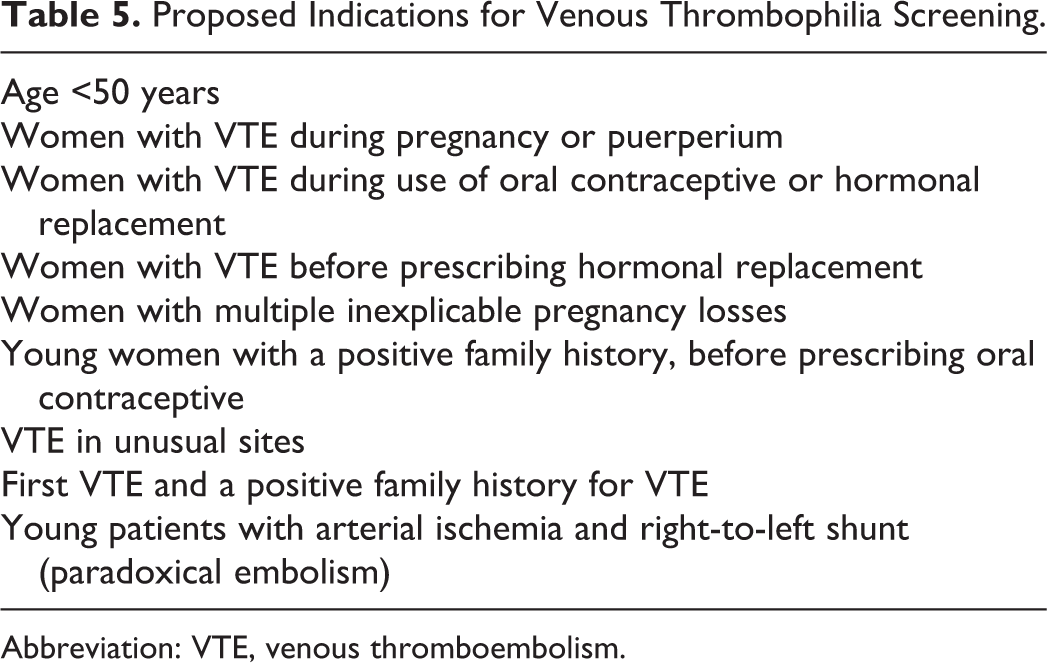
A comprehensive workup including personal and family history and clinical examination is indicated in all patients with VTE. Laboratory test results including hereditary thrombophilia remain helpful in the management of selected patients (Table 5). Because testing for thrombophilia is advantageous if it influences the management of affected patients, we suggest screening in primary young women with VTE during pregnancy, puerperium, oral contraceptives use, hormone replacement therapy, or women with multiple unexplained pregnancy losses. Other indications for thrombophilia screening are thrombosis before 50 years without apparent cause, venous thrombosis in unusual sites, first VTE and a strong family history of VTE. 50,63,64 Identification of asymptomatic family members with hereditary thrombophilia is useful in order to prevent VTE or other complications, especially in young women of childbearing age. These patients may benefit from avoidance of modifiable acquired risk factors (ie, oral contraceptives) and from specific VTE prophylaxis in high-risk situations (ie, pregnancy, puerperium, immobility, trauma, surgery). 65 Testing asymptomatic women randomly before prescribing estrogen medications (oral contraceptives or hormone substitution) is not indicated. 40 Women with a previous VTE and/or positive familial history, though, should be tested. Another indication for venous thrombophilic screening is an arterial ischemia in young patients with right-to-left shunt, such as atrial or ventricular septal defect or arteriovenous malformation (paradoxical embolism).
Proposed Indications for Venous Thrombophilia Screening.
Abbreviation: VTE, venous thromboembolism.
Although diagnosis of genetic thrombophilia is not a criterion anymore to choose the mode and intensity or the length of anticoagulation after a thromboembolic event, knowing whether thrombophilia is present might be useful in assessing the cumulative risk for thrombosis in selected patients. The recent American College of Chest Physicians consensus guidelines 2016 for the treatment of thrombosis stress even more the issue of the personalized risk assessment to determine the length of anticoagulation. 66 There is still no conclusive evidence that thrombophilia testing can prevent thrombotic events in previously unaffected persons. In a cohort study on the prevalence of thrombosis in family members of patients with VTE, only provoked thrombotic events showed a trend for lower prevalence after testing and knowing that thrombophilia is present. In this study, unprovoked thrombosis could not be prevented in the intervention arm. 67 In parallel, various predictive scores for the thrombotic risk have been published, which can be used to assess the clinical risk. These scores do not use genetic thrombophilia as a risk element, but they also have not been prospectively validated in the clinical setting yet. 68,69
Conclusion
In conclusion, our knowledge of VTE etiology has improved over time. Thrombophilia screening is indicated in selected young patients, especially women of childbearing age. The knowledge of the genetic thrombophilic background may help in specific situations to avoid modifiable risk factors and/or introduce prophylactic thromboembolic procedures to decrease the cumulative risk of VTE events. A comprehensive workup including personal and familial history, clinical examination, and laboratory test results including hereditary thrombophilia remains helpful in the management of selected patients. Various national guidelines have discussed indications for thrombophilia testing 70,71 ; a practical one representing the above-mentioned present views is given by the French consensus guideline with Swiss participation. 72
Footnotes
Authors’ Note
All authors have substantially contributed to the conception and design of the article, interpretation of data, drafting of the article, and approved the final version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.