
Abstract
Few data are available on the clinical course of Japanese patients deficient in natural anticoagulants (antithrombin (AT), protein C, and protein S). We conducted a nationwide survey to reveal the clinical course of these patients. Questionnaires were sent to 321 council members of the Japanese Society on Thrombosis and Hemostasis, Japanese Society for Vascular Surgery, and Japanese Society of Phlebology. A total of 103 responses were obtained and data of 183 patients were collected. Of 183 patients, 142 (78%) experienced at least one episode of venous thromboembolism (VTE). The first VTE occurred before the age of 40 years in 71 patients (45%). Venous thromboembolism recurred in 15 (39%) patients with AT deficiency and 19 (18%) patients with other deficiencies. These findings suggest that half of the first episodes of VTE in patients deficient in natural anticoagulants occur before middle age and the risk of VTE recurrence is high in patients with AT deficiency.
Introduction
Patients with inherited thrombophilia, that is, those deficient in natural anticoagulants, such as antithrombin (AT), protein C (PC), or protein S (PS), and polymorphisms of coagulation factors, such as factor V Leiden (FVL) or prothrombin G20210A (PT G20210A), have an increased risk of venous thromboembolism (VTE). Inherited thrombophilia is detected in at least 30% to 40% patients with VTE and is a concern in patients with early-onset thrombotic events, a tendency toward recurrent thrombotic events, a family history of VTE, thrombosis at unusual sites, or idiopathic thrombosis. 1 Although deficiencies in AT, PC, and PS are well-known hereditary risk factors for VTE, they are very rare, presenting in much less than 1% of the general population, 2 and account for 5% to 10% of cases of VTE in Western countries.3,4 On the other hand, in Western countries, FVL and PT G20210A are more frequently found in the general population compared with deficiencies of natural anticoagulants. The estimated prevalence of FVL and PT G20210A is 5% and 2%, respectively, in whites and FVL is present in 12% to 20% of patients with VTE in Western countries.5,6 Several studies have reported the clinical course of subjects with inherited thrombophilia in Western countries,7–11 revealing that deficiencies of natural anticoagulants cause a 5- to 10-fold increase in VTE and the annual incidence of VTE is greater than 1%. On the other hand, FVL and PT G20210A are associated with a lower increase (2- to 5-fold) in VTE and the annual incidence of VTE is less than 0.5%. These data are essential to establish adequate management of patients with inherited thrombophilia. The results of studies in Western countries, however, may not apply to the Japanese because the frequencies of carriers of inherited thrombophilia in the Japanese are quite different from those in whites. For example, the frequency of PS deficiency is as high as 2.04% in the Japanese, 12 whereas the frequency of PS deficiency is less common in whites. 13 Although carriers of FVL or PT G20210A are not rare in whites, they neither has been detected in the Japanese.14–18 Therefore, it is necessary to clarify the clinical course of Japanese patients with inherited thrombophilia, but few data are available. To investigate this issue, we conducted a nationwide survey of Japanese patients deficient in natural anticoagulants.
Materials and Methods
Questionnaires were sent to 321 council members of the Japanese Society on Thrombosis and Hemostasis, Japanese Society for Vascular Surgery, and Japanese Society of Phlebology in April 2009. Physicians who belong to these societies should be specialists of VTE with detailed knowledge of inherited thrombophilia and were assumed to be involved in the management of patients deficient in natural anticoagulants in their institutes. The society members included hematologists, cardiologists, physicians of respiratory medicine, and vascular surgeons. The questionnaire comprised mainly multiple choice questions regarding diagnosis of inherited thrombophilia, family history, oral vitamin K antagonists (VKA) prescription, occurrence of the first episode of VTE, and VTE recurrence. Reply-paid envelopes were used for return of data (Table 1 ). This study was approved by the Institutional Ethical Review Board of Keio University School of Medicine.
Questionnaire Regarding the Status of Japanese Patients Deficient in Natural Anticoagulants (AT, PC, and PS; Originally Written in Japanese)
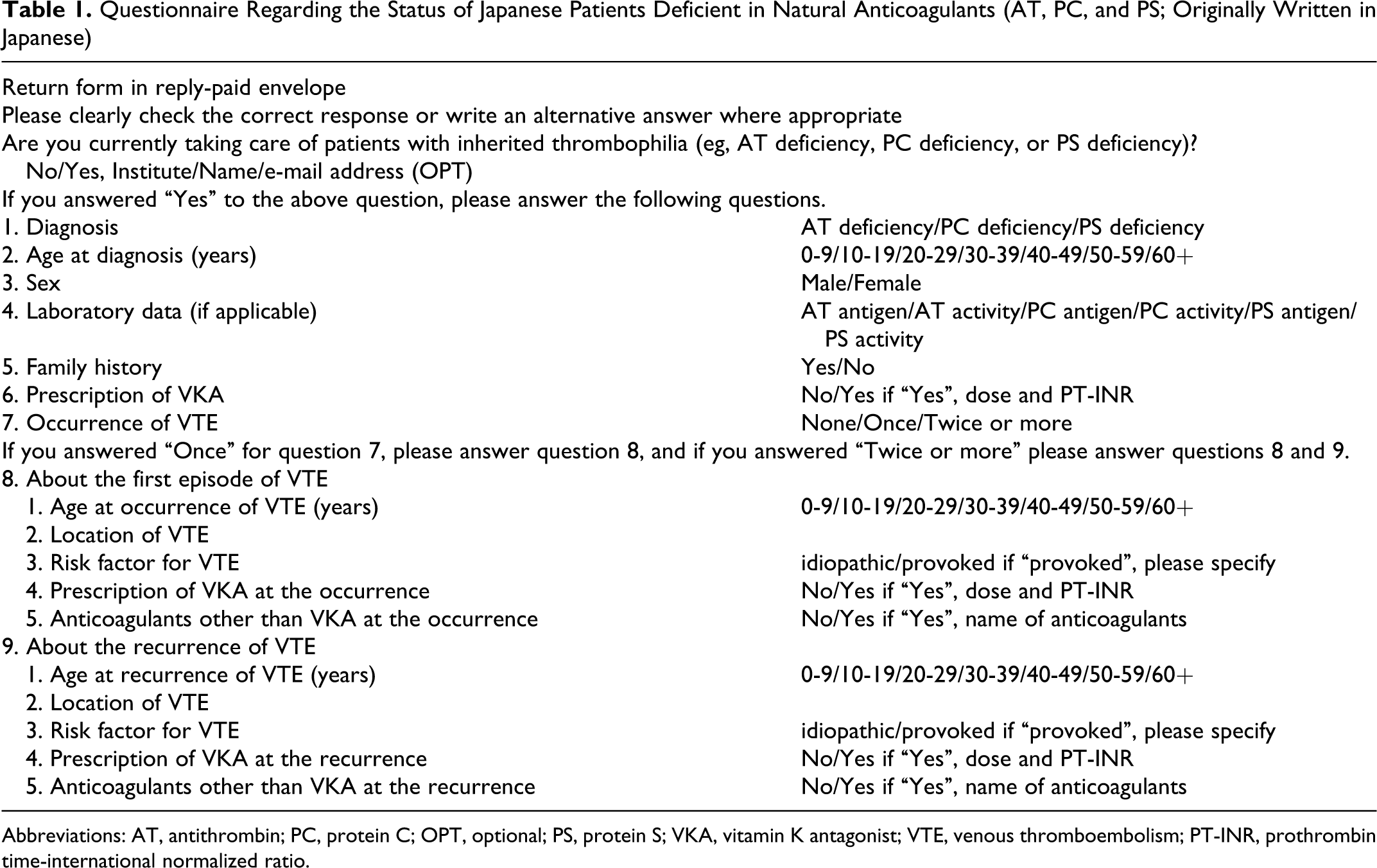
Abbreviations: AT, antithrombin; PC, protein C; OPT, optional; PS, protein S; VKA, vitamin K antagonist; VTE, venous thromboembolism; PT-INR, prothrombin time-international normalized ratio.
Results
Response
Of 321 physicians, 103 (32%) replied to the questionnaires and 33 of them were taking care of patients deficient in natural anticoagulants. Among the 33 physicians, 23 were doing clinical practice in University hospitals, 10 in nonuniversity teaching hospitals, 17 were vascular surgeons, 13 were hematologists, 2 were neurologists, and 1 was a pediatrician.
Patient Characteristics
Detailed information of the clinical course and management was obtained for 183 patients deficient in natural anticoagulants: 50 patients (male to female ratio: 17:33) with AT deficiency, 62 patients (29:33) with PC deficiency, 59 patients (24:35) with PS deficiency, and 12 patients (8:4) with combined deficiencies. Of 17 male patients and 33 female patients, 10 (59%) and 20 (61%) patients, respectively, were diagnosed with AT deficiency before the age of 40 years, whereas 2 (12%) male and 5 (15%) female patients were diagnosed at the age of 60 years or above. Of 29 male patients and 33 female patients, 12 (41%) and 14 (42%), respectively, were diagnosed with PC deficiency before the age of 40 years, whereas 5 (17%) and 7 (21%) patients were diagnosed at the age of 60 years or above. Of 24 male patients and 35 female patients, 11 (46%) and 17 (49%) patients, respectively, were diagnosed with PS deficiency before the age of 40 years, whereas 4 (17%) and 10 (29%) were diagnosed at the age of 60 years or above. Of 8 males and 4 females, 2 (25%) and 1 (25%), respectively, were diagnosed with combined deficiencies before the age of 40 years, whereas 3 (38%) male and 0 (0%) female patients were diagnosed at the age of 60 years or above (Table 2). There were 4 patients with combined AT + PC deficiencies, 3 patients with AT + PS deficiencies, and 5 patients with PC + PS deficiencies.
Activity and Antigen Level of Anticoagulants
The activities of AT or PC were measured in all patients with a diagnosis of AT or PC deficiency. Activity of AT was 48.0% ± 11.4% (n = 50; mean ± standard deviation [SD]) and activity of PC was 43.9% ± 15.0% (n = 62; mean ± SD). Levels of AT antigen were measured in 13 patients with AT deficiency; of them, 10 were diagnosed with AT deficiency type I and 3 were diagnosed with AT deficiency type II. Levels of PC antigen were measured in 32 patients with PC deficiency; of them, 24 were diagnosed with PC deficiency type I and 8 were diagnosed with PC deficiency type II. Activity of PS, measured in 36 of 59 patients with PS deficiency, was 30.5% ± 17.5% (n = 36; mean ± SD). Total PS antigen and/or free PS antigen levels, but not activity of PS, were measured in 23 patients. Both activity and antigen level were measured in 14 patients; 1 was diagnosed with PS deficiency type I and 13 were diagnosed with PS deficiency type II.
Sites of the First VTE Episode
Of 17 male and 33 female patients with AT deficiency, 12 and 26, respectively, had at least one episode of VTE. The first VTE episode was leg deep vein thrombosis (DVT) in 24 (male to female ratio: 6:18), pulmonary embolism (PE) in 4 (2:2), leg DVT + PE in 6 (4:2), and VTE at unusual sites in 4 (0:4; 1 portal vein thrombosis, 2 cerebral venous sinus thrombosis, and 1 leg DVT + cerebral venous sinus thrombosis). Of 29 males and 33 females with PC deficiency, 21 and 25, respectively, had at least one episode of VTE. The first VTE episode was leg DVT in 29 (male to female ratio: 16:13), PE in 6 (2:4), leg DVT + PE in 9 (3:6), and VTE at unusual sites (cerebral venous sinus thrombosis) in 2 (0:2). Of 24 males and 35 females with PS deficiency, 22 and 25, respectively, had at least one episode of VTE. The first VTE episode was leg DVT in 39 (male to female ratio: 18:21), PE in 1 (0:1), leg DVT + PE in 5 (4:1), and VTE at unusual sites in 2 (0:2; 1 leg DVT + mesenteric venous thrombosis and 1 cerebral venous sinus thrombosis). Of 8 males and 4 females with combined deficiencies, 7 and 4, respectively, had at least one episode of VTE. The first VTE episode was in the leg in 6 (male to female ratio: 4:2) and leg DVT + PE in 5 (3:2) (Table 3 ). In total, of the 183 patients deficient in natural anticoagulants, 142 (78%) experienced at least one episode of VTE. Further analysis was performed in these 142 patients.
General Characteristics of the Patients Based on the Responses to the Questionnaire

Age at Occurrence and Predisposing Factors for First VTE Episode
Of the 12 first VTE episodes in male patients with AT deficiency, 8 (66%) occurred before the age of 40 years and 1 (8%) occurred at the age of 60 years or above. Of the 12 VTE episodes, 10 (83%) were idiopathic and the other 2 (17%) were with provoked VTE. Of the 21 first VTE episodes in male patients with PC deficiency, 9 (43%) occurred before the age of 40 years and 4 (19%) occurred at the age of 60 years or above. Of the 21 VTE episodes, 14 (67%) were idiopathic and 7 (33%) were with provoked VTE. Of the 22 first VTE episodes in male patients with PS deficiency, 10 (45%) occurred before the age of 40 years and 4 (18%) occurred at the age of 60 years or above. Of the 22 VTE episodes, 14 (64%) were idiopathic and 8 (36%) were with provoked VTE. Of the 7 first VTE episodes in male patients with combined deficiencies, 3 (43%) occurred before the age of 40 years and 2 (29%) occurred at the age of 60 years or above. Of the 7 VTE episodes, 6 (86%) were idiopathic and 1 (14%) was provoked VTE (Figure 1A ).
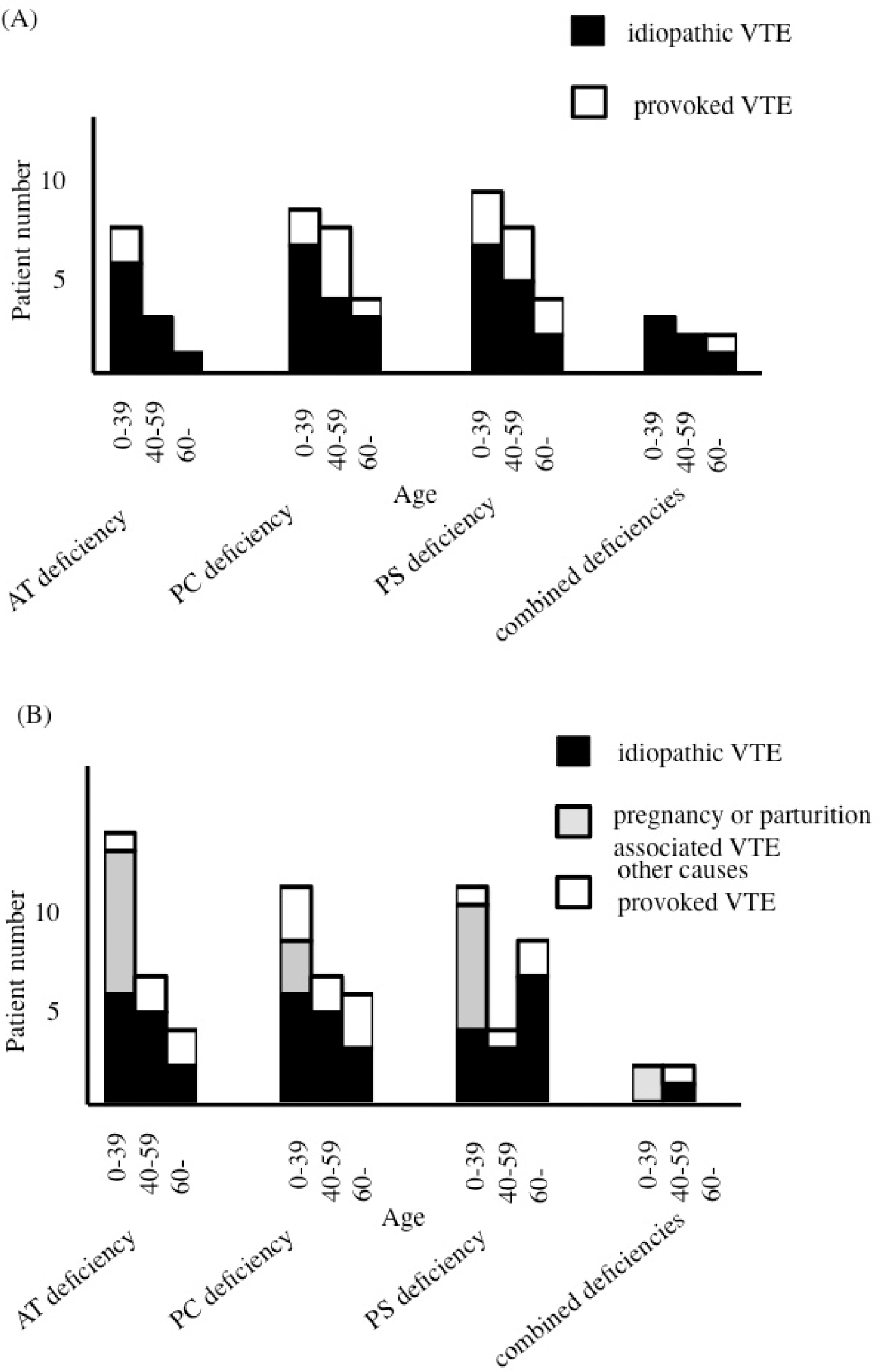
Age at occurrence and predisposing factors of the first episodes of venous thromboembolism (VTE) in male (A) or female (B) patients deficient in natural anticoagulants.
Of the 26 first VTE episodes in female patients with AT deficiency, 15 (58%) occurred before the age of 40 years and 4 (15%) occurred at the age of 60 years or above. Of the 26 VTE episodes, 13 (50%) were idiopathic and 13 (50%) were with provoked VTE. Of the 9 provoked VTE that occurred before the age of 40 years, 8 (89%) were associated with pregnancy or parturition. Of the 25 first VTE episodes in female patients with PC deficiency, 12 (48%) occurred before the age of 40 years and 6 (24%) occurred at the age of 60 years or above. Of the 25 VTE episodes, 14 (56%) were idiopathic and 11 (44%) were provoked VTE. Three of the 6 patients with provoked VTE that occurred before the age of 40 years were associated with pregnancy or parturition. Of the 25 first VTE episodes in female patients with PS deficiency, 12 (48%) occurred before the age of 40 years and 9 (36%) occurred at the age of 60 years or above. Of the 25 VTE episodes, 14 (56%) were idiopathic and 11 (44%) were provoked VTE. Of the 8 provoked VTE occurring before the age of 40 years, 7 (88%) were associated with pregnancy or parturition. Of the 4 first episodes of VTE in female patients with combined deficiencies, 2 (50%) occurred before the age of 40 years and none (0%) occurred at the age of 60 years or above. Of the 4 episodes of VTE, 1 (25%) was idiopathic and 3 (75%) were provoked VTE. Both cases (100%) of provoked VTE that occurred before the age of 40 years were associated with pregnancy or parturition (Figure 1B).
Sites of the First Episodes of VTE in Patients Deficient in Natural Anticoagulants
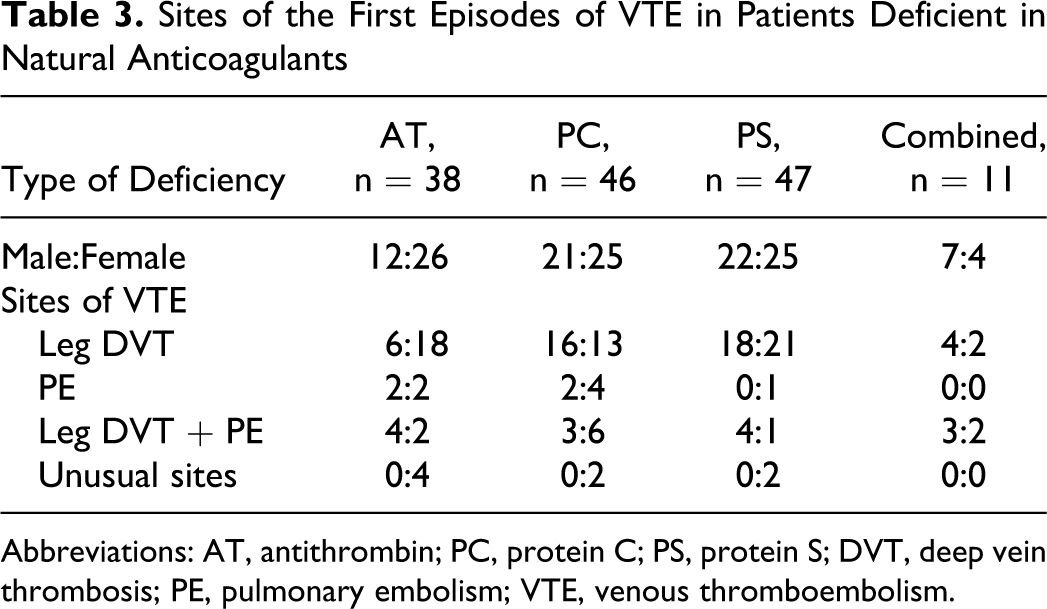
Abbreviations: AT, antithrombin; PC, protein C; PS, protein S; DVT, deep vein thrombosis; PE, pulmonary embolism; VTE, venous thromboembolism.
Prescription of Anticoagulants and VTE Recurrence
In 62 male patients with first episode of VTE, VTE recurred in 3 (38%) of 8 with AT deficiency, 1 (7%) of 14 with PC deficiency, none (0%) of 14 with PS deficiency, and none (0%) of 4 with combined deficiencies who continued anticoagulant therapy after the first episode, while VTE recurred in 4 (100%) of 4 with AT deficiency, 4 (57%) of 7 with PC deficiency, 4 (50%) of 8 with PS deficiency, and 1 (33%) of 3 with combined deficiencies who had stopped anticoagulants (Table 4 ). In 42 female patients with first episode of idiopathic VTE, VTE recurred in 2 (22%) of 9 with AT deficiency, 2 (29%) of 7 with PC deficiency, 1 (10%) of 10 with PS deficiency, and 1 (100%) of 1 with combined deficiencies who continued anticoagulant therapy after the first episode, while VTE recurred in 4 (100%) of 4 with AT deficiency, none (0%) of 7 with PC deficiency, and 1 (25%) of 4 with PS deficiency who had stopped anticoagulants (Table 5 ). In 38 female patients with first episode of provoked, including pregnancy- or parturition-associated VTE, VTE recurred in 1 (13%) of 8 with AT deficiency, 1 (20%) of 5 with PC deficiency, none (0%) of 6 with PS deficiency, and none (0%) of 1 with combined deficiencies who continued anticoagulant therapy after the first episode, while VTE recurred in 1 (20%) of 5 with AT deficiency, none (0%) of 6 with PC deficiency, 2 (40%) of 5 with PS deficiency, and 1 (50%) of 2 with combined deficiencies who had stopped anticoagulants (Table 6 ). All 17 episodes of recurrent VTE in male patients were idiopathic; whereas in the female patients, 9 were idiopathic, 8 were provoked, and 4 were associated with pregnancy or parturition.
Relationship Between Anticoagulant Therapy After First Episode of VTE in Male Patients Deficient in Natural Anticoagulants and Recurrence of VTE
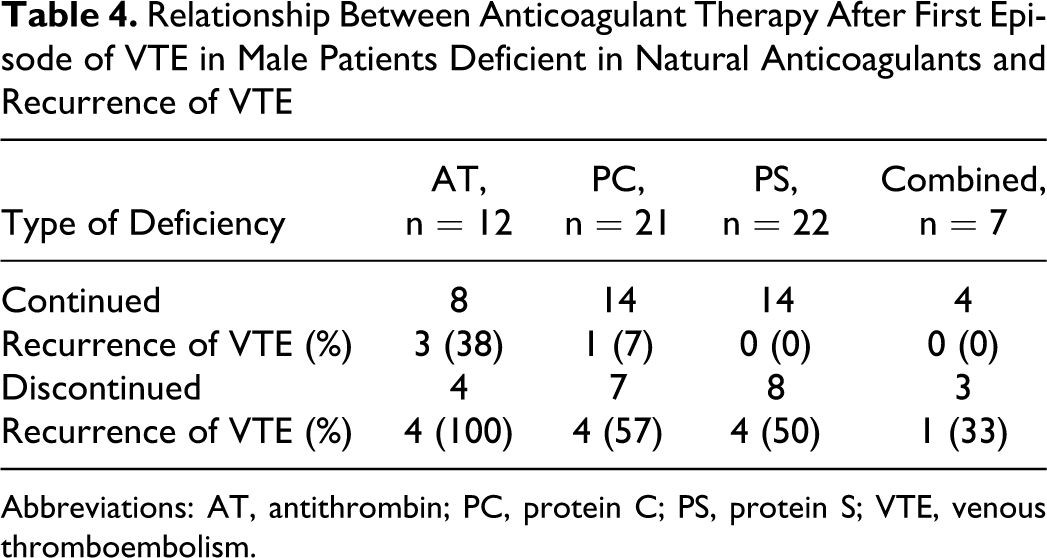
Abbreviations: AT, antithrombin; PC, protein C; PS, protein S; VTE, venous thromboembolism.
Relationship Between Anticoagulant Therapy After First Episode of Idiopathic VTE in Female Patients Deficient in Natural Anticoagulants and Recurrence of VTE
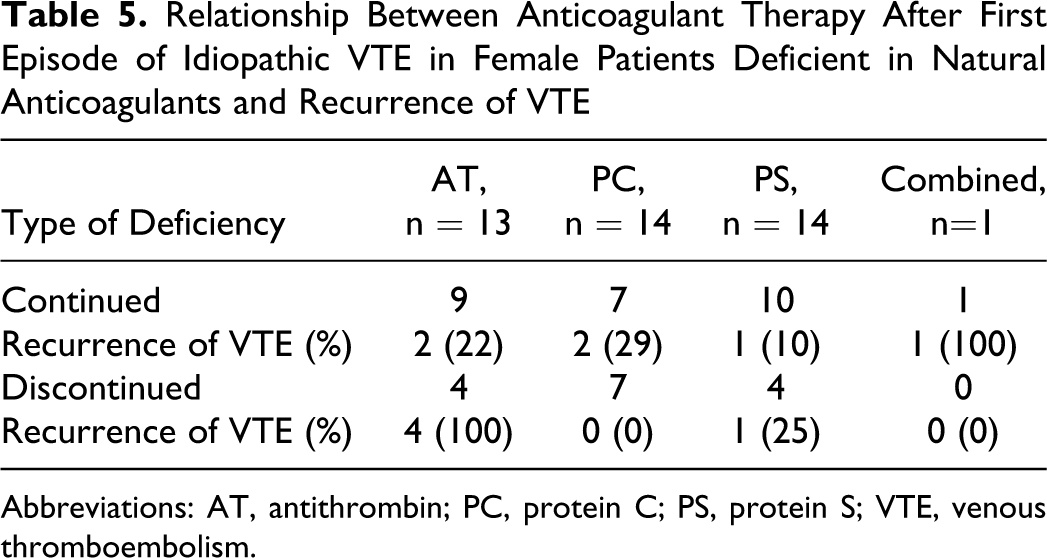
Abbreviations: AT, antithrombin; PC, protein C; PS, protein S; VTE, venous thromboembolism.
Relationship Between Anticoagulant Therapy After First Episode of Provoked VTE in Female Patients Deficient in Natural Anticoagulants and Recurrence of VTE
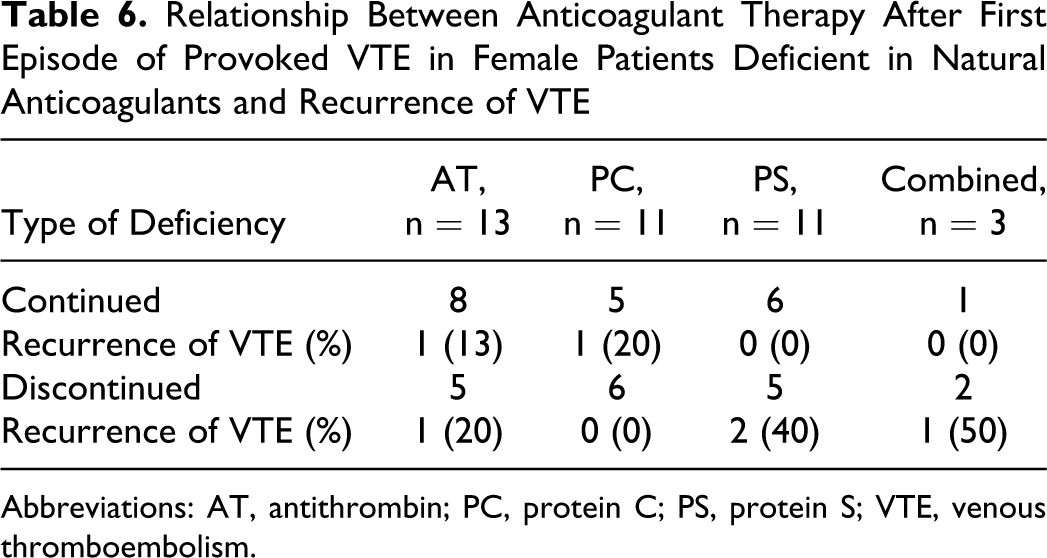
Abbreviations: AT, antithrombin; PC, protein C; PS, protein S; VTE, venous thromboembolism.
Discussion
Several case control studies have reported the incidence of inherited thrombophilia in Japanese patients with VTE. One study demonstrated that 113 Japanese patients are with VTE, 32 (28.3%) had an AT, PC, or PS deficiency, 19 and another study demonstrated that 13 (12%) of 108 patients with AT or PC deficiency had VTE. 20 Of 161 patients with VTE, 15 (9.3%) were carriers of the PS K196E mutation compared with 1.8% of the general population and this mutation is a confirmed genetic risk factor for VTE in the Japanese. 21 These studies demonstrated that deficiencies of natural anticoagulants are more common in Japanese patients with VTE than in whites with VTE, but the clinical course of Japanese patients deficient in natural anticoagulants is not clear. Therefore, we conducted a nationwide survey to elucidate the clinical course of these patients. Detailed information about the clinical course and management of 183 Japanese patients deficient in natural anticoagulants was obtained. Of the patients in our survey, 41 (22%) were diagnosed without previous history of VTE. Antigen and/or activity level of their natural anticoagulants are supposed to be measured because their relatives had been thought to be inherited thrombophilia. Rest of the patients in our survey had had at least one episode of VTE and 60% of the first VTE episodes in patients with AT deficiency occurred before the age of 40 years and approximately 45% of the first episodes of VTE in patients with PC or PS deficiency occurred before the age of 40 years. Approximately 60% of first VTE episodes were idiopathic and some of the first VTE episodes occurred at unusual sites, such as the mesenteric vein and cerebral sinus. Approximately 40% of patients with AT deficiency and 17% of patients with PC or PS deficiency with VTE experienced a recurrence. These findings are comparable with those of a recent prospective study in Europe, demonstrating that 58% of first VTE episodes in thrombophilic individuals were idiopathic and mean age of onset was around the age of 40 years. 9
Women are at increased risk of VTE during pregnancy and the puerperium with an estimated incidence of 0.7 to 1.3 per 1000 pregnant women,22,23 which is approximately 10 times higher than that in nonpregnant women of fertile age. Growing evidence suggests that pregnant women with inherited thrombophilia have a greater risk of VTE than pregnant women without thrombophilia. Administration of prophylactic anticoagulants during pregnancy and postpartum is a common practice for pregnant women with prior VTE and inherited thrombophilia. The management of pregnant women with no prior VTE, but inherited thrombophilia, is controversial, however, because the actual risk of VTE during pregnancy and parturition is uncertain. In a systematic review of 9 studies that estimated the risk of VTE in pregnant women with inherited thrombophilia, deficiencies of natural anticoagulants were associated with a moderately increased risk (AT deficiency: odds ratio [OR] 4.69, PC deficiency: OR 4.76, and PS deficiency: OR 3.19 24 ). A case-control study of 119 women with first VTE episodes during pregnancy or parturition showed that the relative risk of VTE associated with AT, PC, or PS deficiency was increased by as much as 13-fold. 25 In a retrospective study of 72 000 pregnancies, the incidence of VTE was 1 in 113 pregnancies for those with PC deficiency, 1 in 2.8 pregnancies for those with AT deficiency type I, and 1 in 42 pregnancies for those with AT deficiency type II. 26 Considering these results, pregnant women with no prior VTE but AT deficiency should receive prophylactic anticoagulants, while pregnant women with no prior VTE but PC or PS deficiency should be under clinical surveillance or receive prophylactic anticoagulants antepartum and prophylactic anticoagulants postpartum based on the eighth The American College of Chest Physicians (ACCP) guideline. 27 Although the risk of VTE in Japanese pregnant women deficient in natural anticoagulants could not be estimated by our survey, approximately half of the first VTE episodes in female patients occurring before the age of 40 years were associated with pregnancy or parturition. These results suggest that pregnant Japanese as well as white women deficient in natural anticoagulants have an increased risk of VTE, and prophylactic anticoagulants might be beneficial even when the patient has had no prior VTE.
Recurrence of VTE and hemorrhagic complications during anticoagulant therapy are the major problems in the management of patients with VTE. Optimal duration of VKA therapy after the first VTE episode depends on the estimated risk of recurrence and the risk of hemorrhagic complications in patients with prolonged VKA, which is reported to be 1% to 3%.28,29 A recent patient level meta-analysis demonstrated that the 5-year cumulative incidence of recurrent VTE after discontinuation of anticoagulants was 43.1% in men with idiopathic VTE, which was 2.2 times higher than in women with idiopathic VTE, but the risk of recurrence did not differ between men and women with provoked VTE. 30 The relationship between inherited thrombophilia and risk of recurrent VTE was not mentioned in that study. Two recent prospective cohort studies reported a similar risk of recurrence in patients with a first VTE episode regardless of whether they had a thrombophilic defect,31,32 but these two studies included patients with an FVL or PT G20210A mutation as well as patients with AT, PC, or PS deficiency. On the other hand, a recent retrospective analysis involving only patients with AT, PC, or PS deficiency confirmed that relative risk of recurrent VTE was 1.4 for these patients compared with patients without natural anticoagulant deficiencies. The risk of recurrence increased after a first idiopathic VTE as well as with the concomitance of other thrombophilic defects. 33 A total of 34 patients deficient in natural anticoagulants experienced VTE recurrence and 22 episodes occurred after cessation of anticoagulant therapy in our survey. Recurrence of VTE seemed to be more frequent in patients with AT deficiency compared with patients with PC or PS deficiency. Although the optimal duration of anticoagulant therapy after first VTE episode for patients deficient in natural anticoagulants has not been established, based on the previous retrospective analysis and the results of our survey, long-term anticoagulants may be beneficial for male patients deficient in natural anticoagulants after the first VTE episode, and female patients after the first episode of idiopathic VTE, especially in patients with AT deficiency.
Our study has some limitations. All cases with AT or PC deficiency were diagnosed by the measurement of activity of AT or PC. In some cases, antigen levels were also measured to classify the deficiency as type I or type II. Activity of PS was measured in 61% of patients with PS deficiency and other patients with PS deficiency were diagnosed by the measurement of PS antigen only. A higher incidence of VTE in Japanese patients with AT deficiency type I than patients with AT deficiency type II 34 and a high prevalence of PS deficiency type II in the Japanese has been reported. 12 These previous reports led us to measure both antigen levels and activities of AT, PC, and PS in Japanese patients with suspected natural anticoagulant deficiencies, but our questionnaires revealed that all of them were measured in only a limited number of patients. All Japanese are basically covered by national health insurance. The measurement of activities of AT and PC and PS antigen is covered by insurance, but the measurement of activity of PS was not covered at the time of survey. This restriction made it difficult to measure both activities and antigen levels of anticoagulants in all patients with suspected natural anticoagulant deficiencies in clinical practice. We did not ask the cutoff value of the levels of natural anticoagulants in each institute and the variation of cutoff value might exist among institutes; however, the results of our survey suggested that cutoff value was 65% to 70% for the activity of AT and 60% to 65% for the activity of PC. Cutoff value for the activity of PS and PS antigen seemed to be 50% to 55% and 55% to 60%, respectively, except for pregnant women. We asked family history and genetic diagnosis in the questionnaires; however, genetic analysis of natural anticoagulants is not covered by the health insurance and response to the questionnaires about relatives or genetic diagnosis of patients' might conflict with the privacy policy at some institutes. In addition, some patients were only recently diagnosed and attending physicians might have sufficient information about the patients' relatives, while others were diagnosed years ago and information about the patients' relatives might be uncertain because of changes in attending physicians. These limitations could result in insufficient information of family history or genetic diagnosis of patients. Patients with PS K196E might be included in patients with PS deficiency in our survey and it is interesting to compare the clinical course of these patients to those of other patients deficient in natural anticoagulants; however, we could not do it because of above reason. Furthermore, it cannot be completely denied that patients with secondary deficiency in natural anticoagulants might be included in our survey. Finally, most patients in our survey visited their physicians regularly. Because patients without medication or patients with no prior VTE might not continue to visit their physicians, most individuals deficient in natural anticoagulants and with no prior VTE could be excluded from this study. These might result in a high frequency of first or recurrent episodes of VTE and a high VKA prescription rate in patients with prior VTE.
In conclusion, our survey revealed useful information regarding the occurrence of VTE in Japanese patients deficient in natural anticoagulants and the clinical management of these patients. Most of the patients in our survey were followed-up by a vascular surgeon or hematologist. Societies of these specialists should collaborate to create a central registry for Japanese patients with deficiency in natural anticoagulants to determine the actual incidence of VTE in these patients and to establish guidelines for adequate management of these patients to prevent a first or recurrent VTE.
Footnotes
Appendix
Name and institute of the physicians who provided the information of patients deficient in natural anticoagulants are as follow (INPO): H Shikata (Kanazawa Medical University); M Yamazaki (Tokyo Women’s Medical University); U Yatomi (Tokyo University); M Ieko (Hokkaido University); E Morishita (Kanazawa University); H Satokawa (Fukushima Medical University); K Okamoto and M Sakai (University of Occupational and Environmental Health, Japan); H Komai (Tokyo Medical University); M Uchiba (Kumamoto University); K Ijima (Tottori University); O Sato (Saitama Medical Center); T Koyama (Tokyo Medical Dental University); N Yamamoto (Hamamatsu Medical University); T Okamura (Kurume University); H Wada (Mie University); S Madoiwa (Jichi Medical University); K Ota, H Ishibashi, and T Yamada (Aichi Medical University); N Shirasugi (Aiseikai Aisei Hospital); M Yoshida (Hyogo Brain and Heart Center); N Morimoto (Jikeikai Kitami Central Hospital); S Sugiyama (Hiroshima Teishin Hospital); Y Shigekiyo (Tokushima Prefectural Hospital); N Nishikimi (Japanese Red Cross Nagoya Daiichi Hospital); K Niimi (KKR Tokai Hospital); K Naito (Hamamatsu Medical Center); S Matsumoto (National Hospital Organization Tokyo Medical Center); M Yasaka (National Hospital Organization Kyushu Medical Center); T Kawasaki (Osaka University); T Kojima (Nagoya University); K Yokoyama (Keio University).
Acknowledgments
The authors thank the Japanese Society on Thrombosis and Hemostasis, Japanese Society for Vascular Surgery, and Japanese Society of Phlebology for kindly providing the mailing list of council members. The authors also thank the assistance of Ms Yukari Tomita in mailing questionnaires.
Authors’ Note
This manuscript was presented at The 72nd Annual Meeting of the Japanese Society of Hematology, Kanagawa, Japan, September 24-26, 2010.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: supported in part by Grant-in-Aid for Blood Coagulation Abnormalities from Ministry Health, Labor and Welfare of Japan.