
Abstract
The role of thrombophilia in the pathogenesis of stroke is still controversial, especially in the pediatric stroke. In order to examine the role of common thrombophilic mutations in children and adults with stroke, a case–control study was carried out in a group of 80 children and 73 younger adult patients. The control groups encompassed 100 healthy children and 120 healthy blood donors. Our results showed no significant differences in the frequency of factor V (FV) Leiden, FII G20210A, and methylenetetrahydrofolate reductase (MTHFR) C677T variants between patient groups and corresponding controls. According to our results, carriers of 677CT genotype have 3.62 higher risks to develop stroke in children than in adults (P < .001). The obtained data indicate that heterozygosity for MTHFR C677T variant represents a possible important risk factor for pediatric stroke and suggest a different role of this gene variant in etiology of stroke in pediatric and adult patients.
Introduction
Stroke in childhood is less common than in adults (the average annual incidence rate exceeds 8/100 000) but is a very important cause of lifelong morbidity. It is a multifactorial disease in which both acquired and genetic influences may play important role.1,2 Many of well-characterized risk factors for stroke in adults, such as atherosclerosis, hypertension, or smoking, are far less presented in pediatric stroke.2,3 Since that genetic basis of stroke in children is supposed to be more pronounced than in adults. 3
According to published data, prothrombotic genetic risk factors could be involved in pathophysiology of adult stroke, but they are still not well characterized in pediatric patients. The factor V G1691A (FV Leiden) mutation is the most common prothrombotic risk factor, resulting in an increase in thrombin generation. 4 The second most common genetic risk factor is G>A at position 20210 of the FII gene that is associated with increased level of prothrombin and enhanced blood coagulation. 4 Although these 2 gene variants represent a significant risk factor for prothrombotic disorders, their role in the pathogenesis of stroke is not clearly defined, especially in pediatric patients.5 –7 The most frequent inherited cause of hyperhomocysteinemia is C677T variant of methylenetetrahydrofolate reductase (MTHFR). 8 Homozygosity for MTHFR C677T is proposed as a genetic risk factor for stroke in adults, but reports concerning a role of MTHFR C677T variant in pediatric stroke gave conflicting results.9 –12
The aim of our study was to examine the role of FV Leiden, FII G20210A, and MTHFR C677T gene variants as risk factors in pathogenesis of stroke in children, as well as, to analyze possible different influence of genetic basis in the etiology of pediatric and adult stroke.
Design of Study
Patients
In this study, 80 children (34 females and 46 males, age 6.7 ± 4.9 years) and 73 younger adult patients (32 females and 41 males, age 40.3 ± 11.6 years) having cerebral infarcts were included. After objectively diagnosed stroke, patients were referred for genetic testing to the Institute of Molecular Genetics and Genetic Engineering. The diagnosis was established based on clinical and radiological criteria using magnetic resonance imaging and magnetic resonance or digital subtraction angiography. The control groups encompassed 100 (54 females and 46 males, age 9.5 ± 0.5 years) healthy children from general population and 120 healthy blood donors (36 females and 84 males, age 38.5 ± 13.1 years). Individuals included in our study were from the same geographic area and with the same ethnic background. The study protocol was approved by local research ethics committee, and informed consent was obtained from participants and parents of all participating children.
Methods
DNA was extracted from peripheral whole blood using GFX Genomic Blood DNA Purification kit (GE Healthcare, Little Chalfont, UK). The FV Leiden, FII G20210A, and MTHFR C677T mutations were detected by polymerase chain reaction followed by digestion with specific restriction enzymes as described previously. 13
Statistical Analysis
Age is expressed as mean ± standard deviation. Deviations of genotypes distributions from Hardy-Weinberg equilibrium were assessed by χ 2 test. Fisher exact test was used to compare frequencies of allelic and genotype distributions between patients and control individuals. P values <.05 were considered statistically significant. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were also calculated. All statistical analyses were performed using SPSS 10.0 and SAS Power 9.2 and Sample Size 3.1 statistical software.
Results
The genotype distributions were in Hardy-Weinberg equilibrium, with the exception of the MTHFR C677T including both groups of patients. Observed genotype distributions of C677T variant were significantly different than it would be expected. In children group, there was excess of heterozygotes (χ 2 = 8.02, degrees of freedom [df] = 1, P < .005), while in adult patients, there was excess of homozygotes (χ 2 = 4.98, df = 1, P < .05). When genotype frequencies were compared among patients and control groups, no significant differences were observed for FV Leiden, FII G20210A, and MTHFR C677T (Table 1 ).
The Distribution of FV, FII, and MTHFR Genotypes Among Children and Adults With Stroke and Controls
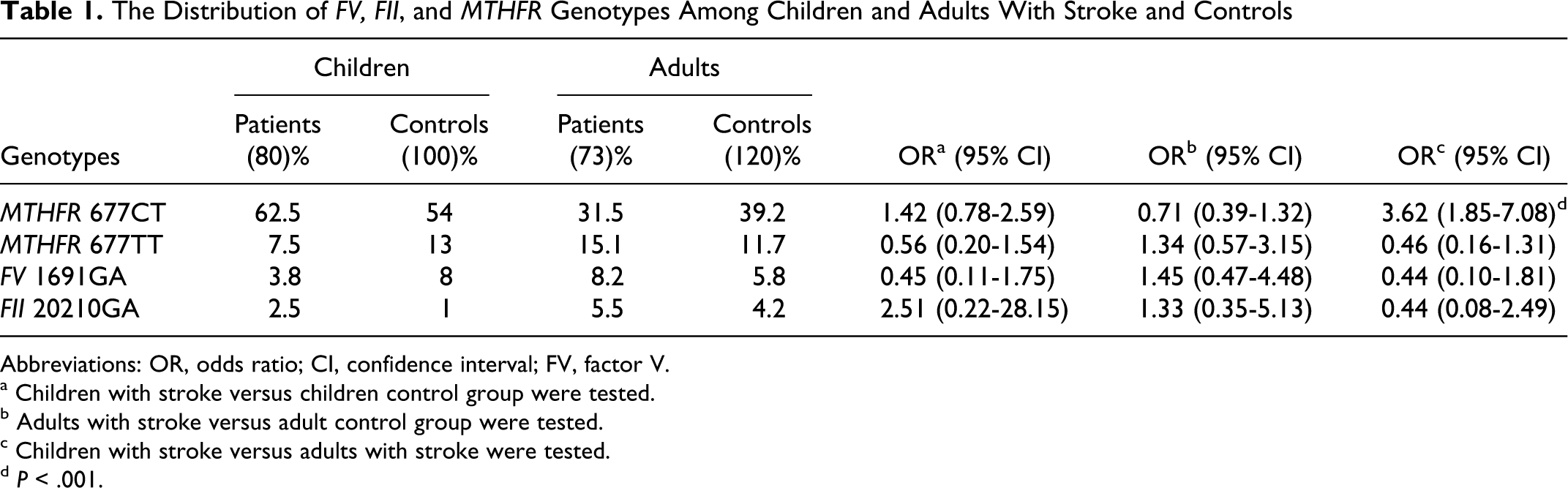
Abbreviations: OR, odds ratio; CI, confidence interval; FV, factor V.
a Children with stroke versus children control group were tested.
b Adults with stroke versus adult control group were tested.
c Children with stroke versus adults with stroke were tested.
d P < .001.
Statistical significance was observed when group of pediatric stroke was compared with adult patients. The frequency of heterozygotes for C677T variant was significantly (P < .001) higher in children with stroke (62.5%) than in adult patients (31.5%; Table 1). According to our results, carriers of MTHFR 677CT genotype have higher risk to develop stroke in children than in adults (OR = 3.62).
Discussion
The etiology of stroke comprises genetic and acquired risk factors. The genetic risk factors involved in development of stroke are multiple and still not well characterized. Since the prevalence of genetic factors might be more pronounced in younger patients, in comparison to older ones, pediatric patients and younger adults with stroke were analyzed in this study.
We compared the distributions of FV Leiden, FII G20210A, and MTHFR C677T gene variants in 2 groups of stroke patients, children and younger adults, with 2 appropriate control groups. The main limitation of our study is a relatively small sample size resulting in low power (<0.25) to detect genotype–disease association. Most of studies regarding the role of genetic factors in childhood stroke are performed on small sample size since the disease is relatively rare.6,14 As we did not have the possibility to enlarge the group of pediatric patients, we opted for the group of adult patients of similar size. Small-scale single-centered studies might provide basic information for large-scale studies regarding proper study design, sample size, and relevant clinical information. However, we performed post hoc power analysis since it can be useful for planning future studies or meta-analysis. 15
So far, studies that investigated the role of FV Leiden and FII G20210A mutations in pathogenesis of stroke reported conflicting results for adult patients.16,17 Majority of these studies did not reach statistical significance, and published meta-analyses are unconvincing due to the inclusion of suboptimal data. 17 The results of our study showed that FV Leiden and FII G20210A genetic variants do not represent statistically significant risk factors for the development of adult stroke (OR 1.45 and OR 1.33, respectively). The role of FV Leiden and FII G20210A mutations in the etiology of pediatric stroke has been extensively studied but with controversial findings. While several studies revealed these variants as significant risk factors,18,19 other investigations found no association with stroke in children.6,14 According to our results, distribution of FV Leiden genotype was lower in children with stroke than in controls (3.8% vs 8.0%). On the other hand, the FII G20210A heterozygotes were overrepresented in a group of pediatric patients than in controls (2.5% vs 1.0%), but the difference was not statistically significant.
A common polymorphism, C677T, of the MTHFR gene, was analyzed in a large number of studies investigating adult and pediatric stroke, but the obtained data were inconsistent.6,17,20 Studies were mainly focused on the role of homozygosity for T allele in the development of this disease, while the possibility that heterozygosity might represent risk factor has gone unrecognized. In our study, the frequency of MTHFR 677TT genotype was higher in adult patients in comparison to control group (15.1% vs 11.7%), but statistical significance was not observed. Due to the low statistical power, this conclusion may lead to type II error. In future studies, larger cohorts should be used to ascertain this observation. However, the distribution of MTHFR gene variant, in adult patient group, was not in Hardy-Weinberg equilibrium (χ 2 = 4.98, df = 1, P < .05). Considering the frequency of 677T allele (30.8%), <15.1% carriers of homozygote genotype should be expected. The reason for this might be due to sampling variation or small sample size but also might implicate importance of MTHFR homozygote genotype in the pathology of stroke in adults. On the other hand, in pediatric patients, the frequency of MTHFR 677CT genotype was higher in comparison to control group (62.5% vs 54.0%), but significance also was not achieved. The distribution of 677TT genotype was almost twice lower in the group of children with stroke in comparison to controls (7.5% vs 13.0%), that is opposed to results obtained for adult patients. Also, in group of children with stroke, the frequency of MTHFR variant was not in Hardy-Weinberg equilibrium. In this group, heterozygote genotype was more frequent than it would be expected according to frequency of T allele (38.8%). These results may implicate importance of MTHFR C677T heterozygote genotype in children, and homozygote in adults, in etiology of stroke.
In this study, different distribution of MTHFR C677T genotypes was revealed among children and adult controls. Two control groups were employed, for comparison with adult and children patients groups, representing age-matched controls, in order to avoid possible influence of age difference on the results. The observed differences in genotype distribution between control groups in our study might be explained by influence of environmental factors, aging and lifestyle. Accordingly, this difference could reflect age-related association of MTHFR C677T polymorphism in healthy individuals. Different distribution of MTHFR C677T genotypes between adult and pediatric controls characterize several European populations, thus supporting the trend observed in our study.21 –26
In order to analyze the possible different role of genetic factors in children and adult stroke patients, we have also compared the distribution of analyzed genotypes between children and adult patient groups. Both FV Leiden and FII G20210A mutations were less frequent in pediatric patients in comparison to adults, but these differences were not statistically significant. We observed statistically significant difference in the distribution of MTHFR CT individuals between the pediatric and adult patient groups (P < .001). According to our results, carriers of CT genotype have more than 3 times higher risk (OR = 3.62) to develop stroke in childhood than in adults. Heterozygosity for MTHFR C677T variant is very common in general populations, associated with slight elevation of homocysteine level, and therefore not considered as an important risk factor so far. Nevertheless, in the study of Bethke et al, heterozygosity variants of MTHFR gene (C677T and A1298C) were associated with the highest risk of meningioma. 27 Increased frequency of MTHFR 677CT genotype was also observed in pediatric patients with acute lymphoblastic leukemia and venous thrombosis.28,29 In our previous study, MTHFR CT heterozygote in combination with eNOS 894TT genotype was associated with arterial ischemic stroke in children. 30 Although the accurate mechanism by which CT genotype may influence stroke occurrence is not defined, it is possible that its different expression in children and adults might be involved in the pathology of stroke.
In conclusion, this is the first study in which the most common prothrombotic genetic risk factors were compared in pediatric and adult patients with stroke. These results point out the possible role of MTHFR 677CT genotype in the etiology of stroke in childhood. Although hampered by a small sample size, our study suggests a possible different role of this polymorphism in pediatric and adult patients. Further analysis in a larger cohort of individuals is needed to confirm our results, which might influence progress in diagnosis and prevention of this disease.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: supported from Ministry of Education and Science, Republic of Serbia [grant number 173008].