
Abstract
The aim of this study was to investigate the prognostic role of mean platelet volume (MPV) in patients with coronary artery ectasia (CAE). The baseline MPV values of 258 patients with CAE were screened. The mean time of follow-up was 49 ± 21 months for major adverse cardiac events (MACEs) defined as the combination of cardiac death, nonfatal myocardial infarction (MI), rehospitalization due to cardiac disorders, and readmission due to chest pain. During follow-up period, 63 (24%) MACEs developed. There were 4 (2%) cardiovascular deaths, 0 nonfatal MI, 14 (5%) rehospitalization, and 45 (17%) readmission. Mean platelet volume values were significantly higher in patients with CAE with MACEs than in patients with CAE without MACEs (9.5 ± 1.2 fL vs 8.9 ± 1.1 fL, respectively, P = .002). The rate of MACE was higher in CAE patients with MPV of >9 fL than those with MVP of ≤9 fL (33% vs. 15%, P = .001). Mean platelet volume has a prognostic value for MACEs in patients with CAE.
Introduction
Coronary artery ectasia (CAE) has been defined as the localized or diffused nonobstructive lesion of the epicardial coronary arteries with a luminal dilation exceeding the 1.5-fold of normal adjacent arterial segment. 1 Incidence of CAE has been reported to range between 1% and 4% in patients undergoing coronary angiography. 2–4 Coronary artery ectasia has been attributed to the condition such as atherosclerosis, inflammatory disease, connective tissue disease, or a congenital disease. 1–3
Mean platelet volume (MPV) is an indicator of platelet activation, which has an important role in the pathophysiology of cardiovascular diseases. 5,6 It has been shown that larger platelets have higher thrombotic potential. 7 Larger platelets have more granules, aggregate more rapidly with collagen, have higher thromboxane A2 level, and express more glycoprotein Ib and IIb/IIIa receptors. 8–10 Elevation of MPV values has been shown in atherosclerotic heart diseases and primarily acute myocardial infarction (AMI). 11,12 Mean platelet volume has been shown to be elevated in patients with CAE. 13–15
Some authors have postulated that CAE may cause myocardial ischemia/infarction without significant coronary artery stenosis due to intracoronary thrombosis within the ectasic segment and distal embolization of this thrombotic material. 16,17 We suggested that patients with CAE with high MPV may have higher risk of myocardial ischemia/infarction. So, we aimed to investigate the prognostic value of MPV in patients with CAE.
Material and Methods
The study group consisted of 258 consecutive patients (127 females, 131 males; mean age 54.1 ± 10.4 years) with CAE who were admitted to our center. The baseline MPV values of 258 patients with CAE were screened. Coronary artery ectasia group consisted of isolated CAE who had no other stenotic lesions under visual assessment. The indication for coronary angiography was either the presence of typical angina or positive or equivocal results of noninvasive screening tests for myocardial ischemia in both the groups. Hypertension was considered to be present if the systolic pressure was >140 mm Hg and/or diastolic pressure was >90 mm Hg or if the individual was taking antihypertensive medications. Family history of coronary heart disease (CHD) was diagnosed if patients had a first-degree male relative <55 years of age or a female relative <65 years of age with CHD. Patients who were smoking before hospitalization were accepted as smokers. Exclusion criteria were prior myocardial infarction (MI), valvular heart disease, heart failure, peripheral vascular disease, renal and hepatic dysfunction, hematological disorders, history of malignancy, acute or chronic infection, and stroke. The patients who had coronary stenotic lesions of >20% were also excluded from the study. All patients and control individuals gave informed consent and the study was approved by the local ethics committee.
Coronary Angiography
Coronary angiography was routinely performed without the use of nitroglycerin. Selective coronary angiography was performed by means of the Judkins technique in multiple projections. We used iohexol (Omnipaque) as contrast agent during coronary angiography in all patients and control individuals. Coronary angiograms were analyzed by 2 blinded interventional cardiologists without the knowledge of the clinical status and laboratory measurements of the individuals. Coronary artery ectasia was defined as the segmental or diffuse dilation of the coronary arteries to >1.5-fold the diameter of the adjacent segments of the same artery or of different arteries as defined by Falsetti and Carroll. 18 We used this definition for terminology. A normal segment was defined as a coronary artery segment without ectasia or stenosis on the basis of coronary angiography. When there was no identifiable adjacent normal segment, the mean diameter of the corresponding coronary segment in the control group served as normal values.
Biochemical Measurements
Blood samples were drawn after a fasting period of 12 hours. Glucose, creatinine, and lipid profile were determined by standard methods. Mean platelet volume was measured in a blood sample collected in dipotassium EDTA tubes (Vacuette, Greiner, UK) in less than 2 hours to prevent EDTA-induced swelling. An automatic blood counter (Beckman-Coulter Co, Miami, FL, USA) was used for whole blood counts.
Follow-up
Follow-up was performed by telephone interview for all the patients. Researcher performing follow-up interviews were blind for MPV status of the patients. For those patients who have reached at least one of the primary end points, recorded data and medical reports were evaluated to determine including criteria. The primary end point of the study was major adverse cardiac events (MACEs), which were defined as the combination of cardiac death, nonfatal MI, rehospitalization due to cardiac causes like chest pain, hypertension, and readmission due to chest pain. If a patient had been readmitted to hospital or rehospitalized for possible cardiac symptoms, the records from the admitting hospital were obtained. For patients with >1 MACEs, only the first event was counted as an end point.
Statistical Analysis
Data were analyzed with the SPSS (Chicago, Illinois) software version 10.0 for Windows. Continuous variables from the study groups were reported as mean ± standard deviation and categorical variables as percentages. To compare continuous variables, the Student t test or Mann-Whitney U test was used where appropriate. Categorical variables were compared with the chi-square test. Normal limits of MPV were 7.2 to 10.8 fL in our laboratory. Since the number of patients with increased MPV (>10.8 fL) was limited to only 20 patients, we calculated the cut-point for MPV to identify the presence of cardiac events using receiver–operating curve analysis. The cut-point of 9 fL was found to be an identifier value for patients with cardiac events with a sensitivity of 67% and a specificity of 57% (area under curve = 0.64, P = .001). According to the categorized MPV values (≤9 vs >9 fL), event-free survival was evaluated by Kaplan-Meier curves. A P < .05 was considered significant.
Results
During the study period, 366 patients had diagnosis of CAE. We could access all 258 patients (127 females, 131 males; mean age 54.1 ± 10.4 years) by telephone interview. The mean time of follow-up was 49 ± 21 (1-78) months. During this follow-up period, 63 (24%) MACEs occurred in allover patients with CAE. There were 4 (2%) cardiovascular deaths, 0 nonfatal MI, 14 (5%) rehospitalization, and 45 (17%) readmission. There was no nonfatal MI in all patients with CAE during follow-up period.
Baseline clinical and laboratory characteristics of patients with MACEs and without MACEs are shown in Table 1 . There were no statistically significant differences between the 2 groups with respect to gender, body mass index, presence of hypertension, smoking, family history, and levels of glucose, creatinine, total cholesterol, triglyceride, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, hemoglobin, and platelet count. The mean age of patients with CAE with MACEs was higher than that of patients with CAE without MACEs (58.7 ± 10.7 vs 52.3 ± 9.7; P < .001). Mean platelet volume values were significantly higher in patients with CAE with MACEs than in patients with CAE without MACEs (9.5 ± 1.2 fL vs 8.9 ± 1.1 fL, respectively, P = .002). Table 2 shows the comparison of the patients with CAE with MPV ≤9 fL and MPV >9 fL. Platelet count was significantly higher in patients with CAE with MPV ≤9 fL than in patients with CAE with MPV >9 fL (253.1 ± 79.4 vs 226.4 ± 63.7, respectively, P = .003). The rate of MACEs was higher in patients with CAE with MPV >9 fL than those with MVP ≤9 fL (33% vs 15%, P = .001). In this study, MPV is related only with readmission. There were no significant differences between these 2 groups with respect to clinical and other laboratory characteristics. In Figure 1 , Kaplan-Meier curves demonstrate survival rate in patients with CAE according to categorized MPV values. Based on Kaplan-Meier curves (Figure 1), event-free survival was much better in patients with CAE with MPV ≤9 fL than those with MPV >9 fL (86% vs 67%, P = .001).
Baseline Clinical and Laboratory Characteristics of Patients With MACEs and Without MACE a
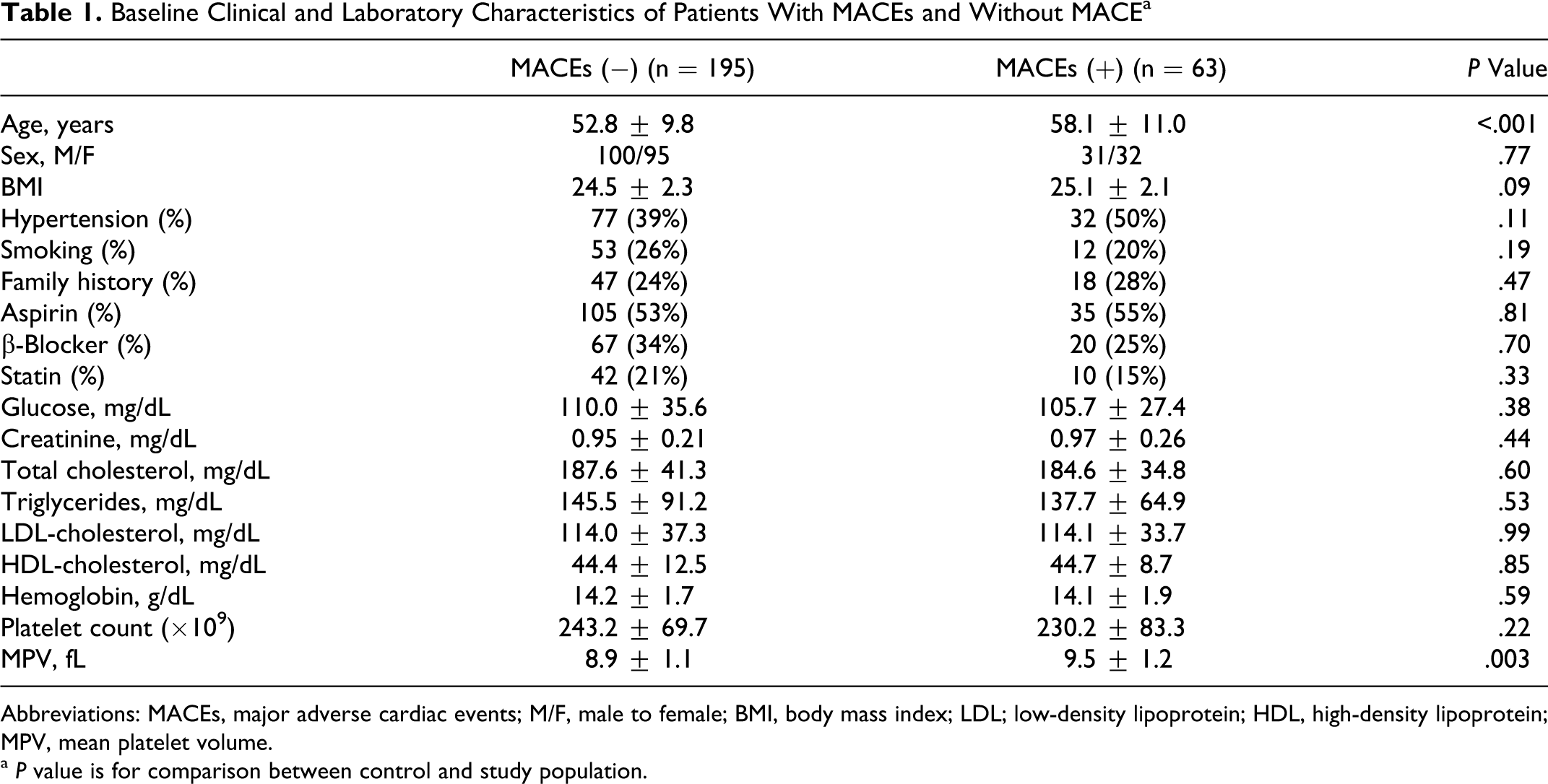
Abbreviations: MACEs, major adverse cardiac events; M/F, male to female; BMI, body mass index; LDL; low-density lipoprotein; HDL, high-density lipoprotein; MPV, mean platelet volume.
a P value is for comparison between control and study population.
Comparison of the Clinical and Laboratory Characteristics of the Patients With MPV ≤9 fL and MPV >9 fL a
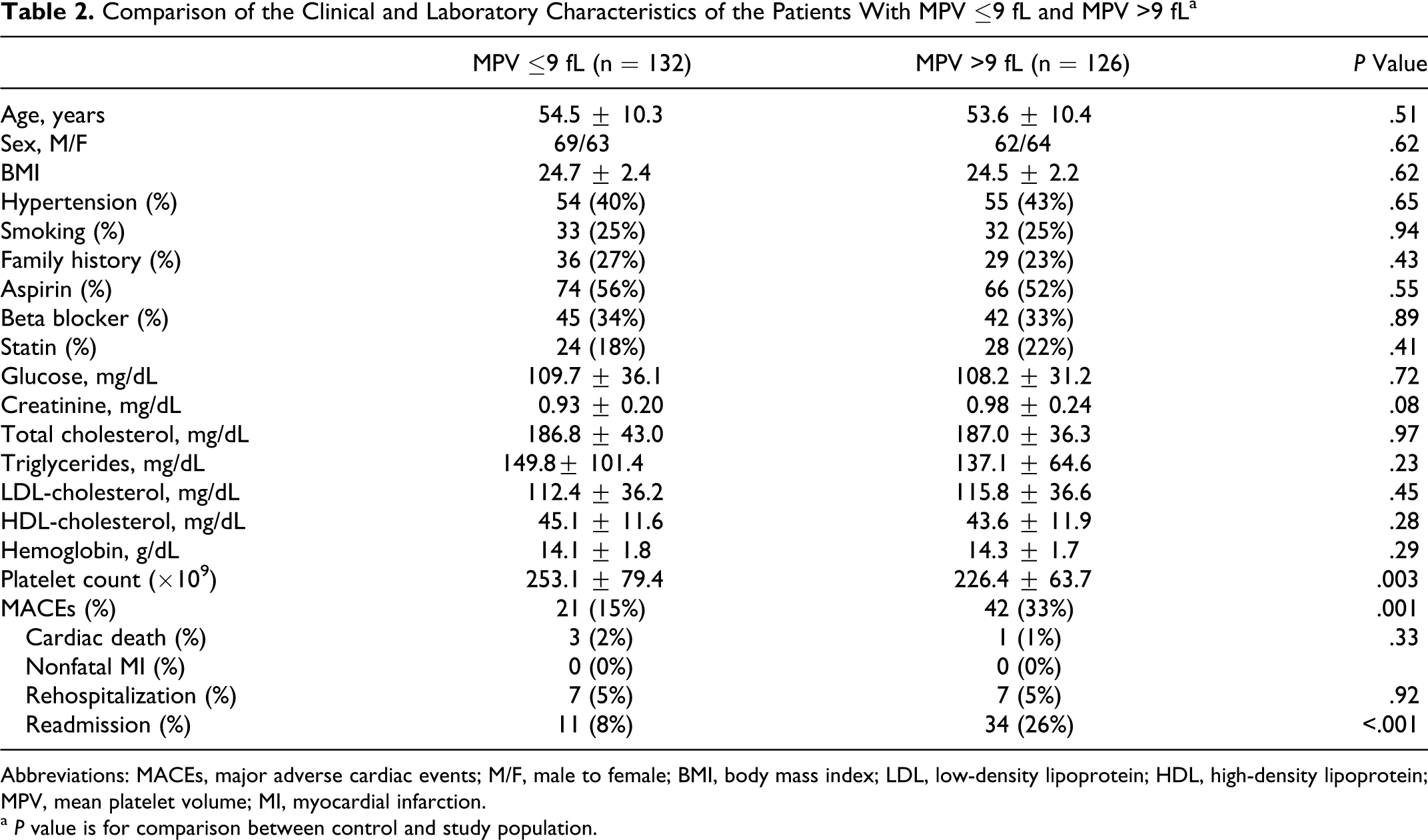
Abbreviations: MACEs, major adverse cardiac events; M/F, male to female; BMI, body mass index; LDL, low-density lipoprotein; HDL, high-density lipoprotein; MPV, mean platelet volume; MI, myocardial infarction.
a P value is for comparison between control and study population.
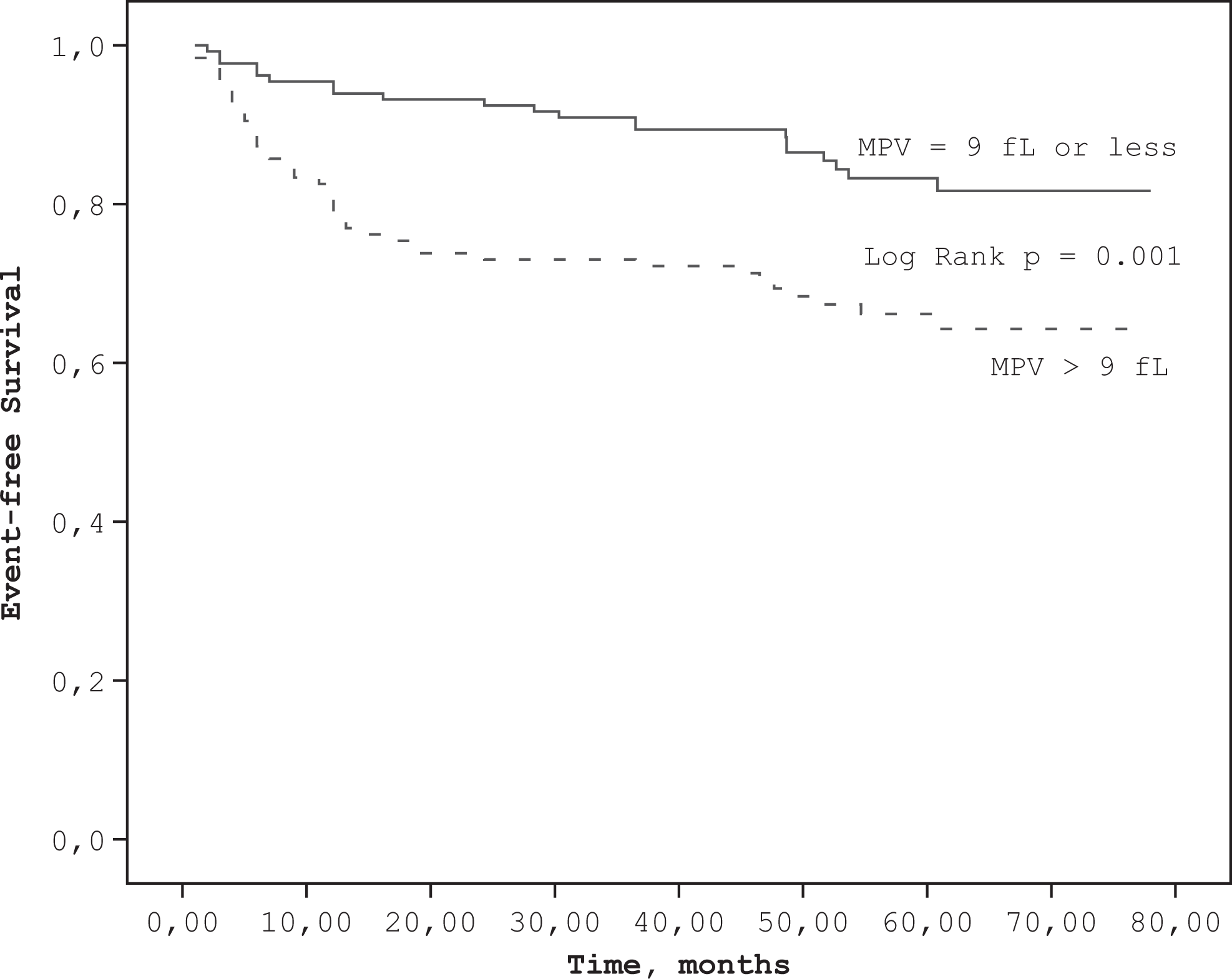
Kaplan-Meier curves demonstrate the event-free survival in patients with coronary artery ectasia by the categorized mean platelet volume (MPV) values (≤9 vs > 9 fL).
Discussion
In the present study, we investigated the prognostic role of MPV in patients with CAE. We found that MPV, an indicator of platelet activation has a prognostic role in patients with isolated CAE.
Previous studies have shown exercise-induced myocardial ischemia in patients with CAE and impaired coronary flow pattern as a possible cause of coronary insufficiency that has been accused for this. 19,20 The changes in blood viscosity, platelet activation, activation of coagulation system, and the altered flow properties of blood in ectatic segments may cause thrombosis within the ectatic segment and this may cause distal embolization to distal coronary artery.
Consequently, this may be responsible for myocardial ischemia/infarction in patients with CAE. Yasar et al showed that patients with CAE have raised levels of plasma P-selectin, β-thromboglobulin, and platelet factor 4 when compared with control group suggesting increased platelet activation in patients with CAE. 21 The platelet activation marker, MPV, was found to be elevated in patients with CAE when compared with control group. 13,14 In our previous study, we also demonstrated that MPV was elevated in 366 patients with CAE when compared with control group. 15
Increased platelet activation and aggregation are closely related to cardiovascular complications. 9 Mean platelet volume is a simple and easy method of assessing platelet function. 5 Larger platelets have a greater mass and are both metabolically and enzymatically more active than smaller platelets. 22
Recently, prognostic value of MPV in cardiovascular diseases has gained great interest. Several studies have shown that MPV has prognostic value in patients with AMI. 23–25 Patients with AMI with an elevated MPV had a significantly higher risk of death than those with a normal MPV in these studies. 23–25 Moreover, MPV was reported to be higher in patients who develop restenosis following coronary angioplasty. 26,27 Recently, a meta-analysis by Chu et al containing above studies suggested that MPV is a potentially useful prognostic biomarker in patients with cardiovascular disease. 28
Although the pathophysiology of CAE remains largely unknown, the common coexistence of CAE with coronary artery disease (CAD) suggests that it may be a variant of CAD.
Long-term prognosis and outcome in patients with CAE is unknown. In the majority of cases, CAE accompanies atherosclerotic coronary disease. 1,3 It has been previously shown that CAE does not confer an additional risk to that which is attributed to coexisting coronary stenosis. 1,3 Baman et al using a criteria for identifying patients with pure CAE, reported a significant adverse outcome among 276 patients they studied, with a 5-year mortality of 29.1%. 29 Although autopsy reports frequently document thrombus within a CAE, the true incidence of thrombotic occlusion is unknown. As a result, pure ectasia is not completely innocuous since there is an appreciable incidence of a previous MI and angina. We thought that platelet activation by means of MPV may have an important role in cardiovascular outcomes and in prognosis. As we know, there is no study investigating the effect of special biochemical or hematological marker on prognosis of CAE. To the best of our knowledge, this is the first study investigating the effect of admission MPV on cardiovascular outcome in patients with CAE. We have demonstrated that MPV has a prognostic value in patients with CAE. In this study, MPV is related only with readmission. The increased MPV has been noted in a number of patient groups with known CAD risk factors, such as smoking, diabetes mellitus, obesity, hypertension, and hypercholesterolemia, when compared with healthy controls. 30 There were no differences between clinical and laboratory parameters between patients with MACEs and without MACEs except age. We also found that platelet count was significantly higher in low MPV group than in high MPV group showing inverse relationship. Platelet volume is mainly determined in the bone marrow. It is supposed that the large platelets are caused by a reduced fragmentation of megakaryocytes. Mean platelet volume has been shown to inversely correlate with the total platelet count, which could even suggest the consumption of small platelets and a compensatory production of larger reticulated platelets. 31
We suggested that patients with CAE with high admission MPV have higher risk of thrombosis and consequently have higher risk of cardiovascular adverse events. By looking at the admission MPV value, we can estimate the long-term risk of patients with CAE. Mean platelet volume may have a role in guiding therapy in this respect. Some authors have suggested that antiplatelet therapy may be useful in the preservation of left ventricular function in patients with CAE. 32 However, the role of antiplatelet therapy has not yet been evaluated in prospective randomized studies. Further studies are required in this area.
Study Limitation
First, MPV was measured in dipotassium EDTA tubes in this study. Mean platelet volume increases over time in EDTA-anticoagulated samples and this increase was shown to be proportional with the delay in time between sample collection and laboratory analysis. 33 The recommended optimal measuring time of MPV is 120 minutes after venipuncture. 34 In our laboratory, time interval between blood sampling and MPV measurement is less than 1 hour. So, we minimized the EDTA-induced platelet swelling effect. Second, our analysis was based on a simple baseline determination at single time point that may not reflect the patient status over long periods.
In conclusion, admission MPV is an independent predictor of cardiovascular outcome. Apart from prognostic value, MPV may also carry further practical therapeutic implications.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.