
Abstract
Epistaxis, superficial and deep hematomas, hemarthrosis, gastrointestinal bleeding, hematuria represent the most frequent hemorrhagic events in congenital coagulation disorders. Occasionally, bleeding manifestations occur in unusual sites or are peculiar. A clotting defect may alter the clinical aspect of skin conditions or infections (hemorrhagic scabies or varicella). Hemobilia may occur as a complication of transjugular liver biopsy in hemophilia or Bernard-Soulier syndrome. Hemarthrosis of small joints of feet and hands occur in patients with hemophilia treated with protease inhibitors. Intramedullary hematomas of long bones have been described in α2-plasmin inhibitor or fibrinogen deficiencies. Spleen fracture with consequent hemoperitoneum has been reported in patients with fibrinogen deficiency. Rectus muscle sheath hematoma may occur in patients with factor VII (FVII)or FX deficiency. Acute or subacute intestinal obstruction may be caused by intramural wall hematomas in hemophilia and von Willebrand (vW)-disease. Physicians should always keep in mind that a congenital hemorrhagic disorder may cause bleeding in any tissue of the body and therefore alter the normal clinical features of a given disease.
Introduction
Ecchymosis, superficial and deep hematomas, gastrointestinal (GI) bleeding, epistaxis, hematuria, hemarthrosis, and cerebral hemorrhage are the most frequent bleeding manifestations seen in patients with congenital bleeding disorders. These bleeding manifestations can be seen in almost every clotting defect.1–5 However, it is well known that some bleeding manifestations are more frequent in a given condition as compared to others. So the hemophilias are usually associated with hemarthosis, whereas patients with von Willebrand (vW) disorder present more frequently mucosal and GI bleeding. Occasionally, in some patients rare bleeding manifestations are seen, which may be overlooked in their significance. These rare bleeding manifestations usually involve the site of bleeding and, sometimes, even the form of bleeding.
The purpose of this article is to evaluate the significance of peculiar bleeding manifestations reported in known congenital clotting disorders.
Patients and Methods
Articles dealing with bleeding manifestations in patients with congenital bleeding disorders published during the past 30 years were gathered by a Pub Med search. Original articles, regardless of the language, were obtained with the help of Pinali Medical Library of our University and through the courtesy of Acta Med, Sorengo, Switzerland.
Cross-checking of references was carried out in order to obtain a thorough evaluation even of the cases published before the search limits. Personal files concerning approximately 2000 patients diagnosed and followed in Padua during the past 40 years were also reevaluated.
Unusual or rare bleeding manifestations were then classified according to the coagulation disorder being dealt with. Both spontaneous and secondary hemorrhagic manifestations were recorded. The secondary causes (trauma or other), if present, were always indicated. The presence of the associated conditions or diseases at the time of the peculiar bleeding episode was also evaluated.
These were fibrinogen defects; factor II (FII) deficiency; FV deficiency; FVII deficiency; hemophilia A; hemophilia B; FX deficiency; FXI defect; FXIII defect; combined FV and FVIII disorder; combined FII, FVII, FIX, and FX deficiency; combined FVII and FX, α2-plasmin inhibitor; antiplasmin deficiency; plasminogen activation inhibitor deficiency; and platelet disorders.
Results
The following peculiar and unusual bleeding manifestations were found for the single coagulation disorder.
Fibrinogen Deficiency
Common bleeding manifestations in afibrinogenemia are bleeding from umbilical stump, cerebral, hematomas, menorrhagia, and epistaxis. On the contrary, osteoarticular bleeding is rare. Furthemore, hemarthrosis usually do not cause the severe arthropathy seen in patients with hemophilia. 6
Apparently, only very few peculiar bleeding manifestations have been reported. One of them refers to a rupture of the spleen with consequent massive hemoperitoneum. This has been reported in several cases of afibrinogenemia, and it is maintained to be fairly typical of the defect.4,6–8 It may be posttraumatic or even, apparently, spontaneous. The persistence of a patent processus vaginalis may occasionally cause, in males, hematocele with consequent painful swelling of left testicle.
Prothrombin Deficiency
Usual bleeding manifestations are varied and often severe (cerebral, GI, muscle hematomas, ecchymosis, epistaxis, menorrhagias, and hemarthrosis). An unusual bleeding manifestation has been reported by Lee et al in a 14-month-old patient with prothrombin deficiency (prothrombin level 6% of normal) and scabies. 9
The coexistence of the 2 conditions was responsible for a hemorrhagic form of scabies characterized by bullous hematomas of the left palm with intermittent oozing of blood. Topic treatment with benzyl benzoate together with a prothrombin complex concentrate (PCC) was effective. Another peculiar bleeding seen in a patient with congenital prothrombin deficiency was hemospermia. 10 The patient was a 36-year-old man with a prothrombin activity, regardless of its assay system of about 5% to 8% of normal. Prothrombin antigen was less than 10%. He had noticed bloody sperm on 3 occasions during a 1 month period. His wife was the only partner and he denied any sexual excess. Rectal examination and prostate sonography were negative. Urinary cytology and prostate antigen were also normal. A condom test (direct examination of sperm contained in a condom after sexual activity) was positive on 2 occasions. Symptoms subsided spontaneously with rest and sexual abstinence. No transfusion therapy was needed.
Factor V
Bleeding in FV deficiency is varied: easy bruising, ecchymosis, muscular hemathomas, epistaxis, hematuria, gum bleeding, and menorrhagia are the most frequent manifestations, but hemarthrosis is rare.
A rare bleeding manifestation is represented by intraperitoneal bleeding due to a ruptured follicle at the time of ovulation. This is a severe bleeding manifestation that requires prompt diagnosis and treatment. Oral contraceptives have been shown to be very effective and are the treatment of choice. 11 Another peculiar bleeding manifestation has been described in a young soldier who had varicella. 12 The vesicles became bloody, evolved in a bloody crust but left no scar. The patient was stationing in Padua and was not known to have FV deficiency even though he had presented occasional epistaxis and easy bruising.
Factor VII Deficiency
There are no typical bleeding manifestations for FVII deficiency: epistaxis, hematomas, hemarthrosis, menorrhagia, and easy bruising have all been described.
A rare hemorrhagic manifestation is represented by rectus muscle sheath hematomas (RMSHs). 13 This may occur spontaneously or after a trauma, even a mild one. If promptly diagnosed and treated, the condition evolves well. On the contrary, if the diagnosis is delayed and the hematoma has become large, the danger of an intrabdominal compression syndrome is to be envisaged.
Bloody tears have been reported in at least 1 case. 14 This was a 3-month-old male infant who also had intracranial bleeding and bleeding from the right external ear channel.
Factor VIII and Factor IX Deficiencies
As thoroughly known, patients with hemophilia may bleed in many districts, but hemarthrosis represents the most typical bleeding manifestation. Cerebral hemorrhage, superficial and deep muscles hematomas, hematuria, and GI bleeding are also common. There are no clinical differences between the 2 hemophilias.
Unusual site bleedings are rare, probably because all the attention is concentrated on major bleeding episodes. However, since patients with hemophilia A or B represent, excluding vW disease, at least 80% of all bleeding disorders, it is not surprising that most reports deal with these 2 conditions. Isolated hematoma in the liver has been reported in a few neonates with hemophilia A.15,16 Hepatic bleeding may be subdivided into 3 types, namely parenchimal hematoma, subcapsular hematoma, and hemolilia. All these forms of bleeding have been described in hemophilia A patients. Parenchimal hematoma has been described mainly in infants or young boys. Subcapsular hematomas, which may be associated with parenchymal hematoma, are usually secondary to liver biopsy. 17 Right upper quadrant pain, nausea, vomiting, fever are the most frequent symptoms. Sonography, computed axial tomography (CAT), and magnetic resonance imaging (MRI) are fundamental for the diagnosis. Treatment is usually conservative.
Hemobilia is a rare bleeding manifestation. Abdominal pain, jaundice fever, nausea, and vomiting are the main symptoms. Stool may be hypobolic or bloody according to the prevalence of obstruction or bleeding.
The condition has been described in a few patients with hemophilia A. The bleeding was either spontaneous or after liver biopsy (both transjugular or transabdominal).17–19 Diagnosis on clinical grounds is difficult, but it should be suspected immediately when a patient with hemophilia has undergone liver biopsy. Sonography, CAT, MRI, and retrograde cholangiography are diagnostic. Treatment is usually conservative with rest, parenteral nutrition, and substitution therapy, but surgery may occasionally be needed.20–23
Contrary to what occurred for hemophilia A, liver hemorrhage has been described only rarely in hemophilia B. Whether this indicates a pathogenetic preference or is just due to the higher prevalence of hemophilia A with respect to hemophilia B remains to be clarified. Hemobilia has been described in a 70-year-old man who was subsequently found to have colangiocarcinoma. 24
Intra-adrenal hematoma has been reported in a neonate with hemophilia A and also in adults usually with inhibitors. 25 Hemophilia B was found in a patient who showed a spontaneous hemorrhage in the columella nasi. 26 Spontaneous, or apparently so, splenic rupture has been reported in hemophilia A and B.27,28 Spinal epidural hematomas are extremely rare bleeding manifestations in patients with hemophilia. They usually require a rapid surgical intervention to avoid spinal cord compression with consequent severe neurological sequels.29–32 A subperiosteal orbital bleeding was reported as the initial symptom of a patient with hemophilia B. 33
Spontaneous hyphema has been described in hemophilia B. This seems to be an extremely rare event. 34
Intramural intestinal wall hematoma is an important bleeding event. Because of the acute picture of abdominal pain, palpable mass, and even intestinal obstruction, several diagnostic problems are raised. Both CAT and MRI are of paramount importance. It may involve the duodenum or other areas of the small intestine.35–41 The treatment may be conservative with adequate substitution therapy, however, surgery is sometimes needed. The condition may be underdiagnosed since minor bleeding episodes may spontaneously subside and the event goes on to be reported as colicky pain. Occasionally, intramesenteric hematomas have been described. 42 Acute epigastric pain radiating to left hypochondrium and shoulder and palpable mass extending down from left hypochondrium are the reported signs or symptoms. 42
Hemarthrosis of small points of hands and feet have been described in patients with hemophilia with HIV infection during treatment with protease inhibitors, specially Ritanavir.43,44 This is peculiar since in patients with hemophilia large joints are usually involved. Pain, swelling, and limitations in functioning of hands and feet are most prominent signs. The condition is often associated with bleeding in soft tissues of palms and soles. Hemoptysis has been demonstrated to be rare in hemophilia and other bleeding disorders safe for terminal HIV-infected patients. 45
Mosquito bites may sometimes cause spontaneous bleeding in hemophilia or in other coagulation disorders. The lesion appears as a localized round bloody swelling. 3
Factor X Deficiency
Bleeding in FX deficiency is varied without any typical manifestations. Hematuria, menorrhagia, GI bleeding, intracerebral hemorrhage, epistaxis, and hematomas have been described. Unusual bleeding manifestations are represented by bleeding from the rupture of the follicle at time of ovulation.46,47 Similarly for what seen for FVII deficiency, at least a case of RMS hematoma has been described. 13
Factor XI
Bleeding manifestations in FXI deficiency are usually only mild to moderate. The most frequent ones occur postsurgery or postinvasive procedures. We are not aware of any peculiar and/or unusual bleeding in these patients.
Factor XIII
Bleeding from the umbilical stump has been maintained to be typical of FXIII deficiency. This is true, but not absolute, since bleeding of the umbilical stunt has been described in other diseases, namely fibrinogen deficiency, hemophilia, and vW disease.
Among the unusual manifestations, a splenic rupture has been described. Since bleeding manifestations have been described in a few patients this bleeding has been maintained to be typical of the condition. Abdominal distension, pain, tenderness, and anemia represent the typical clinical picture. 48
von Willebrand Disease
Bleeding in vWD consists mainly of mucosal bleeding, GI tract, epistaxis, menorrhagia, and postpartum hemorrhage. Hemartrosis are rare and usually limited to severe forms (type III).
Among the unusual presentation, intramural duodenal or small intestine hematomas may be listed. 37 The picture is characterized by abdominal mass, pain, and intestinal obstruction or subocclusion mimicking several forms of acute abdomen (abscess, acute appendicitis, salpingitis, etc). Intramyometrial hemorrhage has been described in at least 1 case. 49
Hemoperitoneum by rupture of the follicle at the time of ovulation and spontaneous intracholecystic hemorrhage has also been described.50,51
Combined FV and FVIII
Bleeding manifestations in this condition resemble those of a mild or moderate hemophilia. Hematuria, hemarthrosis, GI bleeding, and CNS hemorrhage seem relatively less frequent. 4 We are not aware of any peculiar or rare bleeding manifestation in this peculiar condition.
Combined FVII and FX Defects
There are 2 types of combined FVII and FX defects. The most frequent one is due to deletion or abnormalities of the distal part of chromosome 13 (13q34) site of FVII and FX genes. 52 The second form is due to the chance association with the same family of both FVII and FX defects. 53 In the latter, isolated FVII or FX defects are present in the pedigree. Apparently no specific or peculiar bleeding manifestation has been described in these conditions. In the first form, other abnormalities according to the extension of the deletion or abnormalities (mental retardation, growth retardation, craniofacial dysmorphy, etc) predominate and bleeding manifestations are mild or even absent. The level of FVII and FX activity in these patients is usually about 30% 50% of normal.
In the second chance association form, bleeding may be severe, similar to what is seen in FVII and FX deficiencies, depending on the severity of the defect but without peculiar features. 53
Combined FII, FVII, FIX, and FX Defects
Bleeding manifestations in combined FII, FVII, FIX, and FX defects are varied. The severity of the bleeding diathesis also varies from one pedigree to the other. Another peculiar feature of this bleeding condition is the frequent partial connection of the defect by vitamin K administration with consequent improvement or temporary disappearance of the symptoms. 54
α2-Plasmin Inhibitor (Antiplasmin) Deficiency
Late bleeding from incidental cuts or wounds in skin or mucosa are the most frequent bleeding manifestations.
The picture in this defect resembles a little, even though less severe, that of FXIII deficiency. Oral cavity bleeding post tooth extraction and tonsillectomy are prominent, due to a rapid lysis of fibrin hemostatic plug. 55
A peculiar and apparently typical bleeding complication of α2-plasmin inhibitor deficiency is the intramedullary hematoma in the diaphysis of long bones.56,57 Radiographs show homogeneous, hypolucent nodular lesions with regular contour. Magnetic resonance imaging is particularly useful in diagnosis. Similar lesions had been seen also in afibrinogenemia, These are the result of repeated hemorrhage, often posttraumatic, which cause destruction and attempts at the reconstruction of bone with a peripheral fibrous reaction. 58
Deficiency of Plasminogen Activator Inhibitor 1
Bleeding manifestations are varied but mild and usually postsurgery or posttrauma. Menorrhagia is frequent and sometimes important. Apparently there are no typical bleeding manifestations but there is a tendency to rebleeding after initial hemostasis. The clinical picture, even though less severe, resembles to that of FXIII deficiency . 59
In spite of the similar clinical picture of that of antiplasmin deficiency, no intramedullary hematoma has been described so far in Plasminogen activator inhibitor (PAI) deficiency. The reason for this discrepant behavior, in spite of a similarly increased fibrinolysis, is unknown.
Congenital Platelet Disorders
Bleeding diathesis in congenital platelet disorders is usually characterized by epistaxis, easy bruising, and GI bleeding.
There are few reports of peculiar bleeding manifestations. The most interesting one is hemobilia which has been occasionally reported in Bernard-Soulier (BS) syndrome.60,61 Hemobilia is more frequently seen, as we have previously discussed, in hemophilia A patient either spontaneously or after jugular vein access liver biopsy.
It is not known whether the occurrence of hemobilia in BS syndrome represents a chance association or it has a pathogenetic significance. This peculiar bleeding manifestation has never been reported in Glanzman thrombastenia.
Discussion
The significance of these rare or unusual bleeding manifestations is probably less important than that of the more frequent ones.
However, in some instances they may be the only or the initial manifestation of the disease and therefore they have a potential diagnostic significance. In general, these rare and unusual bleeding conditions are seen in patients with moderate defects. This indicates that in severe cases, the common bleeding manifestations are prevalent and concentrate most of the attention. However, this is not absolute since in FXI deficiency, usually not a severe bleeding defect, no peculiar bleeding has ever been described. This review has demonstrated that congenital bleeding disorders may present bleeding in unusual sites or bleeding with peculiar features (Table 1 ). Any disease, in these patients, may be influenced in its clinical presentation and course by the underlying bleeding disorder. This is particularly true in case of diseases with skin involvement as demonstrated by the cases of FV deficiency with bloody varicella vesicles or of prothrombin deficiency with hemorrhagic scabies lesions. This should not surprise anyone since even in acquired conditions such as severe thrombocytopenia, infectious diseases with skin involvement, for example scarlet fever, may assume a bloody aspect.
Peculiar Clinical Observation Worth Remembering a
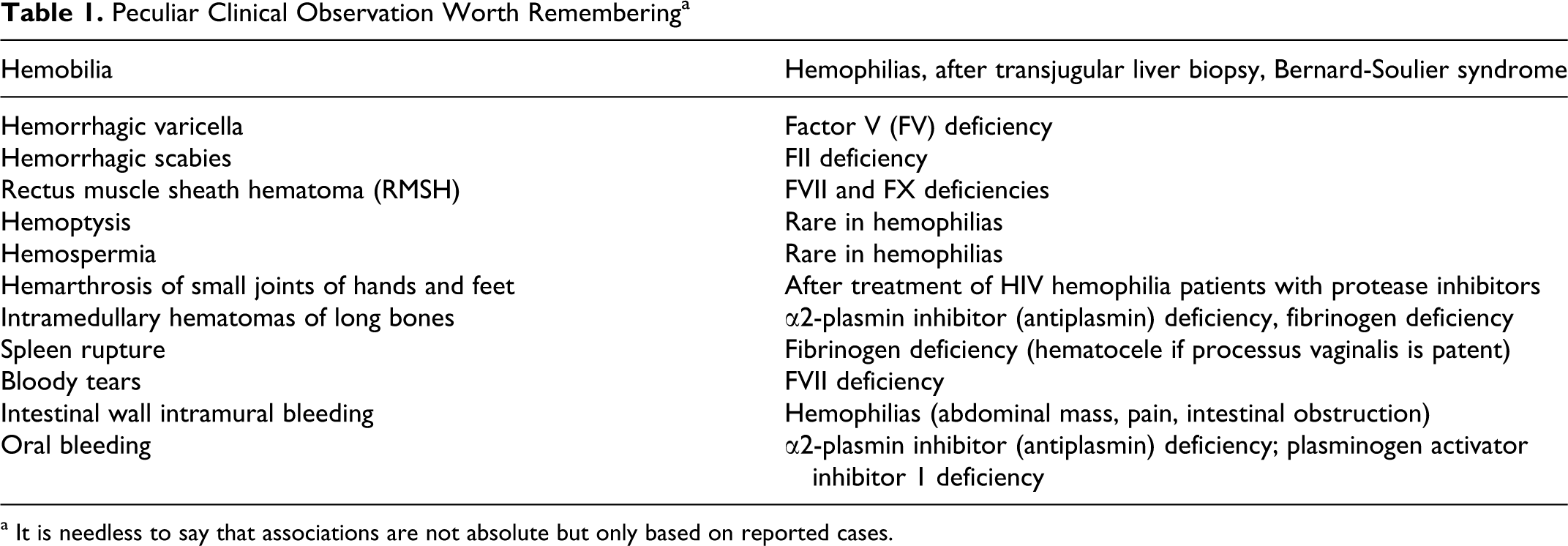
a It is needless to say that associations are not absolute but only based on reported cases.
The correct approach is to assume that any peculiar sign or symptom in patients with congenital bleeding disorders may always be attributed to their bleeding condition till proven otherwise. This is particularly true in case of acute or subacute abdomen secondary to the rupture of follicle at the time of ovulation. In this case, before reaching the correct diagnosis, several causes of acute abdomen may be taken into consideration (appendicitis, salpingitis, volvulus, etc)
The same is true for the intestinal occlusion or subocclusion secondary to intramural hematomas of intestinal wall. The condition, once promptly diagnosed by sonography, CAT, or MRI, can be conservatively managed with adequate substitution therapy, thereby avoiding surgical procedures. The RMSH is usually seen during subcutaneous heparin therapy or during oral anticoagulation, whereas it is rare in congenital bleeding disorders. This is another example of bleeding manifestation that, once promptly suspected on clinical grounds can be easily confirmed by sonography or CAT. Conservative treatment with adequate substitution therapy may avoid severe complications such as an abdominal compression syndrome and consequent surgical procedures.
The purpose of the study was not to establish the frequency of these rare bleeding manifestations but to underline the significance of an adequate evaluation of bleeding and clotting disorders in clinical practice.
Footnotes
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: in part by “Associazione Emofilia ed Altre Coagulopatie delle Tre Venezie”