
Abstract
Pseudothrombocytopenia (PTCP) is a laboratory event of platelet clustering related to drugs used for anticoagulation. This condition is engendered by autoantibodies against platelets in usually EDTA-anticoagulated blood. Pseudothrombocytopenia has no clinical significance but when evaluated as true thrombocytopenia, this misconception may lead to unnecessary diagnostic procedures. Heparin-induced thrombocytopenia with thrombosis (HITT) is a complication of heparin treatment caused by heparin platelet factor 4 (HPF-4) antibodies, leading to platelet activation and hypercoagulability. In our study, 48 patients with PTCP and 36 healthy volunteers were included. Heparin platelet factor 4 antibody positivity was detected in 12 patients from PTCP group; nobody from control group had. Citrated serum samples and peripheral blood smears showed normal platelet count. Of the 4 patients using heparin derivative, 1 (2.1%) had antibody positivity but without any bleeding symptoms. In conclusion, HPF-4 antibody positivity might be a risk factor for PTCP. Clinicians should be aware of this kind of condition.
Introduction
Pseudothrombocytopenia (PTCP) is a consequence of anticoagulant-induced platelet agglutination that causes extremely low platelet counts. Although some anticoagulants like citrate, oxalate, and heparin have been pronounced as causing platelet clumps,1,2 this condition usually occurs in the presence of EDTA agglutination. The diagnosis of PTCP is based on the peripheral smear of the freshly drawn blood without using any anticoagulants. Incidence of EDTA-dependent PTCP is approximately 0.1% in general hospital practice. 3 This phenomenon is usually transient but may persist for years 4 and not an indicator of any hemorrhagic disorder, platelet function abnormality, and thrombosis. Although this laboratory result is devoid of any significant importance, misdiagnosis of PTCP leads to unnecessary diagnostic tests and unwarranted exposure to transfusion and related complications. 5
Heparin-induced thrombocytopenia with thrombosis (HITT) is a dangerous complication of heparin treatment which causes arteriovenous thromboembolism. This condition is suspected if apparently decreased platelet count is observed in 5 days or more after initiation of heparin derivatives. Accurate diagnosis is based on exclusion of other disorders. This condition is managed by stopping heparin and anticoagulation based on nonheparin drugs. This complication seems to be related to an antibody-expanding platelet activation at the milieu of heparin treatment.6,7 These antibodies are called as antibodies to heparin platelet factor 4 (HPF-4) complex which are specific to the heparin and platelet factor 4(PF-4) complexes.
Platelet factor 4 is a basic protein found in alpha granules of platelets. This antibody complex interacts with Fc receptors on platelets and, by this way, induces platelet activation. This event is important in the etiology of thrombotic complications of HITT. 8 The diagnosis of HITT is based on clinical and laboratory examination. Detection of HPF-4-induced antibodies can be achieved by functional and antigenic tests. Antigenic assays such as enzyme-linked immunosorbent assay (ELISA) can detect heparin-PF4-induced antibody (HPF-4-ELISA) levels with a sensitivity of 90%.
Although ELISA is an easy and useful assay for the detection of HPF-4 antibody, which is generally preferred for the initial diagnosis of HITT, 9 false positivities are also possible. Cardiovascular surgeries and diseases with antiphospholipid antibodies 10 are potential for false positivity of the HPF-4 antibody. Also it has been implicated as an independent predictor for myocardial infarction after coronary ischemic syndromes. 11 On the other hand, some antibody-dependent conditions may show cross-reaction and can be confused at diagnosis. The objectives of this current report were to study the coincidence of HPF-4 positivity and PTCP and observe the relationship between HPF-4 positivity and some clinical conditions and medications.
Materials and Methods
The study was conducted at Fatih University Medical School Hospital, Ankara, Turkey. Forty-eight patients (34 women and 14 men; mean age of 53.8), with the diagnosis of PTCP, and 36 age-matched healthy controls (23 women and 13 men; mean age of 43.2), were included in this study. The control group consisted of individuals with normal platelet count and had no disorder causing bleeding. Patient group consisted of participants with low platelet count at EDTA anticoagulated blood, but they have normal values at peripheral blood smear. Platelet values were also normal when citrate coagulated tube is used to study complete blood count.
Informed consent was obtained from each patient and the study protocol conforms to the ethical guidelines of the Declaration of Helsinki as reflected in a prior approval by the Instution’s ethical human research committee. The local ethic committee of Fatih University approved this study.
Blood samples were collected from patients and control group after an overnight fasting. Complete blood count, iron, iron-binding capacity, transferring saturation, thyroid-stimulating hormone (TSH), vitamin B12, and folate were studied. First, complete blood count of every participant was studied with EDTA-coagulated tube; but blood samples of the patient group were analyzed with citrate coagulation after detecting low platelet counts.
Peripheral blood smear of each patient was also assessed. After preparing the blood smear, Giemsa stain was used for staining the smear materials.
Prothrombin time (PT), activated partial thromboplastin time (aPTT), and international normalized ratio (INR) were tested on a CA-7000 automatized coagulation analyzer (Sysmex Ltd, Milton Keynes, UK) using recombinant reagents, Innovin and Actin-FS, respectively (Dade Behring, Marburg, Germany).
Antinuclear antibody (ANA) tests were performed for each participant using ELISA and results were reported as a titer with a particular type of immunofluroscent pattern (when positive). Low-level titers are considered negative, while increased titers, such as 1:320, are considered positive and indicate an elevated concentration of antinuclear antibodies.
Anticardiolipin antibodies (ACAs) and immunoglobulin M (IgM) and IgG were studied using Aeskulisa Prothrombin-GM (AESKU. Diagnostics., Wendelsheim, Germany). Plasma samples diluted 1:100 were applied into micro-wells of an ELISA-plate coated with human native prothrombin antigen. Patients’ antibodies, if present in the specimen, were bound to the immobilized antigen during an incubation time of 30 at room temperature. After a washing step anti-human immunoglobulin-peroxidase conjugate was incubated for 15 minutes. Following a second washing step, the peroxidase substrate, tetramethylbenzidine containing hydrogen peroxide was added. After stopping the reaction by 1 M hydrochloric acid, optical density was measured at 450 nm and corresponding concentrations were calculated by using a standard curve. Normal serum values of ACA-IgM was accepted as 0 to 15 MPL/mL and 0 to 15 GPL/ml for ACA-IgG.
Quantitative measurements of antibodies to human platelet factor 4 were performed using Human Platelet Factor 4 ELISA kit (American Diagnostica Marka, UK).
The diagnosis of PTCP was based on the observation of low platelet counts without signs of bleeding in patients; when citrate is used as anticoagulant, platelet counts were detected within normal ranges in participants. Also the diagnosis is confirmed by peripheral blood smears with normal platelet count. Patient group had no known bleeding diathesis and any disease make predisposition to bleeding.
Exclusion criteria were defined as acute viral infections like rubella, measles, Epstein-Barr virus infections, undergoing any chemotherapy and radiotherapy, B12 and folate deficiency, diseases causing thrombopenia related to autoantibodies such as systemic lupus erythematosus, antiphospholipid syndrome, idiopathic thrombocytopenic purpura, sepsis, complicated pregnancies, pregnancy with a known history of bleeding, usage of heparin derivatives with complications of bleeding.
All statistical analyses were carried out using Statistical Package of Social Sciences (Version 15.0 for Windows; SPSS, Inc, Chicago, Illinois). The relationship among variables was analyzed using Spearman correlation test. The normality of variables was evaluated by performing the Shapiro-Wilk W test. The continuous variables between the 2 groups were compared with Mann-Whitney U test. For all statistical analyses, P values less than .05 were considered statistically significant.
Results
A total of 48 consecutive patients with PTCP were included in the study. Outcomes were compared with those of 36 healthy volunteers. Demographic and clinical features of participants are documented in Table 1 .
Clinical and Demographic Features of Patient and Control Groups
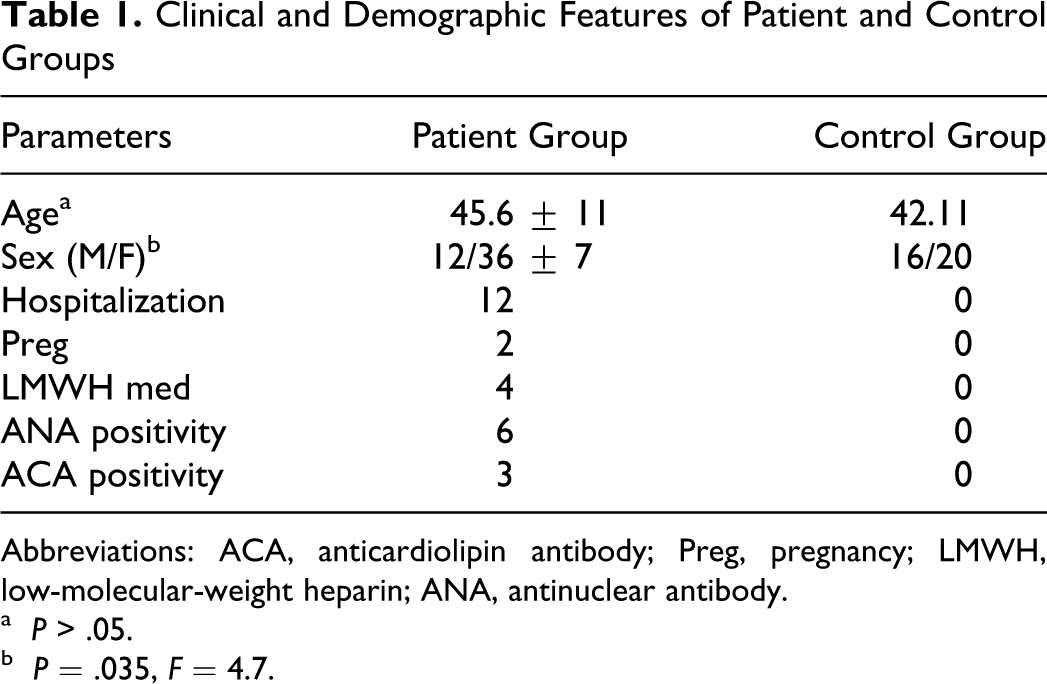
Abbreviations: ACA, anticardiolipin antibody; Preg, pregnancy; LMWH, low-molecular-weight heparin; ANA, antinuclear antibody.
aP > .05.
bP = .035, F = 4.7.
Serum mean corpuscular volume (MCV) values of red blood cells were significantly lower in antibody-positive group when compared to control and antibody-negative ones.(P < .05; Table 2 ). Serum iron-binding capacity is higher and also ferritin values were lower at antibody-positive group, but the difference was not statistically significant (P > .05). All laboratory results are compared at Table 2.
Comparison of Some Blood Parameters With Antibody Positivity
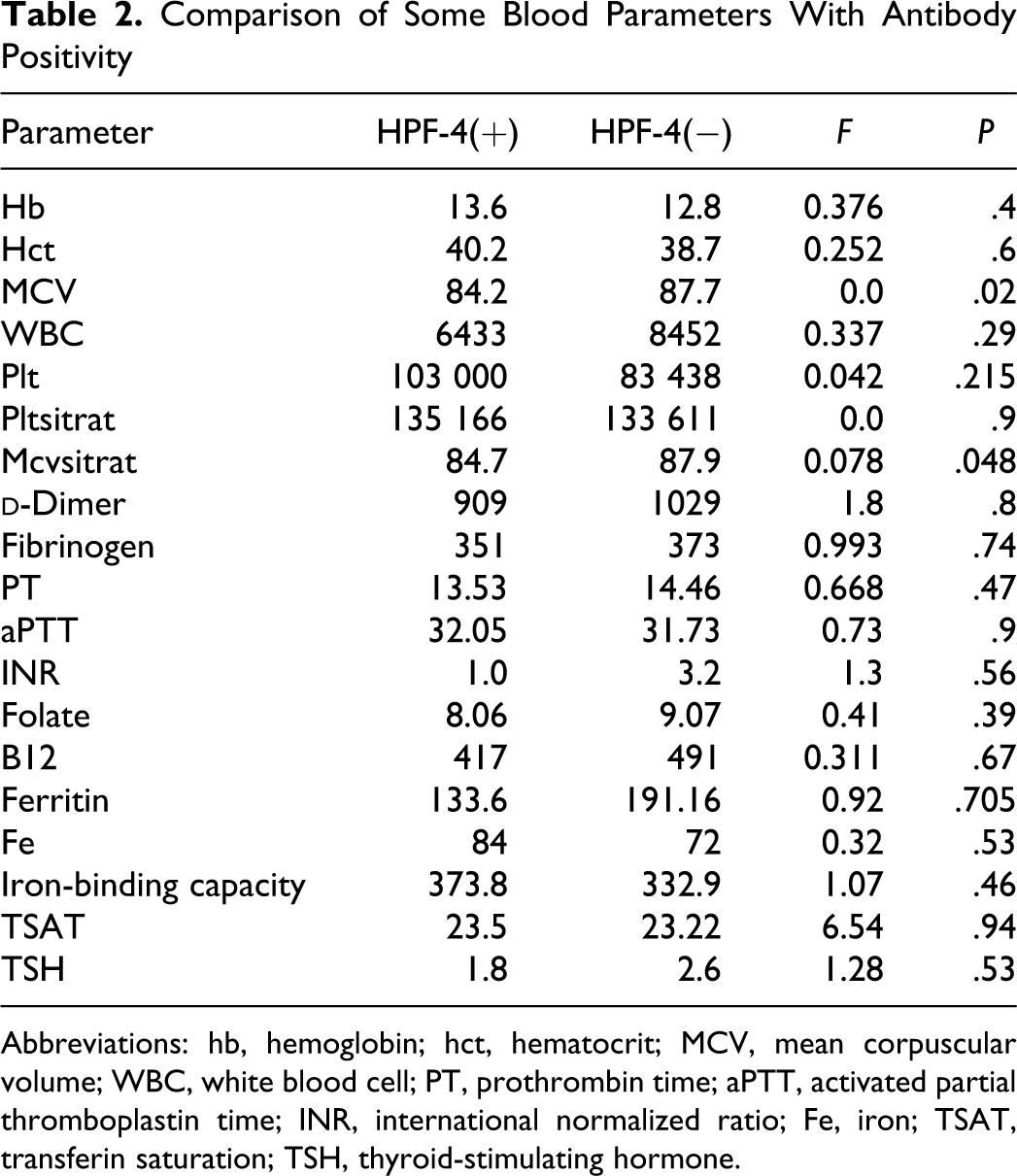
Abbreviations: hb, hemoglobin; hct, hematocrit; MCV, mean corpuscular volume; WBC, white blood cell; PT, prothrombin time; aPTT, activated partial thromboplastin time; INR, international normalized ratio; Fe, iron; TSAT, transferin saturation; TSH, thyroid-stimulating hormone.
Plasma aPTT and INR values were within normal ranges in both PTCP and control groups. There was no statistically significant difference between our groups at these parameters (P > .05).
Antibodies to HPF-4 values were significantly higher at PTCP compared to control group (P < .001). Women in patient group predominantly had more antibody positivity when compared to those of men (28.7% in men and 71.1% in women). None from the control group showed antibody positivity. In all, 12 participants from patient group had antibody positivity. Existence of HPF-4 was not significantly associated with ANA, ACA positivity, and low-molecular-weight heparin medication (P > .05). Comparison of antibody positivity with other factors is shown in Table 3 .
Comparison of Some Clinical Features With Antibody Positivity
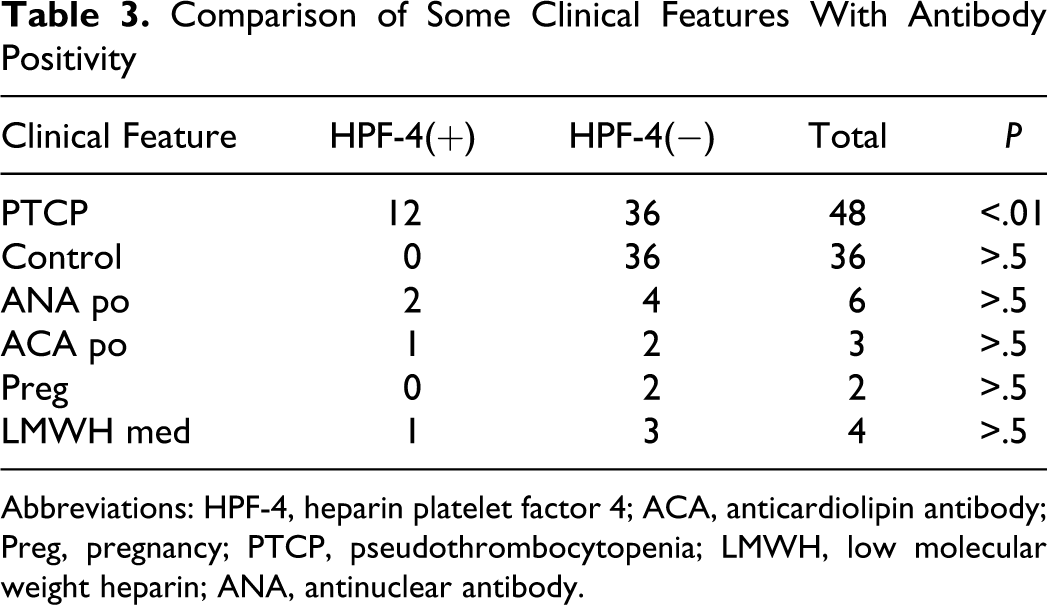
Abbreviations: HPF-4, heparin platelet factor 4; ACA, anticardiolipin antibody; Preg, pregnancy; PTCP, pseudothrombocytopenia; LMWH, low molecular weight heparin; ANA, antinuclear antibody.
Discussion
Pseudothrombocytopenia is an in vitro condition, which is caused by antibodies inducing platelet aggregation when EDTA is used as an anticoagulant for assessing complete blood count. If apparently low platelet count is obtained, platelet count can be studied again using other anticoagulants. Evaluation of a freshly prepared blood smear is an ideal method to diagnose PTCP. Despite citrate or heparin- induced platelet clumping is observed,12 platelet count is usually observed as normal when these anticoagulants are used instead of EDTA.
Platelet clumping is caused by Igs both IgM and IgG type in the serum. These antibodies reacts like cold agglutinins as they are reactive at room temperature and not at 37°C. 13 It is interestingly observed that temperature-independent IgM type antibodies are detected in PTCP with all anticoagulants used. 14 Also in a case report, they observed a patient in whom PTCP was detected before multiple myeloma had been diagnosed and PTCP was discussed as an associated condition of multiple myeloma. 15 In spite of these data, PTCP is not considered devoid of any clinical importance and not related to the any medication.
Heparin-induced thrombocytopenia is an event presented with complications of severe thrombocytopenia due to the administration of heparin or its derivatives. When thrombosis is identified, this condition is pronounced as HITT. Formation of antibodies to HPF-4 complexes and their platelet-activating effect is the main mechanism of disease. If thrombosis is observed or platelet count rapidly falls in a patient using heparin, HITT must be confirmed with specific antibody tests. 16 If the diagnosis is correct, heparin must be stopped and never used for the same patient anymore.
We reported 25% HPF-4 positivity at patient group diagnosed as PTCP. These participants were not diagnosed with HITT and any autoimmune condition. One of the 4 patients medicated with low-molecular-weight heparin showed significant absorbance at ELISA tests, but the participant had PTCP when evaluated with peripheral blood smear and did not have any symptoms of bleeding. Nobody from control group had antibody positivity. Antibody positivity was not significantly associated with pregnancy and any bleeding history. Also ANA and ACA antibody-positive patients had HPF-4 complex but coexistence of them was not statistically significant. As all are autoimmune markers, these antibodies were observed as significantly higher positive in women when compared to men in the patient group.
The existence of HPF-4 with PTCP is not well recognized with large clinical studies anymore. Schwarzinger et al reported HPF-4 positivity at 2 PTCP patients and they hypothesized that in some events; IgM type anti-PF-4 antibodies can aggravate EDTA-dependent PTCP. 17 In another study including 9 patients with EDTA and citrate-dependent PTCP, 88% of patients (n = 8) showed HPF-4 antibody positivity. Antibody was not observed at any of the 6 patients with EDTA-dependent PTCP. It was considered that patients with PTCP have citrated plasma agglutinating antibodies that are similar in immunogenity to HPF-4. These antibodies cross-react and miscount HPF-4 complexes. 18
Heparin-induced thrombocytopenia with thrombosis diagnosis is usually evaluated with ELISA-HPF-4 antibody positivity in clinical practice. But the diagnosis of HITT is primarily based on the exclusion of other reasons causing bleeding and thrombosis. Because the HPF-4 antibody tests have some false positivity, diagnosing HITT and discontinuation of heparin due to antibody positivity may lead to unnecessary diagnostic and therapeutic changes and overtreatment. Therefore, if thrombocytopenia occurs in patients receiving heparin therapy, PTCP must be ruled out before considering HITT.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article