
Abstract
It has been speculated that the atypical clinical presentation of acute pulmonary embolism (PE) in older patients leads to a late diagnosis and therefore contributes to a worse prognosis. Therefore, we prospectively evaluated the delay in diagnosis and its relation to the in-hospital mortality in 202 patients with acute PE. Patients >65 years presented more often with hypoxia (P = .017) and with a history of syncope (P = .046). Delay in diagnosis was not statistically different in both age groups. Older age was significantly associated with an increased risk for in-hospital mortality (OR 4.36, 95% CI 0.93-20.37, P = .043), whereas the delay in diagnosis was not associated with an increase of in-hospital mortality. We therefore conclude that the clinical presentation of acute PE in older patients cannot be considered as a risk factor for late diagnosis and is not responsible for their higher in-hospital death rate.
Introduction
Morbidity and mortality of acute pulmonary embolism (PE) increase with age. The annual incidence for patients younger than 65 years was reported to be 17 / 1 00 000 rising steadily with age up to 112 / 1 00 000 and 157 / 1 00 000 for patients aged 65 to 74 years and 75 to 84 years, respectively. 1 Patients older than 65 years with acute PE carry a substantial risk of death with in-hospital mortality rates between 2% and 21% in previous reports.2–5
Several earlier studies found that the clinical presentation of older patients with acute PE may be atypical, potentially leading to a delay in diagnosis and initiation of treatment.6–10 Selecting the right diagnostic and therapeutic strategy based on the clinical presentation is of utmost importance, because unrecognized PE can be fatal. Previous investigations have shown that outcomes of patients with delayed diagnosis of PE are worse 11 and death rates are highest in undiagnosed cases. 12 Autopsy studies revealed that the post-mortem diagnosis of PE was significantly more frequent in older patients. 13 Since early initiation of sufficient anticoagulation therapy seems to be able to reduce the in-hospital death rate in acute PE, 14 some authors conclude that the atypical clinical presentation with a potential delay in diagnosis possibly contributes to the worse prognosis of older patients presenting with acute PE. 10
Delay in diagnosis has been incompletely investigated in acute PE and it is not clear whether it is age-dependent. Therefore, our study investigates the delay in diagnosis and its relation with in-hospital mortality in younger and older patients admitted to our hospital with the diagnosis of acute PE.
Methods
Study Population and Delay in Diagnosis
In this single-centre study at a tertiary, academic teaching hospital delay in diagnosis was prospectively evaluated in 202 consecutive patients admitted with acute PE from December 2007 through January 2009. Data collection and analysis were conducted in accordance with current ethical standards and were approved by local authorities. Diagnosis of PE was confirmed by multidetector computed tomographic (CT) angiography or lung perfusion scan. All patients included in the study were started on a standard anticoagulation regime with unfractionated heparin or enoxaparin and subsequently phenprocoumon or long-term treatment with enoxaparin. The study population was divided into a younger (≤65 years) and an older age group (>65 years) based on numerous previous reports.2,7–10 Dyspnea, chest pain, syncope, or hemoptysis were considered as clinical features of PE. 6 Delay in diagnosis was defined as the time span between the day of symptom onset and the day of diagnosis. Time was not subdivided by the hours of the day. Delay in diagnosis more than 14 days was not considered assuming that the exact onset of symptoms could not precisely be remembered after that long time. In patients who were diagnosed on the same day on which the first symptoms occurred, delay in diagnosis was set to 0.
Patients' Characteristics
Room air oxygen saturation and blood pressure were measured immediately after admission to the hospital. The severity of the disease was graded as low-, intermediate-, or high-risk PE according to current guidelines. 15 Pulmonary embolism was considered to be recurrent when at least 2 episodes of the disease were diagnosed in a patient. Pulmonary embolism was regarded to be idiopathic when no predisposing factors (adapted from ref 16) could be evaluated. Information about earlier PE and predisposing circumstances were drawn from the medical records or were based on the patients' interview. Syncope was defined as a temporary loss of consciousness upon or following the onset of symptoms. Congestive left heart disease was considered in patients with a preexisting or newly diagnosed ejection fraction of the left ventricle of less than 40%. Uncontrolled asthma, chronic obstructive pulmonary disease, lung fibrosis, or other symptomatic interstitial lung diseases (eg, sarcoidosis) were defined as concomitant lung diseases. Creatinine was measured at the time of admission to the hospital. Serum levels >1.1 mg/dL were regarded elevated in women, values >1.25 mg/dL (age >50 years) or >1.44 mg/dL (age ≥50 years) were considered elevated in men. 17
Statistics
Statistical analysis was performed with SPSS software for Windows version 12.0 (SPSS, IBM Inc, Chicago, Illinois). Continuous variables are shown as means ± 1 standard deviation (SD). Student t-test was used for the comparison of continuous variables and the χ2 test for the comparison of nominal variables. Multiple linear regression analysis was performed to investigate predictors for in-hospital mortality and a delay in diagnosis more than 1 week and to detect potential confounding effects between the different covariates. A probability value of less than .05 was considered statistically significant, all reported P values are 2-tailed.
Results
Of 202 patients, 30 could not remember or determine exactly the time of symptoms onset. In 12 patients, delay in diagnosis was more than 2 weeks. Thus, a total of 160 patients could be included in the study. In all, 93 patients were older than 65 years; the younger age group consisted of 67 patients. The majority of patients (96.2 %) suffered from low- or intermediate-risk PE.
The time span between the first symptoms and diagnosis of PE increase with advancing age, but there was no statistically significant difference in the delay in diagnosis between the different age groups (Table 1 and Figure 1 ). A history of syncope was more frequent in patients older than 65 years (P = .046). The room air oxygen saturation of older patients was significantly lower upon presentation to the emergency ward compared with the younger age group (P = .017). Concomitant lung disease (P = .021), congestive heart failure (P < .0001), diabetes mellitus (P = .049), and an elevated serum creatinine (P = .014) were significantly more frequent in older than in younger patients. The in-hospital mortality rate was significantly (P = .043) higher among patients older than 65 years compared with younger patients.
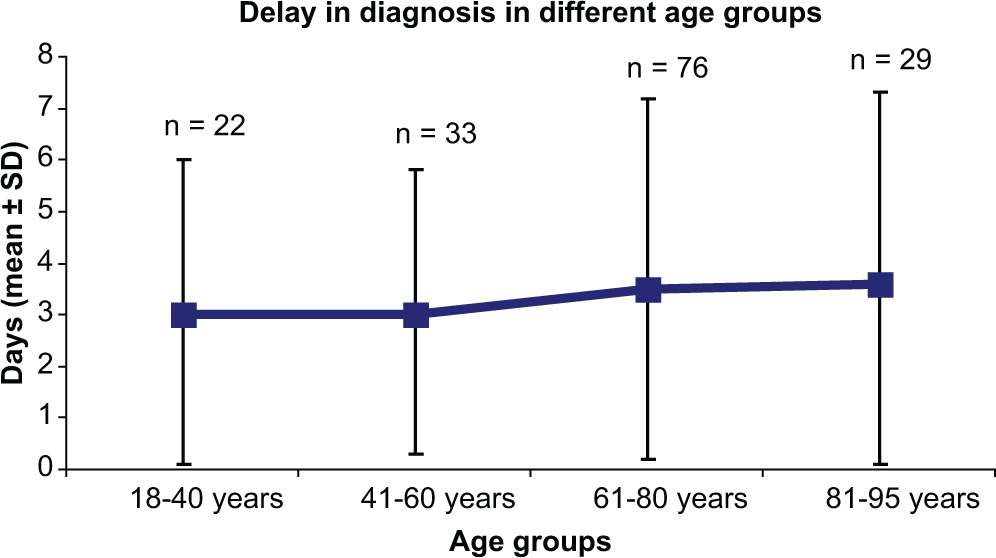
Delay in diagnosis in different age groups.
Delay in Diagnosis and Patients' Characteristics in the Younger and Older Age Group a
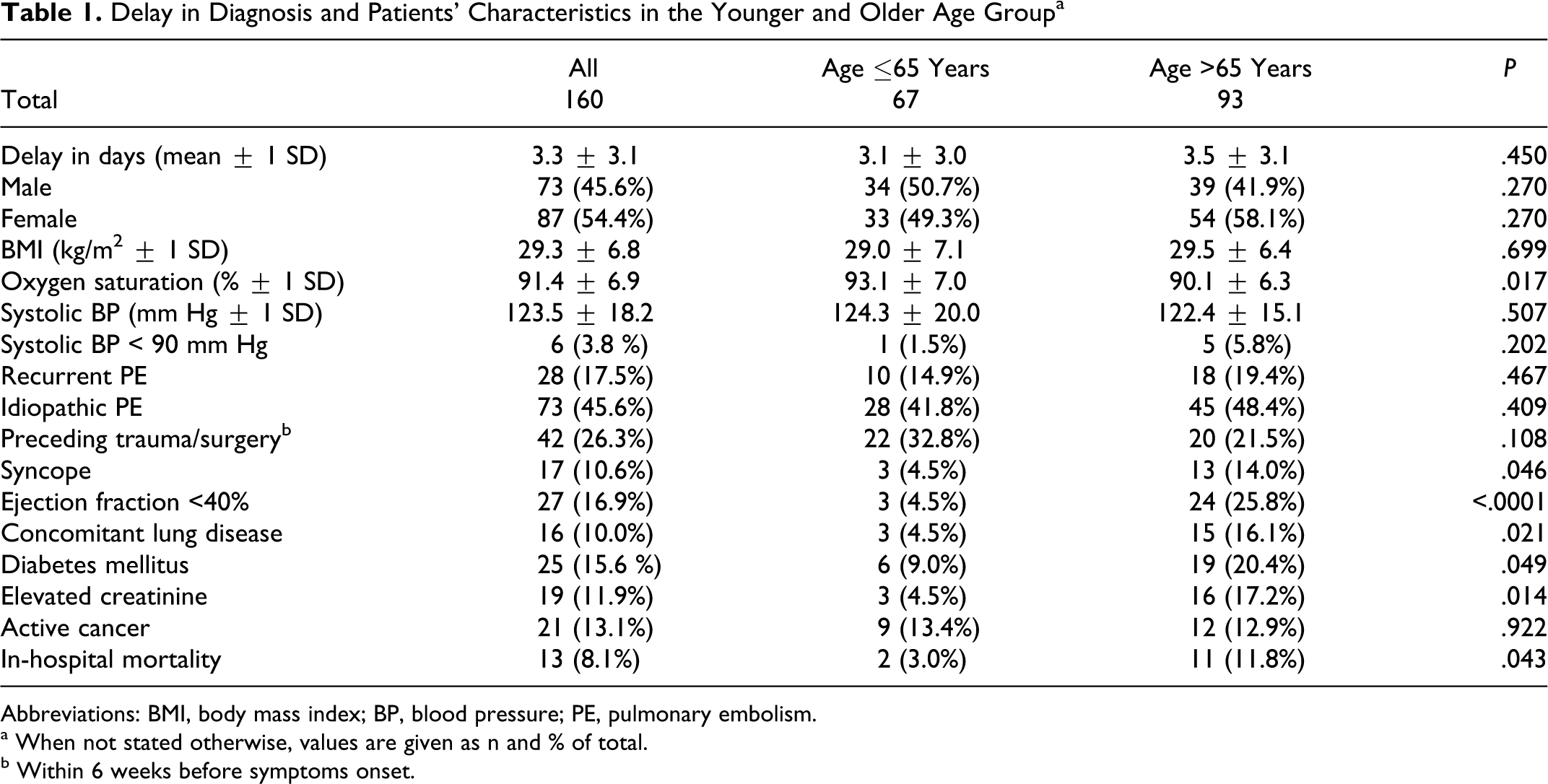
Abbreviations: BMI, body mass index; BP, blood pressure; PE, pulmonary embolism.
a When not stated otherwise, values are given as n and % of total.
b Within 6 weeks before symptoms onset.
In univariate analysis (Table 2 ), patients with recurrent PE were exposed to a significantly higher risk for a delay in diagnosis of more than 1 week (OR 3.70, 95% CI 1.20-11.43, P = .017). In contrast, multiple regression analysis fails to demonstrate that recurrent PE is an individual predictor for a prolonged delay in diagnosis. Patients who present without syncope are at increased risk for late diagnosis in univariate (OR 7.10, 95% CI 3.90-12.90, P < .0001) and multivariate analysis (P = .003). No other parameter tested (including advanced age) was identified to be a reliable predictor for a prolonged delay in diagnosis.
Predictors for a Delay in Diagnosis > 1 Week in Univariate and Multivariate Analysis
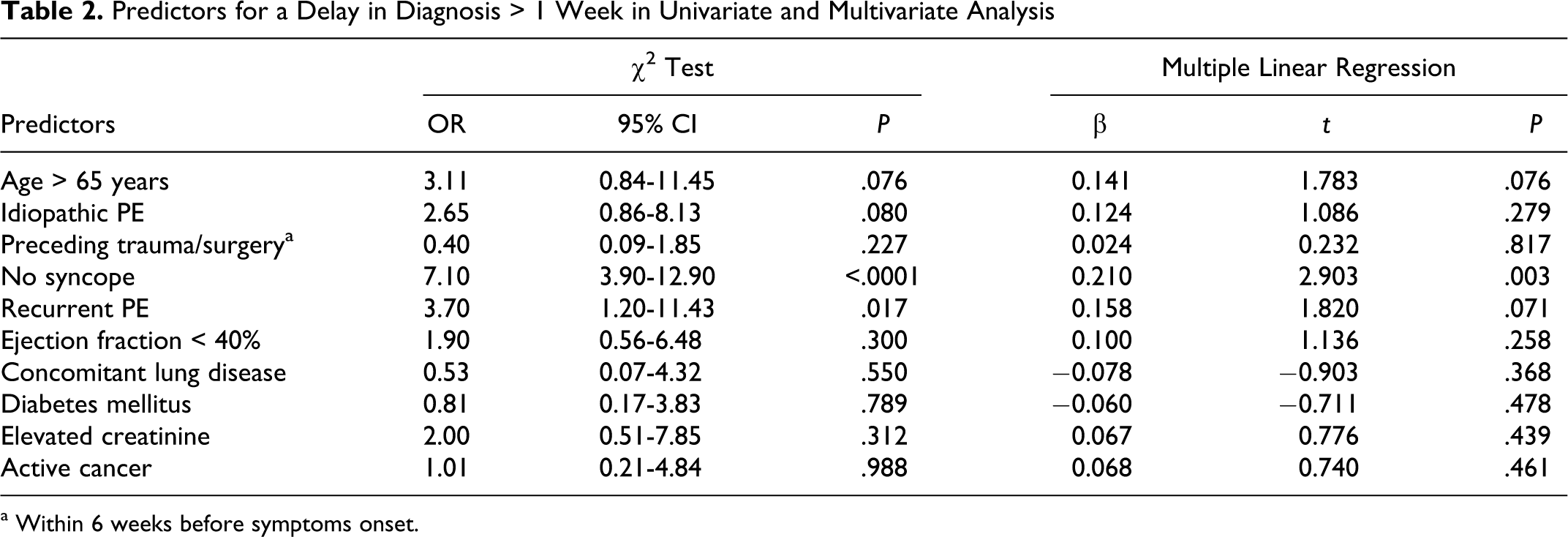
a Within 6 weeks before symptoms onset.
Advanced age (OR 4.36, 95% CI 0.93-20.37, P = .043), recurrent PE (OR 4.87, 95% CI 1.50-6.23, P = .005), a history of syncope (OR 12.36, 95% CI 3.41-44.81, P < .0001), concomitant chronic lung (OR 9.64, 95% CI 2.79-33.32, P < .0001), or congestive left heart disease (OR 16.0, 95% CI 4.46-57.37, P < .0001) as well as diabetes mellitus (OR 5.77, 95% CI 1.75-19.0, P = .002) or elevated creatinine (OR 3.91, 95% CI 1.07-14.25, P = .028) were significantly associated with an increased risk for in-hospital mortality in univariate analysis (Table 3 ). A history of syncope upon or following the onset of symptoms, recurrent PE, and congestive left heart failure were shown to be individual predictors for in-hospital death in multiple-regression analysis (P < .0001, P = .010 and P < .0001, respectively). Delay in diagnosis was not associated with an increase of in-hospital mortality in univariate or multivariate analysis.
Predictors for in-Hospital Mortality in Univariate and Multivariate Analysis
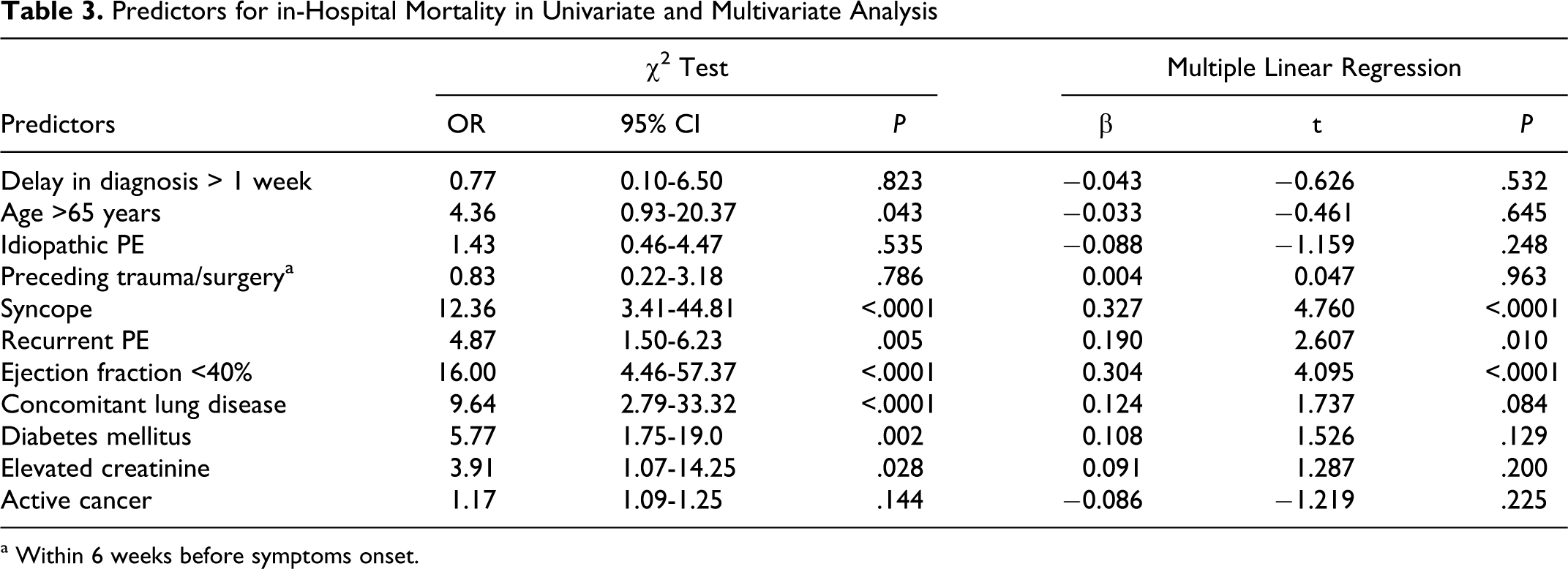
a Within 6 weeks before symptoms onset.
Discussion
The present study was conducted to test the hypothesis that the atypical clinical presentation of acute PE in older patients may lead to a greater delay in diagnosis. Secondly, we investigated whether the delay in diagnosis of acute PE is related to the in-hospital mortality.
The clinical presentation of older patients with acute PE is supposed to be subtle and atypical, since hypoxia may be the leading clinical sign and chest pain may be less frequent, whereas syncope may occur more often upon or in the course of symptoms onset. In agreement with previous studies,2,9 we found that older patients were more often hypoxic when presenting with acute PE. A higher degree of respiratory compromise due to pulmonary obstruction or the increased prevalence of concurrent heart and lung diseases in advanced age might be responsible for this observation. Consequently, dyspnea was the predominant clinical sign of PE observed in our study (data not shown). Several earlier reports revealed that chest pain is less frequent in older patients suffering from PE.8–10 It was speculated that older patients may have a reduced visceral pain sensation and perception. 18 In contrast but in agreement with other investigations,6,7,19 we found no such difference in clinical presentation between younger and older patients as most study participants suffer from both dyspnea and chest pain and were not able to clearly determine one predominant clinical symptom. In accordance with numerous previous reports,2,4,9,10 we found that a history of syncope upon or in the course of symptoms onset was more frequent among older patients, probably due to a reduced cardiopulmonary reserve in advanced age. 9 Nevertheless, the incidence observed in our study was lower compared to earlier investigations, as syncope was defined solely as temporary loss of consciousness in our study in contrast to earlier observations, where circulatory collapse was also considered to be syncope. In summary, although conducted as a single-centre study, we believe that the patients characteristics observed in our study are comparable to earlier investigations describing the clinical presentation of acute PE in older age.
Although the clinical presentation may be atypical, delay in diagnosis was not significantly different in the younger and older age group in our study. The mean delay in diagnosis in our observation and the proportion of patients with a late diagnosis (more than 1 week from symptoms onset in our study) was comparable to findings from earlier studies.20,21 Corresponding with recently published reports,11,22 we found that older patients with acute PE tend to be diagnosed later. However, these studies are not comparable to our observation in every respect. Kline et al. 11 focused on a delayed diagnostic work-up within the hospital once the patients were admitted to the emergency department. Therefore, failure to recognize PE might be more strongly influenced by local diagnostic standard than patient-related factors. Moreover, diagnosis was already considered to be late after a period of 48 hours. Thus, the proportion of patients with a late diagnosis might be overestimated compared to our investigation. In contrast to a recent study 22 we were not able to find a statistically significant difference in delays in diagnosis between the different age groups. The main reason for that might be the fact that we did not consider delays in diagnosis longer than 14 days, assuming that the exact onset of symptoms could not precisely be recalled after that long time. In contrast, 25% of the participants of the study conducted by Alonso-Martinez and coworkers 22 had a delay in diagnosis longer than 2 weeks with 10% even longer than 3 weeks. As we doubt that patients, especially those exposed to emotional and physical stress upon admission to an emergency room, are able to precisely recall the symptom onset after that long time, we questioned if the atypical clinical presentation in older patients with acute PE necessarily leads to a delay in diagnosis.
Consequently, we were not able to identify age as a risk factor for a late diagnosis in acute PE. This is in accordance with another study, in which age above 65 years could not be identified as a predictor for a delay in diagnosis of longer than 7 days. 23 We therefore conclude that there is not enough evidence indicating that advanced age is necessarily related to a greater delay in diagnosis of acute PE. The underlying causes are speculative. Assuming that symptoms like dyspnea and chest pain are possibly less often attributed to PE when cardiopulmonary comorbidity exists, 24 it is surprising that delay in diagnosis is not significantly longer in older patients, especially because we could show that concomitant heart and lung diseases are more frequent with advanced age. On the other hand, comorbidity fails to be an individual risk factor for a delay in diagnosis in our study. In agreement with a number of earlier reports,21–23 we found in univariate and multivariate analysis that patients with a history of syncope were diagnosed earlier. Syncope as a clinical sign of acute PE was more than 3-fold more common among older patients in our study. Those patients were possibly diagnosed earlier and therefore counteract the potential delay in diagnosis caused by cardiopulmonary comorbidity.
Older patients with a history of syncope, recurrent PE, or concurrent heart and lung diseases have a significantly greater risk of death during their hospital stay in our study. In contrast, delay in diagnosis was not related to the in-hospital mortality rate. This is in accordance with recent studies,22,23,25 suggesting that the delay in diagnosis of PE is not predictive for early death. However, our findings have to be interpreted with caution, because we may have missed deaths in unrecognized cases of PE. Therefore, our study does not allow the conclusion that early diagnosis and initiation of treatment is irrelevant, as undiagnosed cases of PE might have been missed. The mortality rate in our study was comparatively low, possibly reflecting the low number of patients with active cancer and high-risk PE. As we only included patients with confirmed PE by CT angiography or lung perfusion scan in our study, we possibly have missed high-risk patients who were treated urgently under the suspicion of having PE without further diagnosis. Although we believe that these are rare cases, we conclude that our findings are primarily valid for patients with low- or intermediate-risk PE.
Though our results are confirmed by a number of other reports, we acknowledge that our study has some limitations. Firstly, our data might be biased by geographical and socioeconomic factors in this single-centre study. Secondly, the sample size might be underpowered to detect rare events. Thirdly, the study only evaluated the short-term outcome and it did not test if the diagnostic delay of PE is associated with higher rates of long-term sequelae such as chronic thromboembolic pulmonary hypertension.
In summary, we suggest that the atypical clinical presentation of PE in patients older than 65 years cannot be considered as a risk factor for late diagnosis. Moreover, delay in diagnosis is not related to the higher in-hospital death rate of older patients suffering from acute PE.
Footnotes
The author(s) declared no conflicts of interest with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.